
32: Hipospádia Proximal
Este capítulo levará aproximadamente 27 minutos para ler.
Introdução
Hipospádia é definida como uma abertura do meato uretral no aspecto ventral do corpo peniano, proximal à ponta da glande. Como mencionado no capítulo anterior, a hipospádia é classificada de acordo com a localização do meato uretral em distal, médio e proximal. A variante posterior (grave), que corresponde a 20% dos casos, estende-se pelo terço proximal do corpo peniano até o períneo. Pode ainda ser subclassificada como peniana posterior (na base do corpo peniano), penoescrotal (na base do corpo peniano, à frente do escroto), escrotal (no escroto ou entre as intumescências genitais) ou, na forma mais grave, a perineal (atrás do escroto e atrás das intumescências genitais, Figura 1).1 Embora a classificação da hipospádia em distal, terço médio do corpo peniano e proximal tenha sido historicamente baseada na localização do meato no pré-operatório, a classificação correta é melhor feita no momento da cirurgia, pois a localização do meato pode mudar em função de uretra hipoplásica mais proximalmente. A hipospádia grave é frequentemente associada a curvatura ventral do pênis, conhecida como chordee, a um prepúcio “em capuz” ou incompleto e a um corpo esponjoso abortivo. Hipospadiologia, termo cunhado por John W. Duckett, Jr., é o estudo de todos os aspectos dessa condição e abrange uma disciplina em contínua evolução e expansão.2 A incidência de hipospádia é de cerca de 1:200–300 nascidos vivos nos EUA.3,4 O aumento recente da incidência pode ser atribuído à prematuridade, a recém-nascidos pequenos para a idade gestacional, ao baixo peso ao nascer e à idade materna de 35 anos ou mais.1
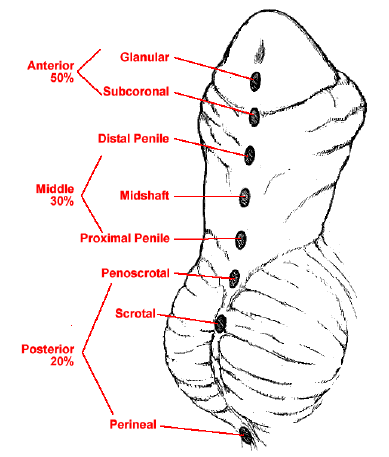
Figura 1 Espectro das apresentações da hipospádia.
Embriologia
A genitália externa masculina desenvolve progressivamente características reconhecíveis até o 3º mês de gestação. Normalmente, a abertura do seio urogenital estende-se até a face ventral do tubérculo genital, constituindo o sulco uretral. O orifício urogenital primitivo e o sulco uretral são limitados, em ambos os lados, pelas pregas uretrais.5 O tubérculo genital alonga-se para formar o falo, e as pregas uretrais começam a fundir-se a partir do orifício urogenital em direção à ponta do falo, o que resulta na formação da uretra peniana ao final da 14ª semana. Os corpos cavernosos surgem como colunas mesenquimais pareadas no corpo do pênis na 7ª semana. O corpo esponjoso resulta da diferenciação das massas mesenquimais ao redor da uretra peniana.5 Em casos de hipospádia proximal, acredita-se que haja falha na fusão dessas pregas uretrais. Devido à interrupção da tubularização, ocorre crescimento diferencial do pênis na face ventral em comparação com a face dorsal.
A compreensão da anatomia do pênis auxiliará significativamente na compreensão do reparo da hipospádia (Figura 2).
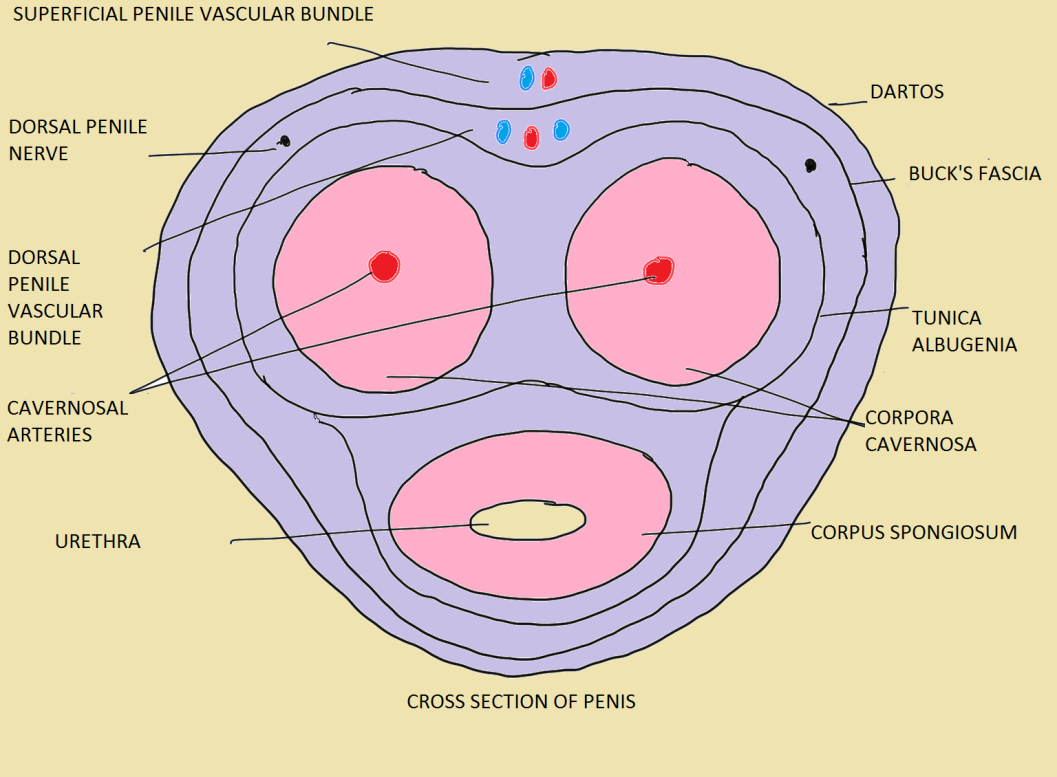 Figura 2 As camadas do pênis em um adulto normal.6
Figura 2 As camadas do pênis em um adulto normal.6
Hipospádia grave e outras condições geniturinárias associadas
Devido a uma embriopatia comum, a hipospádia proximal está mais frequentemente associada a outras condições congênitas, a saber, criptorquidia em 10% dos casos,7 hérnia inguinal em até 32% dos meninos,8 distúrbios do desenvolvimento sexual em até 27.3%9 e utrículo prostático.
Na presença de hipospádia grave e um testículo não palpável, a DSD deve ser descartada.10 Nesses casos, é imprescindível obter um cariótipo. A hipospádia escrotal por si só deve levantar suspeita de distúrbio do desenvolvimento sexual, ainda mais quando associada à criptorquidia bilateral.11 Suspeita-se de genitália ambígua em pacientes com hipospádia e gônadas impalpáveis; hipospádia com micropênis e uma ou nenhuma gônada palpável; recém-nascido com genitália externa feminina e uma massa gonadal nos lábios ou fusão labial e/ou clitoromegalia.12
Avaliação
Tabela 1 Pontos a observar ao avaliar um caso de hipospádia.6
| História | História adicional | Exame | Exame adicional |
|---|---|---|---|
| idade, criado como do sexo masculino | antecedente de mudança de voz, desenvolvimento mamário | comprimento fálico estirado | habitus (masculino ou feminino) |
| antecedente de urinar pela face inferior do pênis | antecedente de ingestão materna de hormônios durante a gestação | chordee (ausente/leve <30˚/grave >30˚) | desenvolvimento mamário (estadiamento de Tanner) |
| curvatura ventral do pênis | história familiar de hipospádia | meato (estenótico/não estenótico) | pelos axilares (presentes ou ausentes, desenvolvimento de tipo masculino ou feminino) |
| jato urinário desviado da linha média ou estreito | antecedente de perdas fetais repetidas ou doença aguda e vômitos no período neonatal | localização do meato (glandular/coronal/peniano distal/peniano médio/peniano proximal/penoescrotal/escrotal) | pelos pubianos (presentes ou ausentes, desenvolvimento de tipo masculino ou feminino) |
| antecedente de cirurgia genital | glande (arredondada/cônica) | ambiguidade de genitália externa (estadiamento de Prader em caso de DSD) | |
| testículo não descido | sulco uretral (raso/profundo) | ||
| antecedente de ereções e curvatura em adolescente mais velho | placa uretral (larga/estreita/cicatrizada/maleável) | ||
| prepúcio (capuz dorsal/adequado para reconstrução/ausente) | |||
| localização dos testículos | |||
| tamanho dos testículos | |||
| escroto (bem desenvolvido/transposição penoescrotal/hipoplásico/ponte penoescrotal) |
Além disso, o escore GMS (Glande, Meato e Corpo do pênis) parece correlacionar-se com o risco de complicações cirúrgicas. O escore GMS baseia-se no tamanho da glande/qualidade da placa uretral, na localização do meato e no grau de curvatura. Arlen et al demonstraram um aumento estatisticamente significativo na probabilidade de qualquer complicação pós-operatória a cada aumento de uma unidade no escore GMS total Tabela 2.13 Em seu estudo, 262 meninos (idade média 12.3 ± 13.7 meses) submetidos à correção primária de hipospádia apresentaram escore GMS médio de 7 ± 2.5 (G 2.1 ± 0.9, M 2.4 ± 1, S 2.4 ± 1) e seguimento clínico médio de 17.7 ± 9.3 meses. Eles observaram que 37 meninos desenvolveram 45 complicações. Observou-se uma relação significativa entre o escore GMS total e a presença de qualquer complicação (p < 0.001); a cada aumento de uma unidade no escore GMS, as chances de qualquer complicação pós-operatória aumentaram 1.44 vezes (IC 95%, 1.24–1.68).13 O desenvolvimento de fístula uretrocutânea foi observado em 21 de 239 (8.8%) reparos em estágio único e foi a complicação mais comum. Aqueles com hipospádia leve (GMS 3–6), moderada (GMS 7–9) e grave (GMS 10–12) apresentaram taxas de fístula de 2.4%, 11.1% e 22.6% (p < 0.001), respectivamente. Além disso, o grau de curvatura foi observado como preditor independente de fístula na análise multivariada. Constatou-se que pacientes com curvatura ventral >60° tinham 27 vezes mais probabilidade de desenvolver fístula do que aqueles sem curvatura (IC 95%, 3.2–229).13
Tabela 2 O escore GMS.13
| Pontuação da Glande (G) | Pontuação do Meato (M) | Pontuação do Corpo Peniano (S) |
|---|---|---|
| 1. Glande de bom tamanho; placa uretral saudável, profundamente sulcada | 1. Glandular | 1. Sem curvatura peniana |
| 2. Glande de tamanho adequado; placa uretral adequada, sulcada | 2. Sulco coronal | 2. Curvatura peniana leve (< 30°) |
| 3. Glande pequena; placa uretral estreita, alguma fibrose ou plana | 3. Meio ou distal do corpo peniano | 3. Curvatura peniana moderada (30–60°) |
