
32: 近端型尿道下裂
阅读本章大约需要 10 分钟。
引言
尿道下裂的定义为:尿道外口开口位于阴茎体腹侧、相对于龟头顶端更近端的位置。正如上一章所述,尿道下裂按尿道外口的位置分为远端型、中段型和近端型。后部型(重度),约占20%的病例,其范围从阴茎体近端三分之一延伸至会阴。其还可进一步分为:后部阴茎型(位于阴茎体根部)、阴茎阴囊型(位于阴茎体根部、阴囊前方)、阴囊型(位于阴囊上或两侧生殖隆起之间),以及最为严重的会阴型(位于阴囊后方及生殖隆起后方,图 1).1 尽管尿道下裂的“远端、中段和近端”分型在历史上基于术前外口位置,但更准确的分型应在手术时进行,因为由于近端存在发育不良的尿道,外口的位置可能发生改变。重度尿道下裂常伴有称为阴茎腹侧弯曲(chordee)的阴茎弯曲、“帽状”或不完整包皮,以及尿道海绵体发育不良。Hypospadiology(尿道下裂学)这一术语由 John W. Duckett, Jr. 创造,指对该疾病各个方面的研究,是一个不断发展和扩展的学科。2 在美国,尿道下裂的发生率约为 1:200–300 例活产。3,4 近期发生率的升高可归因于早产、小于胎龄儿、低出生体重以及母亲年龄 ≥35 岁。1
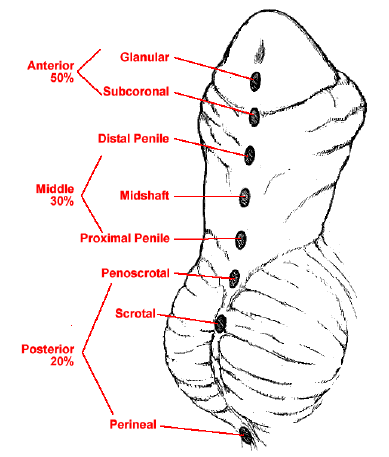
图 1 尿道下裂的临床表现谱。
胚胎学
男性外生殖器在妊娠第3rd个月时逐渐发育出可辨识的特征。正常情况下,泌尿生殖窦开口向生殖结节的腹侧延伸,形成尿道沟。原始泌尿生殖口和尿道沟的两侧由尿道褶皱所界定。5 生殖结节延长形成阴茎,尿道褶皱自泌尿生殖口向阴茎尖端开始融合,从而在第14周末形成阴茎尿道。阴茎海绵体于第7周在阴茎干内呈成对的间充质柱出现。尿道海绵体由包绕阴茎尿道的间充质团块分化而来。5 在近端尿道下裂的情况下,普遍认为这些尿道褶皱未能融合。由于管化过程受阻,阴茎腹侧相较于背侧出现差异性生长。
了解阴茎的解剖结构将极大地有助于理解尿道下裂的修复 (图 2).
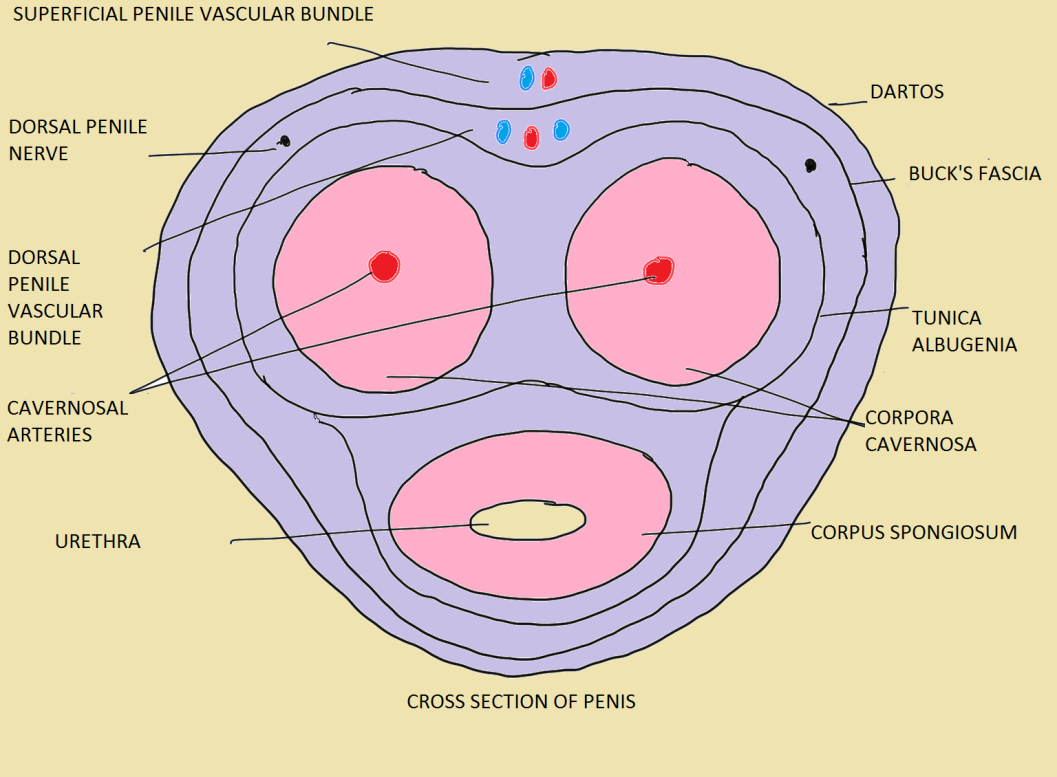 图2 正常成人阴茎的各层。6
图2 正常成人阴茎的各层。6
重度尿道下裂及其他相关的泌尿生殖系统疾病
由于共同的胚胎发育异常,近端尿道下裂更常与其他先天性疾病相关,即10%的病例合并隐睾症,7 多至32%的男孩合并腹股沟疝,8 多至27.3%合并性发育障碍9 以及前列腺小囊。