| 4. Glande muito pequena; placa uretral indistinta, muito estreita ou plana | 4. Corpo peniano proximal, penoescrotal | 4. Curvatura peniana grave (> 60°) |
A avaliação da placa uretral também é importante, pois uma placa uretral estreita está associada a um prognóstico pior (Figura 3). Os dois fatores predominantes que orientam nossa decisão sobre como corrigir uma hipospádia proximal são a qualidade da placa uretral e, talvez mais importante, o grau de curvatura ventral presente
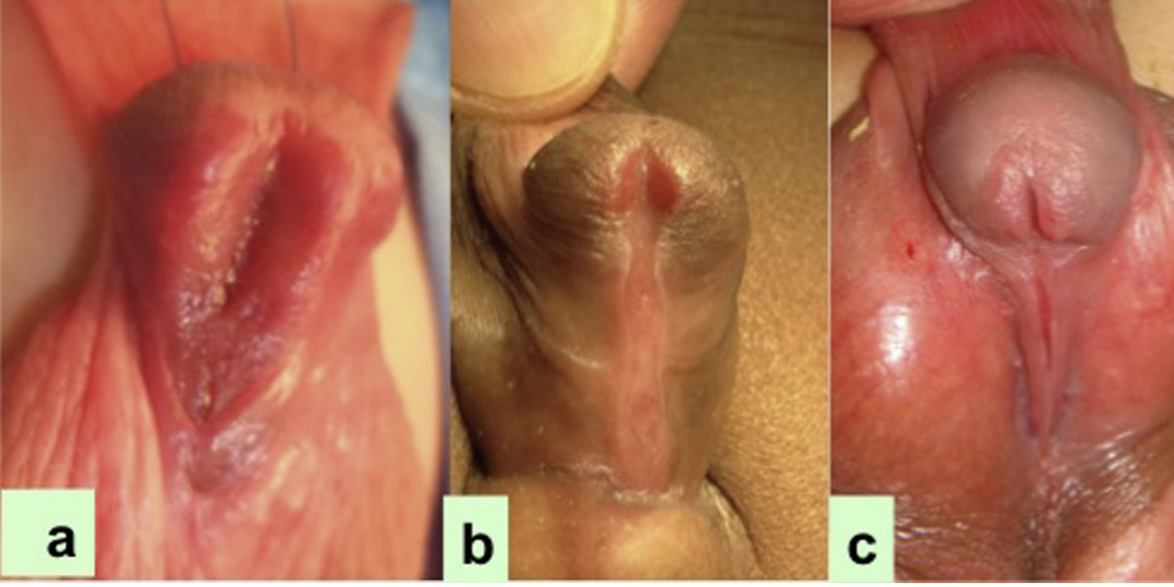
Figura 3 A largura da placa uretral diminui de a para c nos pacientes com hipospádia proximal.14
Exames complementares
Exames de imagem
- A ultrassonografia deve ser realizada em casos de hipospádia proximal para excluir anomalias renais associadas, embora tais anomalias sejam extremamente raras.12 Se houver histórico de infecção do trato urinário recorrente, deve ser realizada uma cistouretrografia miccional. Além disso, em casos de genitália ambígua verdadeira, a MCU pode ajudar a avaliar a presença de remanescentes dos ductos müllerianos. Esses pacientes geralmente são assintomáticos e não requerem ressecção cirúrgica rotineira dos remanescentes. Ocasionalmente, a ressecção do utrículo pode ser necessária por infecção do trato urinário recorrente, gotejamento urinário ou formação de cálculos.12 Durante a operação em pacientes com hipospádia proximal, o utrículo prostático às vezes pode impedir a colocação do cateter na bexiga, com o cateter alojando-se preferencialmente no próprio utrículo. Isso pode ser resolvido utilizando qualquer um dos seguintes métodos i) o método do duplo cateter, no qual o primeiro cateter entra inadvertidamente no utrículo prostático; em seguida, um cateter de menor calibre (French) é inserido pelo meato uretral e este, invariavelmente, entra na uretra; ii) o dilatador de Clutton para guiar o cateter uretral; iii) em casos difíceis, pode-se inicialmente passar para a bexiga um fio-guia maleável sob auxílio de cistoscopia e, então, avançar sobre o fio um cateter de ponta aberta até alcançar a bexiga.15
Cariotipagem
A diretriz da AUA sobre criptorquidia recomenda que todos os meninos com testículos não descidos unilaterais ou bilaterais e hipospádia proximal grave devem ser submetidos a exames adicionais para excluir um distúrbio da diferenciação sexual (DSD), que ocorre com muito mais frequência nesses contextos .9,10 Diretrizes introduzidas em 2006 incluíram a hipospádia grave como uma forma de 46,XY DSD.16 A preocupação com DSD é particularmente alta em um menino com hipospádia e testículo não palpável. Kaefer et al.10 examinaram 79 pacientes com histórico de hipospádia e criptorquidia. Aqueles com testículo(s) não palpável(is), unilateral ou bilateral, apresentaram risco três vezes maior de ter um diagnóstico subjacente de DSD identificado (aproximadamente 50% vs. 15%). Houve um risco significativamente aumentado de DSD com hipospádia proximal em comparação com hipospádia distal (64% vs. 7%) .10 Um cariótipo 46, XY normal pode ser enganoso, particularmente em meninos com as variantes mais graves. Os autores também preferem investigar tais pacientes com hipospádia grave e UDT com Cariotipagem.
Andrógeno Pré-operatório
O uso pré-operatório de DHT ou testosterona pode ser feito por aplicação local ou, mais frequentemente, por injeção intramuscular; pode levar a um aumento do comprimento e da largura do pênis e causar aumento do tamanho da glande. Em pacientes com micropênis, a testosterona demonstrou ser benéfica para estimular o crescimento do pênis. O protocolo de aplicação pode variar entre diferentes instituições. É recomendada a aplicação local de creme de propionato de testosterona a 2% no pênis três vezes ao dia por 3 semanas.12 Essa via de administração da testosterona é de fácil aplicação e apresenta boa resposta. No entanto, a resposta é variável, dependendo da adesão à aplicação diária e da quantidade de creme aplicada. Quantidades excessivas podem levar à absorção sistêmica, ao engrossamento da voz e, em casos extremos, a alterações de comportamento dos meninos. A aplicação deve ser interrompida pelo menos 3 semanas antes da data da cirurgia. A testosterona intramuscular, 2 mg/kg/dose, total de três doses em intervalos de 3 semanas, sendo a última dose administrada pelo menos 2 semanas antes da data da cirurgia, é uma via de administração mais confiável.
Consentimento para Cirurgia
Deve ser obtido um consentimento por escrito plenamente informado após fornecer informações apropriadas, suficientes e oportunas sobre o procedimento planejado e os possíveis procedimentos alternativos que melhor se apliquem ao caso individual. Muitas vezes, o procedimento pode mudar dependendo do exame sob anestesia e, portanto, a possibilidade de várias opções cirúrgicas deve ser informada aos pais previamente. Deve-se fornecer uma visão clara do desfecho, dos resultados estéticos e das possíveis complicações (formação de fístula, estenose ou deiscência). Nos casos de hipospádia proximal, os pais devem compreender que seu filho muito provavelmente necessitará de um reparo em múltiplos estágios. Assim, a preparação da família e do paciente para o procedimento adequado, uma avaliação anatômica precisa e uma discussão honesta sobre os desfechos cirúrgicos e as potenciais complicações são necessárias.7
Momento da cirurgia
O momento da correção eletiva primária é recomendado para ocorrer entre as idades de 6 e 12 meses pela Academia Americana de Pediatria [AAP]7,17, com base em estudos que destacam o equilíbrio entre os potenciais efeitos psicológicos adversos da cirurgia, o risco anestésico para a criança, o grau de desenvolvimento peniano que facilitará uma correção bem-sucedida e as diferenças na cicatrização de feridas à medida que os meninos crescem.18 Belman et al mostraram que meninos submetidos à correção antes dos 12 meses de idade apresentaram menos ansiedade e tiveram desfechos psicosexuais melhores em comparação com meninos submetidos à correção em idades mais avançadas.19
Objetivos da Reconstrução
- Permitir a micção com velocidade normal e fluxo laminar,
- Obter função sexual satisfatória com pênis reto, e
- Obtenção de um meato em fenda com glande bem coaptada, do ponto de vista estético.20
Etapas da Reconstrução
- Correção da curvatura ventral
- Uretroplastia
- Glanuloplastia
- Cobertura cutânea
Técnicas de Correção Cirúrgica
Na hipospádia proximal, estes são mais frequentemente alcançados por meio de uma correção em estágios. Existem duas correntes de pensamento quanto à correção da hipospádia proximal:
- uso de retalhos
- procedimentos de enxerto em etapas
Estes dependem da correção da curvatura ventral. Em raras ocasiões, após o desenluvamento cutâneo não há mais curvatura ventral, e utiliza-se para a uretroplastia a técnica da placa incisa tubularizada (TIP) ou o retalho em ilha onlay, embora a TIP longa seja menos preferida devido a complicações a longo prazo. Se restar curvatura, alguns cirurgiões preferem o reparo em estágios, no qual, após dividir a placa uretral, colocam um enxerto prepucial e, se não disponível, um enxerto de mucosa bucal (BMG) no primeiro estágio e então tubularizam o enxerto no segundo estágio. Se, após o desenluvamento cutâneo, ainda houver curvatura ventral acima de 30 graus, então a correção da curvatura, seja por retalho de túnica vaginal (TVF), por enxerto de túnica vaginal (TVG), por SIS, por enxerto dérmico, ou por múltiplas corporotomias transversas conforme descrito por Snodgrass21, é realizada no primeiro estágio. Em seguida, a uretroplastia é feita no segundo ou terceiro estágio do reparo, com base na técnica utilizada para corrigir a curvatura ventral.
Em resumo, se, após o desenluvamento da pele, há Chordee< 30, então há 2 opções: reparo TIP (não preferido pela maioria dos cirurgiões), e o retalho exclusivamente dorsal.
Se a curvatura peniana for > 30˚, então a Placa uretral (UP) é dividida. Agora, se após a divisão não houver curvatura peniana, podemos usar retalho prepucial dorsal como inlay ou como tubularizado (segundo Duckett) ou podemos usar enxerto prepucial ou BMG.
Correção da Curvatura Ventral Peniana
Visão geral sobre chordee
A correção da curvatura (corda) é o passo inicial mais importante no reparo da hipospádia proximal, seja em estágios ou em estágio único. No primeiro estágio, após o desenluvamento da pele peniana, o grau de curvatura peniana é avaliado pelo teste de ereção artificial. Se a curvatura (corda) for superior a 30 graus, medida com régua ou goniômetro (Figura 4), o passo seguinte será seccionar a placa uretral, o que é feito, na maioria das vezes, na extremidade distal, próximo ao nível da glande. Nesta etapa, corrige-se a curvatura ventral, repara-se a transposição penoescrotal, desenluva-se a pele do corpo peniano e divide-se a placa uretral para corrigir a curvatura.
Moscardi et al.22 apontaram que uma alta porcentagem das curvaturas penianas foi resolvida apenas com o desenluvamento do pênis, a pele ventral encurtada e o dartos ventral fibrótico. Braga et al.23 revisaram a taxa de resolução da curvatura peniana após a dissecção da pele e da fáscia de Dartos em 137 pacientes com hipospádia7 em que 9 apresentavam curvatura leve (<30°), 44 moderada (30–45°) e 85 grave (>45°). A taxa de resolução completa da curvatura, após o desenluvamento do pênis, foi de 70% no grupo de curvatura leve, 30% no de curvatura moderada e 2,4% no de curvatura grave.23
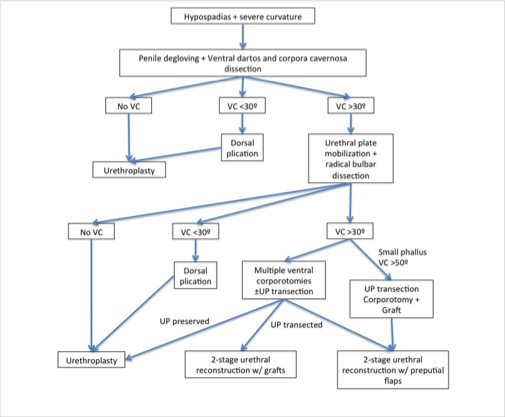
Figura 4 Manejo em pacientes com hipospádia peniana proximal e curvatura peniana.22
Mensuração do Grau de Chordee
O endireitamento da haste peniana é medido utilizando o teste de ereção artificial, isto é, técnica de Gittes e McLaughlin.24 Neste teste, soro fisiológico é injetado através de uma agulha fina (calibre 25–27) na face lateral dos corpos cavernosos ou na glande, com um torniquete na base do pênis (Figura 5).
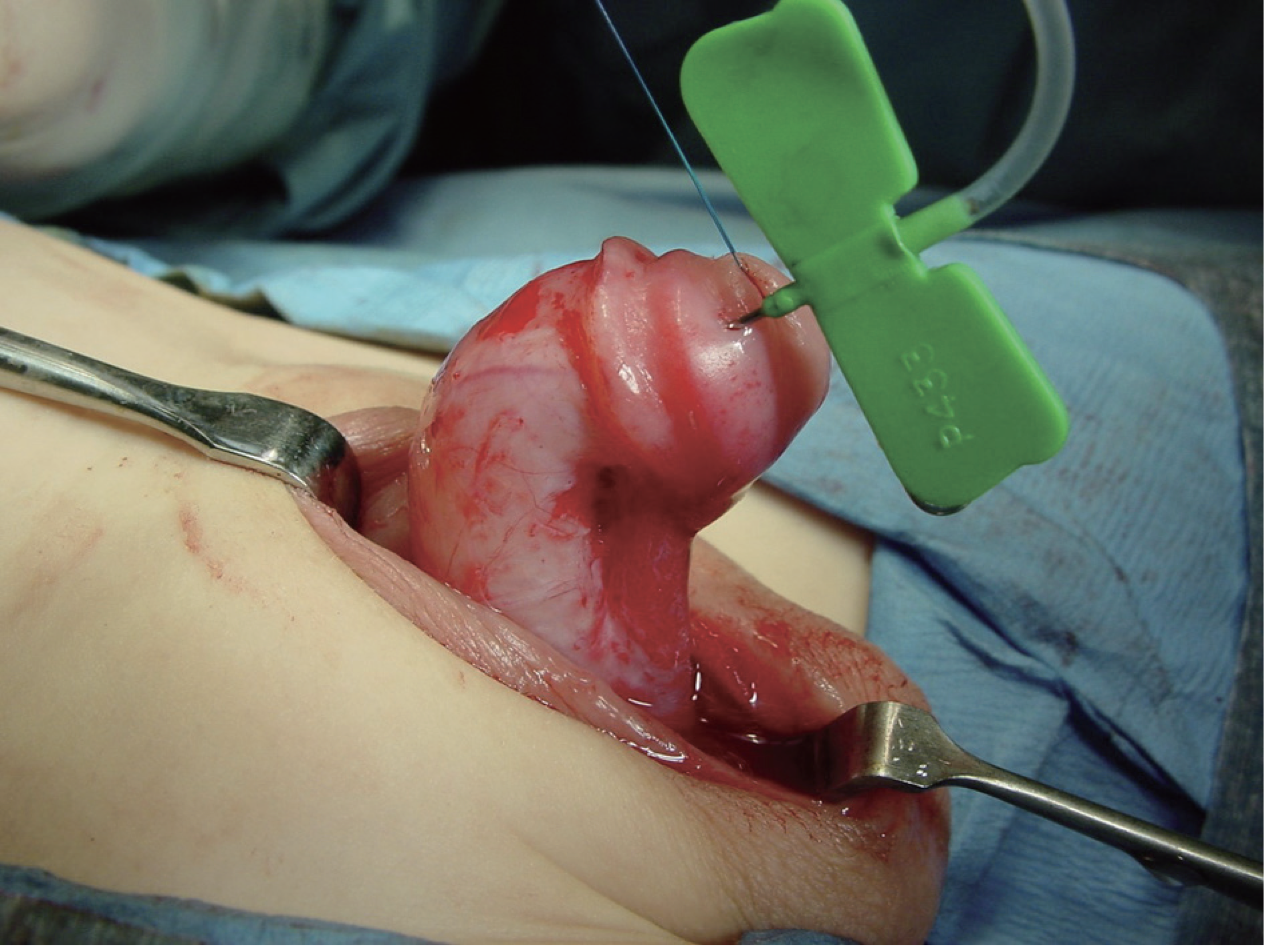
Figura 5 Medição intraoperatória do grau de curvatura peniana.
No entanto, em uma alta porcentagem de hipospádias proximais, após o desenluvamento, se uma ereção artificial apresentar mais de 30 graus de curvatura, então a UP é dividida na extremidade distal próxima à glande, e a uretra proximal é dissecada para endireitar o pênis, melhorar o comprimento peniano e evitar retração pela placa uretral curta e fibrótica.22 As técnicas de alongamento peniano incluem a realização de múltiplas incisões transversais no aspecto ventral da túnica albugínea ou, realizando uma única incisão transversal e aplicando um enxerto ou retalho de túnica vaginal, enxerto de SIS ou de derme (Figura 6).

Figura 6 Correção da curvatura peniana por corporotomia e utilizando enxerto de SIS para cobrir a área cruenta.
Curvatura peniana residual após incisão Up
Em casos em que a chordee ainda persiste no teste de ereção artificial, após dividir a UP, há duas formas de lidar com a chordee residual: corporotomias, isto é, realizar 3 incisões transversais ventralmente, não muito profundas, sem cobertura por qualquer enxerto, ou a outra forma, que os autores também utilizam, é realizar uma grande incisão transversal e então cobri-la com enxerto dérmico, SIS, TVG ou TV FLAP (Figura 7).21
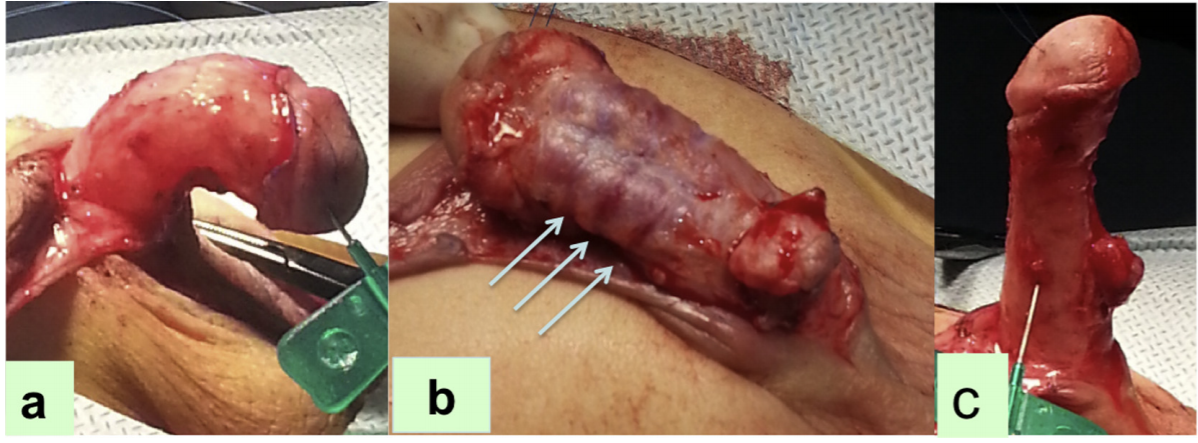
Figura 7 (a) O teste de ereção artificial demonstrando o grau de curvatura (chordee), (b) Múltiplas corporotomias transversais, (c) Retificação da curvatura peniana em testes repetidos. [De: Uma alternativa para alongamento ventral em crianças com curvatura peniana grave que permite cobertura com enxerto durante o reparo da hipospádia em estágios. Bruno Leslie, Bryce Weber, Rodrigo Romao, Walid Farhat, Darius Bagli, Armando Lorenzo, Joao Pippi Salle. J Urol Vol 221, Pg 11, 2011]
Na primeira técnica, três corporotomias transversais são realizadas ventralmente, primeiro no ponto de curvatura máxima, das 4 às 8 horas, e mais duas a 5 mm proximal e a 5 mm distal à primeira, através da túnica albugínea até que o tecido erétil fique visível, e o teste é então repetido. Essas corporotomias podem ser cobertas utilizando a uretra proximal nativa, após a dissecção proximal, ou cobertas por enxerto prepucial ou BMG.21,25
Snodgrass realizou um estudo com 43 meninos com hipospádia proximal e curvatura ventral de 30 graus ou mais; após o desenluvamento, foi realizada a transecção da placa uretral. Os pacientes com curvatura ventral persistente de 30 graus ou mais também foram submetidos a 3 corporotomias ventrais, sem enxertia corporal, para retificação. Realizou-se uretroplastia em estágios com enxerto utilizando prepúcio ou mucosa labial.21,25,26 Constatou-se que a curvatura ventral média era de 70 graus, a corporotomia foi realizada em 65% deles e enxertos prepuciais foram utilizados em 88%; nos demais pacientes, a corporotomia foi coberta por enxertos dérmicos. Nenhum desses pacientes apresentou recorrência da curvatura ventral, embora 10 (23%) tenham tido complicações durante o seguimento e 9 tenham sido submetidos a reoperações.26 Com isso, o conceito atual de correção da hipospádia STraighten And Close (STAC) ou Straighten and Graft (STAG) foi popularizado por Snodgrass e Bush (Figura 8).

Figura 8 O reparo com autoenxerto tubularizado em estágios (STAG). (A) No momento da primeira etapa, são realizadas de uma a três corporotomias ventrais através da túnica albugínea, com a incisão intermediária oposta ao ponto de curvatura máxima. (B) O enxerto prepucial é demarcado e colhido. (C) O enxerto prepucial é colocado na face ventral do corpo peniano e então fixado com suturas em colchoeiro (D). O painel inferior exibe a segunda etapa do reparo. (E) As incisões da uretroplastia são marcadas e estendidas ao longo da linha média do escroto. (F) As asas da glande são confeccionadas. (G) Realiza-se uretroplastia em duas camadas e, subsequentemente, é coberta com uma camada de barreira de túnica vaginal. (H) Aspecto após o fechamento [De: Snodgrass W: Staged tubularized autograft repair for primary proximal hypospadias. J Urol 198:680–686, 2017].
Os retalhos apresentam a referida limitação de suprimento vascular nas bordas, maior chance de estenose e maior taxa de formação de divertículos, pois são menos fixados aos corpos cavernosos subjacentes. Essas limitações são superadas pela técnica com enxerto, na qual há suprimento uniforme ao enxerto, que fica bem fixado aos corpos cavernosos subjacentes e, assim, há menor chance de formação de estenose e de divertículos, respectivamente. O fluxograma de Moscardi et al é útil para individualizar o manejo da curvatura peniana grave em pacientes com hipospádia proximal (Figura 4).22
Plicatura Dorsal
Em alguns pacientes em que a curvatura ainda persiste ou há apenas inclinação da glande, ou se o chordee for menor que 30 graus, pode-se realizar uma plicatura dorsal, conforme previamente popularizado por Baskin. Atualmente, a maioria dos cirurgiões realiza o procedimento de Nesbit ou o procedimento de Nesbit modificado. Nessa técnica, uma cunha em forma de losango da túnica albugínea dorsolateral é ressecada no ponto de máxima curvatura e o defeito é suturado transversalmente em seguida com uma sutura não absorvível, como proline.27 Várias modificações dessa técnica foram relatadas, incluindo plicatura dorsal sem ressecção da fáscia peniana.
Correção de hipospádia em tempo único
Isso geralmente envolve plicatura dorsal para corrigir a curvatura peniana ventral, em conjunto com várias técnicas diferentes de uretroplastia, dependendo do tecido utilizado no reparo; pele prepucial; pele local; ou um enxerto de mucosa bucal.7 Algumas das correções de hipospádia em estágio único são:
Retalho em ilha prepucial transverso (tubo de Duckett);28 Nessa técnica, colhe-se um retalho em ilha prepucial, que é tubularizado em uma uretroplastia de substituição. Esta foi modificada por Asopa,29 em que, em vez de tubularizar o retalho antes de fixá-lo à haste peniana, o lado esquerdo do retalho é ancorado à superfície ventral da haste peniana, logo à esquerda da linha média.7 Em seguida, suturas de Lembert interrompidas são usadas para fechar o retalho na linha média. Isso reduz o risco de exposição do epitélio sob a reconstrução. As suturas são levadas até a porção média da glande. Depois, o retalho é cuidadosamente posicionado sobre a linha de sutura, e as asas da glande são trazidas sobre a uretroplastia e o retalho vascularizado. A base do retalho tubularizado é ancorada à extremidade distal da uretra nativa (Figura 9).2,7 Realiza-se uma tubularização em duas camadas, mantendo um calibre uniforme em todo o trajeto. Em pacientes com curvatura grave corrigida após a dissecção cutânea e a divisão da placa uretral, essa abordagem pode ser útil.7
O procedimento de Retalho em Ilha Onlay: OIF é indicado em meninos nos quais a curvatura é corrigida após desenluvamento peniano e não requer a divisão de uma placa uretral relativamente delgada que, de outra forma, não poderia ser tubularizada.7 As características mais importantes deste procedimento e de outras técnicas de reparo da hipospádia em tempo único são apresentadas abaixo.
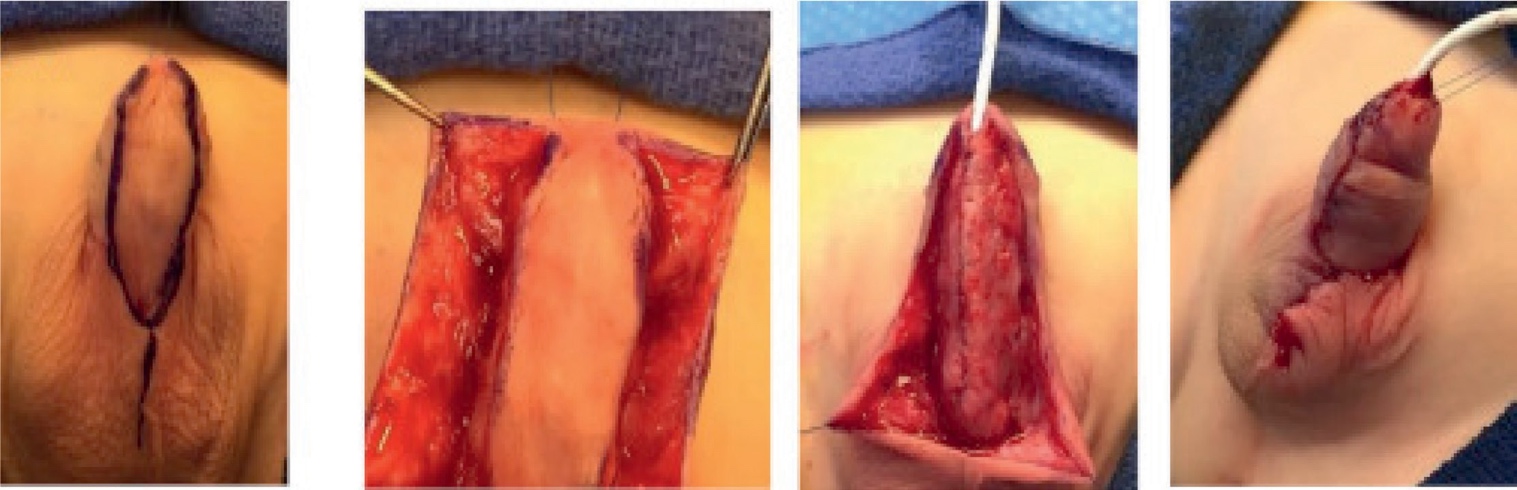
Figura 9 Correção da hipospádia com tubo em ilha. (A) Aspecto pré-operatório. A pele ventral rosada e brilhante sugere afinamento do corpo esponjoso ventral. Apesar do meato subcoronal, trata-se de uma variante proximal. (B) Após o desenluvamento, o meato é localizado na junção penoescrotal e é cateterizado com uma sonda de alimentação 8-Fr. (C) A ereção artificial após plicatura dorsal não revela curvatura peniana residual. (D) O retalho prepucial em ilha é mobilizado, com colheita do pedículo de dartos flexível a partir da pele do corpo peniano em direção à base do pênis. (E) Uma borda do retalho é ancorada à túnica albugínea. (F) O retalho é ajustado a uma largura de 12 mm, com excisão do epitélio redundante. Em seguida, o retalho é fechado sobre um tubo de derivação, aproximando a borda epitelial da porção previamente ancorada do retalho. (G) Reparo concluído. [De Kraft KH, Shukla AR, Canning DA: Hypospadias. Urol Clin North Am 2010; 37: 167–181.]
Retalho em ilha onlay
- Retalho em ilha colhido da mucosa prepucial interna
- A largura combinada da placa uretral e do retalho deve ser de 12 mm ou menos e é aparada conforme necessário, em particular para estreitar o retalho proximal a fim de prevenir um divertículo na junção da anastomose entre a neo-uretra e a uretra nativa
- A vascularização da pele dorsal não depende do tecido subcutâneo
- Pode ser realizado em hipospádia escrotal/perineal
- Sem estenoses
- Taxa de fístulas reduzida para 15%
Base lateral
- Em hipospádia proximal com pouca curvatura peniana30
- Glande pequena ou plana
- A largura do retalho é determinada pela placa uretral
- Suturar a extremidade distal do retalho a 2mm da ponta da glande
- A borda esquerda é suturada primeiro antes de separar da borda direita
Reparo com retalho em ilha tubularizado
- Casos de hipospádia grave em que a placa uretral precisa ser ressecada
- Transferência dorsoventral da uretroplastia com placa tubularizada (DVTPTU)
- Alta incidência de divertículos
- Baixa incidência de formação de fístulas
Uretroplastia TIP estendida
- Descrita no contexto de um menino cuja curvatura é corrigida com dissecção cutânea ou plicatura em combinação com uma placa uretral adequada31
- Modificações técnicas incluindo mobilização da placa uretral e corporotomias transversas, no contexto de curvatura ventral persistente superior a 30 graus após desenluvamento, para aumentar sua aplicabilidade.
- No entanto, análise de Snodgrass et al.32 sugeriu que a mobilização agressiva da placa uretral pode levar à desvascularização, aumentando o risco de formação de estenose, o que, em última instância, limita a aplicabilidade do TIP proximal no contexto de hipospádia grave com corda. Devido ao maior risco de complicações, essa técnica desde então caiu em desuso em favor de outras reconstruções em dois tempos, como o retalho de Byars ou o reparo STAG.
Correção de hipospádia em dois tempos
Procedimentos mais comumente realizados para hipospádia grave
- Reparo em dois tempos de Byars:
- Na fase 1
- Correção da curvatura peniana (chordee)
- Realiza-se o endireitamento peniano com remoção da placa uretral ventral aderida
- Retalho prepucial formado pela divisão da pele dorsal é rotacionado para cobrir o defeito ventral
- Abrir amplamente a glande & posicionar retalho cutâneo adequado
- Na Fase 2
- A área é tubularizada em um tubo uretral
- Realizado pelo menos 6 meses após a fase 1
- Na fase 1
Shukla et al realizaram correção de hipospádia proximal pela técnica do retalho de Byar em 700 meninos ao longo de um período de 11 anos.33 Relataram fístula em 21 (3%) desses pacientes. Nenhum apresentou deiscência completa, divertículos uretrais ou estenose meatal. Na sua série, a faixa etária dos pacientes em nosso estudo foi de 3–12 anos e a segunda etapa foi realizada pelo menos 1 ano após a primeira cirurgia. Os autores enfatizaram as vantagens de um retalho de Byar: 1) por ser um retalho cutâneo vascularizado, consideraram-no confiável quando utilizado na primeira etapa e, ao mesmo tempo, restava pele vascularizada abundante para recobrir a área cruenta criada como resultado da correção da chordee, 2) ao término do procedimento, obtinha-se um aspecto circuncidado, 3) não se relataram contração ou perda, ao contrário do que ocorre no caso de um enxerto, em seu estudo.33
- Correção de hipospádia em dois tempos com enxerto bucal/prepucial de Bracka34
- No estágio 1 (Figura 10):
- Tecido cicatricial prévio, se houver, é ressecado
- As asas da glande são mobilizadas
- O enxerto bucal ou o enxerto prepucial livre é fixado com suturas em quilting para cobrir a área ventral da cicatriz ressecada
- O sítio doador da mucosa bucal é geralmente o lábio ou a bochecha
- A sutura do defeito mucoso após a remoção do enxerto não é recomendada.
- No estágio 2:
- A placa é tubularizada, geralmente após 6 meses
- Bom procedimento para refazer uretroplastias
- No estágio 1 (Figura 10):
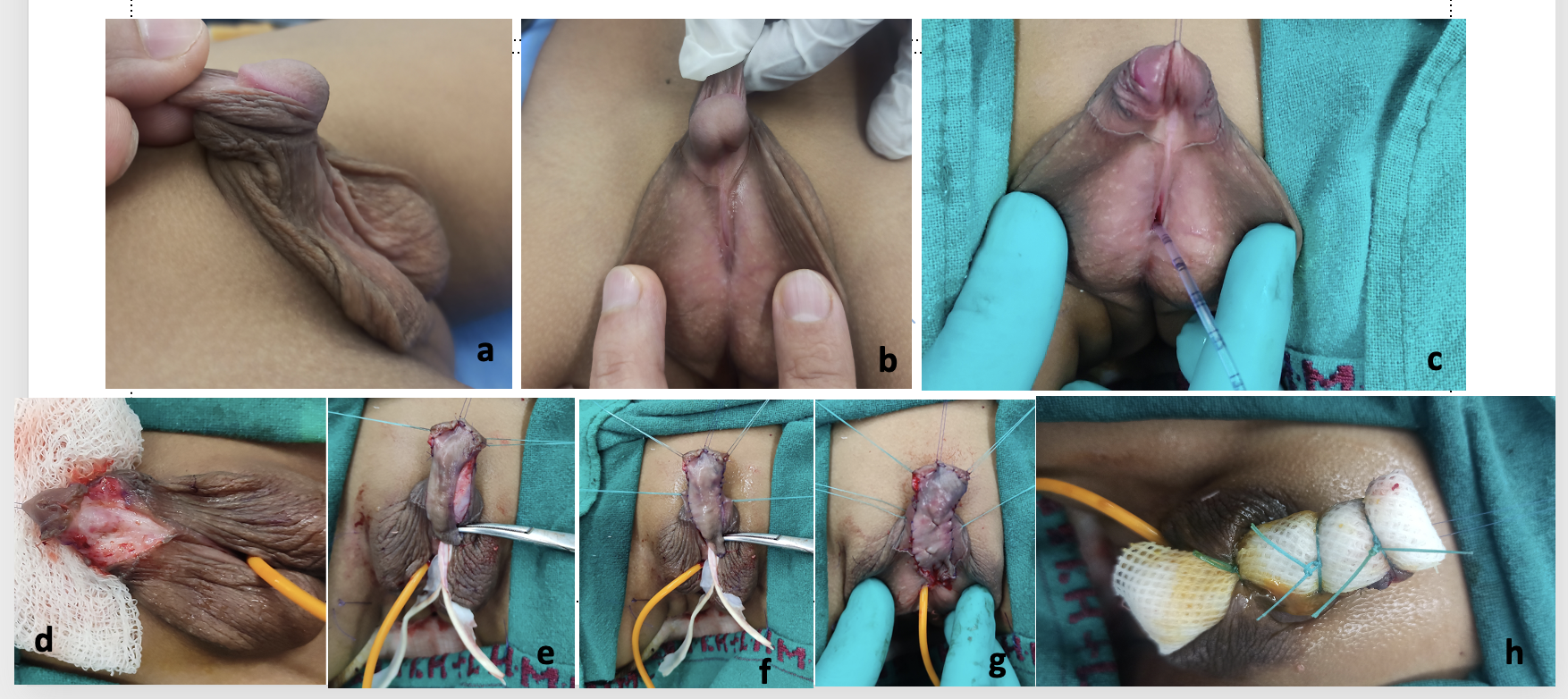
Figura 10 Cortesia do Dr. Vikram Khanna, Professor Associado , Cirurgia Pediátrica, Lady Harding Medical College e Kalawati Saran Children’s Hospital, Nova Deli, a) Foto pré-operatória mostrando hipospádia penoescrotal com transposição penoescrotal, curvatura peniana (chordee) e falo curto com prepúcio em capuz dorsal, b) Perfil lateral mostrando o grau de curvatura peniana e a placa uretral, c) sonda de alimentação inserida como stent usando o método de duplo cateter
d) Desenluvamento do corpo peniano e correção da curvatura peniana, e) Enxerto de pele prepucial colhido, f) Enxerto suturado à área das asas da glande separadas e à área da placa uretral e do corpo cavernoso, g) Fixação completa do enxerto com quilting realizada, h) Curativo tie-over feito sobre o enxerto e cateter mantido in situ por 1 semana.
Bracka descreveu o conceito de correção do hipospádia em 2 estágios.34 Após pelo menos 6 meses do primeiro estágio da correção, o segundo estágio pode ser realizado. Durante essa correção, corrige-se qualquer curvatura peniana residual, realiza-se a tubularização do enxerto, cria-se a neouretra, e fazem-se a meatoplastia e a glanuloplastia. A uretroplastia é coberta por um retalho de dartos ou por um retalho de túnica vaginal. Na era atual, tornou-se amplamente aceita como tratamento primário para pacientes com hipospádia proximal e curvatura peniana. Na série de Bracka de correção do hipospádia em dois estágios em pediatria, que incluiu 457 crianças (369 correções primárias e 88 secundárias ou de resgate) e 143 adultos (22 primárias e 121 secundárias), 5.7%35 desenvolveram fístulas uretrocutâneas, 7%14 desenvolveram estenoses, e 4.6%29 desenvolveram estenoses de aparecimento tardio.34,35
O uso da pele do folheto interno do prepúcio é uma excelente opção, pois o enxerto é fino, flexível, glabro e resiste a um ambiente úmido. O enxerto é colhido, a fáscia de Dartos é removida, e ele é anastomosado ventralmente aos corpos cavernosos para formar a placa neouretral. A tubularização do enxerto é geralmente realizada mais tarde, após 6 meses. Um dos problemas
com enxerto de prepúcio é a disponibilidade desse enxerto. Isso ocorre porque muitos pacientes com hipospádia proximal e curvatura ventral têm pele peniana escassa e, toda a pele é necessária e usada para o revestimento cutâneo do pênis no estágio inicial. Embora o uso de enxertos para o reparo da hipospádia tenha sido empregado principalmente em reoperações, algumas séries relataram bons resultados com reparo em estágios utilizando enxertos prepuciais também para a correção primária da hipospádia proximal.36,37
Nos casos em que a pele prepucial não pode ser utilizada ou está indisponível, a mucosa bucal (Figura 11) é colhida da face interna da bochecha e/ou da região alveolar labial inferior e enxertada nos corpos cavernosos. Suas propriedades incluem maior conteúdo de elastina, rigidez relativa que proporciona bom suporte e, por fim, diminui a ocorrência de divertículo uretral e prolapso meatal,38,39 o que a torna adequada para seu uso na cirurgia de hipospádia. Durante a colheita do enxerto de mucosa bucal, deve-se evitar cruzar o ângulo da boca em direção ao lábio inferior, evitando assim deformidades estéticas faciais. Em segundo lugar, deve-se tomar cuidado para evitar o ducto de Stensen ao colher a mucosa da face interna da bochecha.
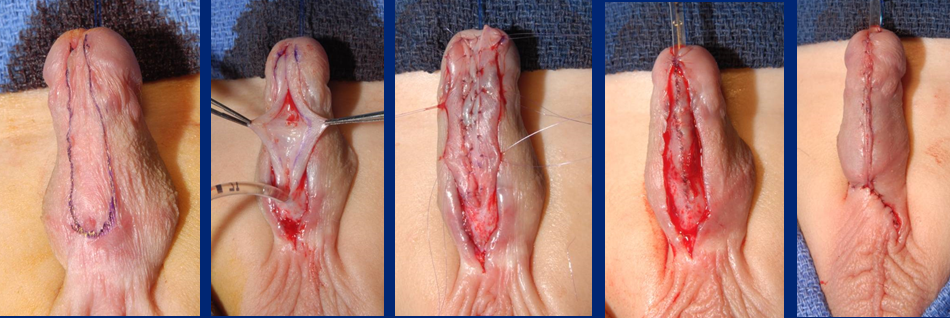
Figura 11 Tubularização do enxerto tipo inlay de mucosa bucal
Com base na literatura disponível, o enxerto prepucial em casos primários é o método preferido; os outros enxertos disponíveis são o enxerto lingual e os enxertos de mucosa bucal.40,41 Nos casos de hipospádia proximal, na maioria das vezes, podemos usar a mucosa prepucial, que não é propriamente pele prepucial e apresenta aspecto brilhante, como enxerto, e não encontramos deficiência de pele na primeira etapa, uma vez que não estamos cobrindo o pênis com pele na primeira etapa da colocação do enxerto.
Em uma série de 43 meninos que completaram ambas as etapas com seguimento pós-operatório, Snodgrass e Bush concluíram que o autoenxerto tubularizado em estágios resultou em pênis reto com neomeato em posição normal em 77% dos meninos com a forma mais grave de hipospádia proximal.26 Esse número aumentou para 98% após 1 ou 2 reoperações por complicações. Na série deles, também não foi observada recorrência da curvatura ventral após terem sido realizadas 3 corporotomias sem enxerto corporal [Snodgrass]. A curvatura ventral média nesses pênis foi de 70 graus, e a corporotomia foi realizada em 65%; enxertos prepuciais foram utilizados em 88%.26
Manejo e cuidados pós-operatórios
Drenagem urinária
A drenagem deve ser garantida por uma sonda de alimentação infantil deixada in situ após o reparo. Geralmente usamos uma IFT 6F ou 8F para crianças pequenas e uma 10F a 12F para crianças maiores, adolescentes e adultos. Deve-se ter cuidado ao posicionar a ponta do stent dentro da bexiga, de modo que não ocorram espasmos vesicais por irritação do trígono e não haja formação de nós internos devido ao comprimento excessivo do cateter deixado no interior. O ideal é utilizar um cateter de silicone.
Curativo
O curativo é aplicado de forma circular ao redor do corpo do pênis após acolchoamento adequado sobre a região escrotal reparada. Não deve ficar nem muito apertado nem muito frouxo, e a ponta da glande deve estar visível ou exposta para inspeção visual durante o período pós-operatório.
Outra alternativa poderia ser aplicar um curativo e fixá-lo à parede abdominal com um curativo plástico estéril ou um curativo em sanduíche com Elastoplast.
Durante o reparo em estágios, ao utilizar o enxerto na primeira etapa, usamos um curativo tie-over (Figura 10) para fixar o enxerto, e ele é removido uma semana depois. O enxerto por baixo é fixado aos corpos cavernosos subjacentes por meio de suturas de quilting. O curativo tie-over ajuda a obliterar qualquer espaço morto entre o enxerto e os corpos cavernosos subjacentes, drenar o excesso de líquido e favorece melhor aposição do tecido do enxerto.
Complicações
A breve visão geral das principais complicações após o reparo pode estar relacionada tanto à uretroplastia quanto a complicações cutâneas.7
Complicações da Uretroplastia
- Fístula
- Deiscência da glande
- Sintomas obstrutivos de estenose meatal (esforço miccional, micção prolongada, infecção do trato urinário e/ou retenção urinária)
- Estenose uretral
- Divertículo uretral
Complicações cutâneas
- Necrose cutânea
- Torsão peniana > 30 graus- ângulo entre o plano vertical normal da glande e o plano vertical verdadeiro da glande >30 graus em relação à linha média (especificar no sentido horário ou anti-horário)
- Fístula prepucial - defeito tipo fístula na pele do prepúcio que não tem contato com o lúmen uretral
- Deiscência prepucial após reconstrução prepucial: defeito na pele do prepúcio recriando um prepúcio incompleto
- Líquen escleroso
Estas também podem ser definidas como precoces, na forma de isquemia da glande, necrose do retalho prepucial, obstrução do cateter, expulsão prematura do cateter e infecção da ferida. As complicações tardias incluem formação de fístula uretrocutânea, deiscência da glande, estenose do meato, curvatura peniana recorrente ou residual, estenose uretral, deiscência uretral e divertículo uretral.
Tabela 3 As complicações de vários estudos de enxerto em dois estágios foram destacadas, a apenas 48 (de 140) pacientes foram tratados em dois estágios usando enxerto prepucial, b 15 (30%) pacientes tiveram múltiplas complicações, c 44 eram casos primários, com 8 sendo reoperações.
| Estudo | Número de pacientes | Seguimento médio (meses) | Localização do meato | Tipo de reparo | Complicações gerais (%) | Estenose meatal (%) | Deiscência (%) | Estenose uretral (%) | Divertículos uretrais (%) | Fístula (%) | Curvatura residual (%) | Outros |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferro, 200236 | 34 | 1–48 (intervalo) | proximal | Enxerto prepucial em 2 estágios | 8 (24%) | 0 | 4 (11.7%) | 1 (3%) | 1 (3%) | 2 (6%) | — | — |
| Johal, 200637 | 62 | 26 (mediana) | terço médio / proximal | Enxerto em 2 estágios | 11 (18%) | 3 (5%) | 3 (5%) | 0 | 0 | 0 | 3 (5%) | Jato desviado 2 (3%) |
| Pippe Salle, 201614 | 48a | 29.6 (mediana) | proximal | Enxerto em 2 estágios | 16 (33.3%) | 0 | 7 (14.5%) | 1 (2%) | 1 (2%) | 5 (10.4%) | 2 (4.1%) | — |
| Faure, 201642 | 52 | 34 (mediana) | proximal / redoc | Enxerto em 2 estágios (prepucial/BMG) | 20 (38.4%) | 8 (15.3%) | 1 (1.9%) | 4 (7.6%) | 1 (1.9%) | 8 (15.3%) | 0 | — |
| Sakr, 201743 | 23 | 12 | reoperação | 2 estágios (enxerto lingual) | 3 (13%) | 0 | 1 | 0 | 0 | 2 | 0 | — |
| Snodgrass, 201726 | 43 | 22 | proximal | 2 estágios | 10 (24%) | 0 | 7 (16.2%) | 0 | 1 (2.3%) | 2 (4.6%) | 0 | — |
| Lanciotti, 201740 | 50 | 63.6 | proximal | 2 estágios (enxerto vesical) | 23 (46%)b | 4 (8%) | 0 | 15 (30%) | 6 (12%) | 9 (18%) | 5 (10%) | Prolapso do meato 7 (14%) |
Tabela 4 As complicações de vários estudos de reparo com retalho em 2 estágios foram destacadas. a técnica combinada em 2 estágios com TIP distal e retalho de Byars tubularizado, b - VC reavaliada durante o procedimento em 2 estágios com ereção artificial, c 37 foram realizados em 2 procedimentos, d 6 tiveram tubo vesical, enxertos bucais etc, e Apenas 12 (de 140) pacientes foram tratados com retalhos prepuciais em dois estágios, f 81 (de 167) pacientes foram tratados com retalhos prepuciais em dois estágios, TPIF=retalho ilhado prepucial transverso; BILAB=retalho cutâneo de base bilateral.
| Estudo | Número de pacientes | Seguimento médio (meses) | Localização do meato | Tipo de reparo | Complicações gerais (%) | Estenose meatal (%) | Deiscência (%) | Estenose uretral (%) | Divertículos uretrais (%) | Fístula (%) | Curvatura residual (%) | Outros |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Greenfield, 199444 | 39 | 16 | Subglandular a perineal | retalho em 2 estágios (belt-fuqua) | 16 (41%) | 0 | 0 | 7 (17.9%) | 8 (20.5%) | 1 (2.5%) | — | - |
| Retik, 199445 | 58 | — | Escrotal/perineal | retalho em 2 estágios | 3 (5%) | 0 | 0 | — | — | 3 (5%) | — | - |
| Cheng, 200346 | 14 | 6–36 (intervalo) | proximal | em 2 estágiosa | 4 (28.5%) | 0 | 0 | 0 | 2 (14%) | 1 (7%) | 0b | Retração meatal 1 (7%) |
| Hadidi, 201439 | 63c | 43 | perineal | 1 estágio/2 estágios BILAB | 9 (14.2%) | — | 3 (4.7%) | — | 2 (3%) | 1 (1.5%) | — | Contratura cicatricial 3 (4.7%) |
| McNamara, 201547 | 134d | 45.6 (mediana) | proximal | retalho em 2 estágios | 71 (53%) | 17 (12.7%) | 19 (14.2%) | 16 (11.9%) | 12 (9%) | 39 (29.1%) | 3 (2.2%) | - |
| Stanasel, 201548 | 56 | 38.6 | proximal | retalho em 2 estágios | 38 (68%) | 5 (9%) | 3 (5%) | 8 (14%) | 8 (14%) | 32 (57%) | — | - |
| Tiryaki, 201649 | 34 | 44.8 | proximal | retalho de Byars em 2 estágios | 32 (95%) | 0 | 0 | 0 | 24 (70%) | 23 (67%) | 1 (3%) | 27 prolapso uretral |
| Pippe Salle, 201614 | 12e | 29.6 | proximal | retalho em 2 estágios | 4 (41.6%) | 0 | 3 (25%) | — | 0 | 2 (16.6%) | 1 (8.3%) | - |
| Chen, 201650 | 87 | TPIF - 38 (mediana)Byars – 36 (mediana) | proximal | TPIF em estágios,42 retalho de Byars em 2 estágios45 | TPIF 9.5%, Byars 33% | — | 0, 3 (6.6%) | 1 (2.3%), 2 (4.4%) | 1 (2.3%), 0 | 2 (4.6%), 10 (22.2%) | 0b,0b | - |
| Long, 201736 | 81f | 27.7 (mediana) | proximal | retalho de Byars em 2 estágios | 40 (49%) | 5 (6%) | 6 (7%) | — | 5 (6%) | 30 (37%) | 3 (4%) | - |
| Jayanthi, 201737 | 34 | 15.2 | proximal | Ulaanbaatar modificada | 5 (14.7%) | 0 | 0 | 0 | 4 (12%) | 0 | — | Epididimite recorrente 1 (2.7%) |
Em um estudo realizado no The Children’s Hospital of Philadelphia (CHOP) entre 1996–2006, que comparou os resultados de 665 meninos consecutivos submetidos à correção de hipospádia, constatou-se que a taxa de complicações para todas as hipospádias foi de 17%.51 Dos 665, 86 (13%) apresentavam hipospádia proximal, definida pela localização do meato uretral proximal à porção média do eixo peniano após desenluvamento peniano no centro cirúrgico. Observou-se que um número desproporcional de complicações (35%) ocorreu nos meninos com hipospádia proximal, com uma taxa de complicações de hipospádia proximal de 39/86 (45%).51 Isso contrastou fortemente com a taxa global de complicações de 17%.51
A maioria dos pacientes submetidos à correção de hipospádia proximal requer um seguimento mais prolongado e mais próximo para um relato detalhado e honesto das complicações. Um hypospadias criple pode ser definido como um menino que frequentemente requer múltiplos procedimentos complexos para corrigir as sequelas de uma reparação inicial malsucedida.52 Devido ao tubo de uretroplastia mais longo, há um risco maior de estenose ou um efeito profundo da falha da uretra reconstruída em se expandir durante a micção, aumentando a resistência ao fluxo urinário e, em última instância, resultando na formação de fístula e/ou divertículo uretral, como destacado por Braga et al.53 Assim, anteriormente houve subnotificação das complicações nas hipospádias proximais.
Para melhorar os desfechos do reparo da hipospádia proximal, Long e Canning51 apontaram que pode ser utilizado um sistema padronizado para quantificar de forma sistemática a gravidade do fenótipo da hipospádia, de modo a criar uma linguagem universal da hipospádia que facilitaria a colaboração entre instituições. Atualmente, os sistemas de pontuação utilizados são o HOSE, o HOPE e o GMS13,54, que incluem diversos fatores como a largura da glande, o grau de curvatura peniana e a qualidade da placa uretral para, em um determinado paciente, calcular uma pontuação específica. Isso, em certa medida, tem simplificado a comparação para análise de desfechos, ressalvadas algumas limitações relacionadas ao paciente e à variabilidade interobservador entre cirurgiões.
Eles também destacaram a importância de que a avaliação do paciente e da família seja cotejada com a análise do cirurgião após a intervenção cirúrgica51, pois nem sempre coincidem. O escore de percepção peniana leva em conta essa limitação.55 Weber et al55, em seu estudo, avaliaram 77 meninos (6–17 anos) submetidos à correção de hipospádia quanto à autopercepção peniana com relação ao meato, glande, pele e aparência geral. Eles constataram que a intercorrelação desses itens “meato”, “glande” e “pele” com “aparência geral” foi boa entre os meninos, os pais e os urologistas. Pacientes com hipospádia expressaram alta satisfação com a aparência peniana, que não diferiu significativamente dos controles pareados por idade. Curiosamente, contudo, os pais e os urologistas mostraram-se menos satisfeitos com a aparência peniana do que os próprios pacientes.55 Isso ressalta a importância da autoavaliação pelo paciente e pelos pais, além da avaliação do cirurgião operador.
Outro método sugerido por Long et al é por meio de mentoria e trabalho em equipe51 utilizando várias oportunidades, como reuniões, conferências, workshops, análise crítica de vídeos gravados em grupo fechado, feedback e discussão. Isso certamente aumentaria a exposição e aprofundaria a compreensão dessa condição complexa e rara de hipospádia proximal.
Referências
- Baskin LS. Chapter 121 - Hypospadias. In: Coran AG, In, editors. Pediatric Surgery (Seventh Edition). Mosby; 2012. DOI: 10.1016/b978-0-323-07255-7.00121-5.
- Samuel M, Capps S, Worth A. Proximal Hypospadias. Eur Urol 2011; 40 (4): 463–468. DOI: 10.1159/000049817.
- Baskin L, Erol A, Jegatheesan P, Li Y, Liu W, Cunha G. Urethral seam formation and hypospadias. Cell Tissue Res 2001; 305 (3): 379–387. DOI: 10.1007/s004410000345.
- Baskin L, Shen J, Sinclair A, Cao M, Liu X, Liu G, et al.. Development of the human penis and clitoris. Differentiation 2018; 103: 74–85. DOI: 10.1016/j.diff.2018.08.001.
- Smith DR, Tanagho EA, McAninch JW. Smith’s General Urology. Norwalk, Conn: Appleton & Lange; Chap; 1992.
- Wein AJ, Kavoussi LR, Campbell MF. 1. 2012.
- Gerasaro TS, Brock WA, Kaplan GW. Upper Urinary Tract Anomalies Associated With Congenital Hypospadias: Is Screening Necessary? J Urol 1986; 135 (3): 537–538. DOI: 10.1016/s0022-5347(17)45729-6.
- Rajfer J, Walsh PC. The Incidence of Intersexuality in Patients with Hypospadias and Cryptorchidism. J Urol 1976; 116 (6): 769–770. DOI: 10.1016/s0022-5347(17)59004-7.
- Kaefer M, Diamond D, Hendren WH, Vemulapalli S, Bauer SB, Peters CA, et al.. The Incidence Of Intersexuality In Children With Cryptorchidism And Hypospadias: Stratification Based On Gonadal Palpability And Meatal Position. J Urol 1999; 162 (3 Part 2): 1006–1007. DOI: 10.1016/s0022-5347(01)68049-2.
- Ahmed SF, Achermann JC, Arlt W, Balen A, Conway G, Edwards Z. Society for Endocrinology UK guidance on the initial evaluation of an infant or an adolescent with a suspected disorder of sex development. 2015; 4 (5): 71–88. DOI: 10.1111/j.1365-2265.2011.04076.x.
- Hadidi AT, Azmy AF. Hypospadias surgery: an illustrated guide. 2004. DOI: 10.1111/j.1440-1754.2005.571_3.x.
- Shoor G, Acharya SK. Bedside clinics and Round questions in Pediatric Surgery. 2022.
- Arlen AM, Kirsch AJ, Leong T, Broecker BH, Smith EA, J.M.. Faculty Opinions recommendation of Further analysis of the Glans-Urethral Meatus-Shaft (GMS) hypospadias score: correlation with postoperative complications. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 11. DOI: 10.3410/f.725403208.793522967.
- Abbott JE, Heinemann A, Badalament R, Davalos JG. A clever technique for placement of a urinary catheter over a wire. Urol Ann 2015; 7 (3): 367. DOI: 10.4103/0974-7796.157959.
- Hughes IA, Houk C, Ahmed SF, Lee PA, Group LWPESC, Group ESPEC. Consensus Statement on Management of Intersex Disorders. Pediatric Clinical Practice Guidelines &Amp; Policies 2006; 91 (7): 1317–1317. DOI: 10.1542/9781610021494-part06-consensus_statement2.
- Urology S on. Timing of Elective Surgery on the Genitalia of Male Children With Particular Reference to the Risks, Benefits, and Psychological Effects of Surgery and Anesthesia. Pediatrics 1996; 97 (4): 590–594. DOI: 10.1542/peds.97.4.590.
- Bermudez DM, Canning DA, Liechty KW. Age and pro-inflammatory cytokine production: Wound-healing implications for scar-formation and the timing of genital surgery in boys. J Pediatr Urol 2011; 7 (3): 324–331. DOI: 10.1016/j.jpurol.2011.02.013.
- Belman AB, Kass EJ. Hypospadias Repair in Children Less than 1 Year Old. J Urol 1982; 128 (6): 1273–1274. DOI: 10.1016/s0022-5347(17)53458-8.
- Hadidi AT. History of hypospadias: Lost in translation. J Pediatr Surg 2017; 52 (2): 211–217. DOI: 10.1016/j.jpedsurg.2016.11.004.
- Snodgrass W, Prieto J. Straightening Ventral Curvature While Preserving the Urethral Plate in Proximal Hypospadias Repair. J Urol 2009; 182 (4s): 1720–1725. DOI: 10.1016/j.juro.2009.02.084.
- Moscardi PRM, Gosalbez R, Castellan MA. Management of High-Grade Penile Curvature Associated With Hypospadias in Children. Front Pediatr 2017; 5 (189). DOI: 10.3389/fped.2017.00189.
- Braga LHP, Pippi Salle JL, Dave S, Bagli DJ, Lorenzo AJ, Khoury AE. Outcome Analysis of Severe Chordee Correction Using Tunica Vaginalis as a Flap in Boys With Proximal Hypospadias. J Urol 2007; 178 (4s): 1693–1697. DOI: 10.1016/j.juro.2007.03.166.
- Gittes RF, McLaughlin AP. Injection technique to induce penile erection. Urology 1974; 4 (4): 473–474. DOI: 10.1016/0090-4295(74)90025-9.
- Castellan M, Gosalbez R, Devendra J, Bar-Yosef Y, Labbie A. Ventral corporal body grafting for correcting severe penile curvature associated with single or two-stage hypospadias repair. J Pediatr Urol. 2011;7:289-93. . DOI: 10.1016/j.jpurol.2012.02.009.
- Snodgrass W, Bush N. Staged Tubularized Autograft Repair for Primary Proximal Hypospadias with 30-Degree or Greater Ventral Curvature. J Urol 2017; 198 (3): 680–686. DOI: 10.1016/j.juro.2017.04.019.
- Nesbit RM. Operation for Correction of Distal Penile Ventral Curvature with or Without Hypospadias. J Urol 1966; 97 (4): 720–722. DOI: 10.1016/s0022-5347(17)63105-7.
- Duckett JW. Transverse Preputial Island Flap Technique for Repair of Severe Hypospadias. Urol Clin North Am 1980; 7 (2): 423–430. DOI: 10.1016/s0094-0143(21)01243-x.
- Ascopa HS, Elhence IP, Atri SP, Bansal NK. One stage correction of penile hypospadias using a foreskin tube. Plast Reconstr Surg 1971; 49 (1): 104–105. DOI: 10.1097/00006534-197201000-00044.
- Hypospadias Surgery: Science and Art - V.V.S. . DOI: 10.4103/jiaps.jiaps_202_20.
- Snodgrass WT, Lorenzo A. Tubularized incised-plate urethroplasty for proximal hypospadias. BJU Int 2002; 89 (1): 90–93. DOI: 10.1046/j.1464-410x.2002.02524.x.
- Snodgrass WT, Granberg C, Bush NC. Faculty Opinions recommendation of Urethral strictures following urethral plate and proximal urethral elevation during proximal TIP hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2013; 9 (6 Pt B): 990–994. DOI: 10.3410/f.718013467.793494058.
- Singh AP, Shukla AK, Sharma P, Shukla J. Two stages repair of proximal hypospadias: Review of 700 cases. J Indian Assoc Pediatr Surg 2017; 22 (3): 158. DOI: 10.4103/0971-9261.207627.
- Bracka A. Hypospadias repair: the two-stage alternative. Br J Urol 1995; 76 (6): 31–41. DOI: 10.1111/j.1464-410x.1995.tb07815.x.
- Bracka A. Buccal Mucosa: Good But Not Perfect. J Urol 2011; 185 (3): 777–778. DOI: 10.1016/j.juro.2010.12.015.
- FERRO F, ZACCARA A, SPAGNOLI A, LUCCHETTI MC, CAPITANUCCI ML, VILLA M. Skin Graft for 2-stage Treatment of Severe Hypospadias: Back to the Future? J Urol 2002; 168 (4 Pt 2): 1730–1733. DOI: 10.1097/00005392-200210020-00018.
- Johal NS, Nitkunan T, O’Malley K, Cuckow PM. The Two-Stage Repair for Severe Primary Hypospadias. Eur Urol 2006; 50 (2): 366–371. DOI: 10.1016/j.eururo.2006.01.002.
- Dessanti A, Rigamonti W, Merulla V, Falchetti D, Caccia G. Autologous Buccal Mucosa Graft for Hypospadias Repair: An Initial Report. J Urol 1992; 147 (4): 1081–1083. DOI: 10.1016/s0022-5347(17)37478-5.
- Hadidi AT. Perineal Hypospadias: The Bilateral-Based (BILAB) Skin Flap Technique. Hypospadias Surgery 2014; 49 (1): 497–506. DOI: 10.1007/978-3-030-94248-9_32.
- Lanciotti M, Betti M, Elia A, Landi L, Taverna M, Cini C, et al.. Proximal hypospadias repair with bladder mucosal graft: Our 10 years experience. J Pediatr Urol 2017; 13 (3): 294.e1–294.e6. DOI: 10.1016/j.jpurol.2017.01.011.
- Pal DK, Gupta DK, Ghosh B, Bera MK. A comparative study of lingual mucosal graft urethroplasty with buccal mucosal graft urethroplasty in urethral stricture disease: An institutional experience. Urol Ann 2016; 8 (2): 157. DOI: 10.4103/0974-7796.172214.
- Pippi Salle JL, Sayed S, Salle A, Bagli D, Farhat W, Koyle M, et al.. Proximal hypospadias: A persistent challenge. Single institution outcome analysis of three surgical techniques over a 10-year period. J Pediatr Urol 2016; 12 (1): 28.e1–28.e7. DOI: 10.1016/j.jpurol.2015.06.011.
- Faure A, Heloury Y. Response to “Re: Faure A, Bouty A, Nyo L, O’Brian M, Heloury Y. Two-stage graft urethroplasty for proximal and complicated hypospadias in children: a retrospective study.” J Pediatr Urol 2016; 12 (5): 286 1–286 7. DOI: 10.1016/j.jpurol.2016.12.007.
- Sakr A, Elkady E, Abdalla M, Fawzi A, Kamel M, Desoky E, et al.. Lingual mucosal graft two-stage Bracka technique for redo hypospadias repair. Arab J Urol 2017; 15 (3): 236–241. DOI: 10.1016/j.aju.2017.06.002.
- Greenfield SP, Sadler BT, Wan J. The Two-Stage Repair for Severe Primary Hypospadias. Yearbook of Urology 1994; 2007 (2 Pt 1): 250. DOI: 10.1016/s0084-4071(08)70198-2.
- Retik AB, Bauer SB, Mandell J, Peters CA, Colodny A, Atala A. Management of Severe Hypospadias with a 2-Stage Repair. J Urol 1994; 152 (2 Part 2): 749–751. DOI: 10.1016/s0022-5347(17)32697-6.
- CHENG EARLY, KROPP BRADLEYP, POPE JOHNC, BROCK JOHNW. Proximal Division of the Urethral Plate in Staged Hypospadias Repair. J Urol 2003; 170 (4 Part 2): 1580–1584. DOI: 10.1097/01.ju.0000084258.93064.f4.
- Canning D. Faculty Opinions recommendation of Management of Proximal Hypospadias with 2-Stage Repair: 20-Year Experience. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (4): 1080–1085. DOI: 10.3410/f.725486894.793522961.
- Canning D. Faculty Opinions recommendation of Complications following Staged Hypospadias Repair Using Transposed Preputial Skin Flaps. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (2): 512–516. DOI: 10.3410/f.725364224.793522958.
- Tiryaki S, Əl\Elzschwakb\Elzschwarova VE, Dokumcu Z, Ergun R, Tekin A, Yagmur I, et al.. Unexpected outcome of a modification of Bracka repair for proximal hypospadias: High incidence of diverticula with flaps. J Pediatr Urol 2016; 12 (6): 395.e1–395.e6. DOI: 10.1016/j.jpurol.2016.04.046.
- Lin H, Wang Y-Y, Li S-B, Chen Z-T, Su L-J. Staged transverse preputial island flap urethroplasty for some proximal hypospadias with moderate-to-severe chordee. BMC Urol 2016; 21 (1): 1536–1540. DOI: 10.1186/s12894-021-00948-8.
- Hanna M. Faculty Opinions recommendation of Hypospadias: Are we as good as we think when we correct proximal hypospadias? Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2016: 1477513116300432–. DOI: 10.3410/f.726422269.793519822.
- Barbagli G, Sansalone S, Djinovic R, Lazzeri M. Surgical Repair of Late Complications in Patients Having Undergone Primary Hypospadias Repair during Childhood: A New Perspective. Adv Urol 2012; 2012 (705212): 1–5. DOI: 10.1155/2012/705212.
- Braga LH, Pippi Salle JL, Lorenzo AJ. Comparative Analysis of Tubularized Incised Plate Versus Onlay Island Flap Urethroplasty for Penoscrotal Hypospadias. Yearbook of Urology 2007; 2008 (1451-6): 246–247. DOI: 10.1016/s0084-4071(08)79119-x.
- Holland AJA, Smith GHH, Ross FI, Cass DT. HOSE: an objective scoring system for evaluating the results of hypospadias surgery. BJU Int 2001; 88 (3): 255–258. DOI: 10.1046/j.1464-410x.2001.02280.x.
- Merriman LS, Arlen AM, Broecker BH, Smith EA, Kirsch AJ, Elmore JM. The GMS hypospadias score: Assessment of inter-observer reliability and correlation with post-operative complications. J Pediatr Urol 2013; 9 (6): 707–712. DOI: 10.1016/j.jpurol.2013.04.006.
- F T, TP J, RP G. RE: Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A validation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients. J Pediatr Urol 2013; 9 (6): 1016. DOI: 10.1016/j.jpurol.2013.07.022.
- Weber DM, Schonbucher VB, Landolt MA, Gobet R. Faculty Opinions recommendation of The Pediatric Penile Perception Score: an instrument for patient self-assessment and surgeon evaluation after hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2008; 180 (1080-4): 1084. DOI: 10.3410/f.719560881.793500484.
Ultima atualização: 2025-09-21 13:35