当存在重度尿道下裂并伴不可触及的睾丸时,必须排除性发育障碍(DSD)。10 在此类情况下,必须进行染色体核型分析。单纯的阴囊型尿道下裂就应引起对性发育障碍的怀疑,若合并双侧隐睾则更应高度怀疑。11 在以下情况应怀疑外生殖器不明确:伴不可触及性腺的尿道下裂;伴小阴茎且仅一侧或无可触及性腺的尿道下裂;新生儿具有女性外生殖器并在阴唇内出现性腺肿块,或存在阴唇融合和/或阴蒂肥大。12
评估
表 1 评估尿道下裂病例时的注意要点。6
| 病史 | 补充病史 | 体格检查 | 补充检查 |
|---|---|---|---|
| 年龄,以男性身份抚养 | 有声音改变、乳房发育史 | 牵拉阴茎长度 | 体貌(男性型或女性型) |
| 有从阴茎下表面排尿史 | 有母亲妊娠期摄入激素史 | 阴茎弯曲(无/轻度 <30˚/重度 >30˚) | 乳房发育(Tanner分期) |
| 阴茎腹侧弯曲 | 尿道下裂家族史 | 尿道口(狭窄/不狭窄) | 腋毛(有或无,男性型或女性型发育) |
| 尿流偏离中线或变细 | 有反复流产史或新生儿期急性病及呕吐史 | 尿道口位置(龟头部/冠状沟/阴茎远端/阴茎中段/阴茎近端/阴茎阴囊交界/阴囊) | 阴毛(有或无,男性型或女性型发育) |
| 有生殖器手术史 | 龟头(圆形/锥形) | 外生殖器不明确(DSD病例的Prader分期) | |
| 隐睾 | 尿道沟(浅/深) | ||
| 较大青少年期的勃起及弯曲史 | 尿道板(宽/窄/瘢痕化/柔软) | ||
| 包皮(背侧兜帽样/足以重建/缺如) | |||
| 睾丸位置 | |||
| 睾丸大小 | |||
| 阴囊(发育良好/阴茎阴囊转位/发育不良/阴茎阴囊蹼) |
此外,GMS(龟头、尿道口和阴茎体)评分似乎与手术并发症的风险相关。GMS评分基于龟头大小/尿道板质量、尿道口位置以及阴茎下弯程度。Arlen 等人 证明,总GMS评分每增加1分,发生任何术后并发症的可能性即出现统计学显著增加 表2.13 在其研究中,262名男童(平均年龄12.3 ± 13.7个月)接受了一期尿道下裂修复,平均GMS评分为7 ± 2.5(G 2.1 ± 0.9,M 2.4 ± 1,S 2.4 ± 1),平均临床随访时间为17.7 ± 9.3个月。共发现37名男童出现了45例并发症。观察到总GMS评分与任何并发症发生之间存在显著关系(p < 0.001);GMS评分每增加1分,任何术后并发症的发生比值比增加1.44倍(95% CI, 1.24–1.68)。13 在239例单期修复中,观察到21例(8.8%)发生尿道皮肤瘘,为最常见的并发症。轻度(GMS 3–6)、中度(GMS 7–9)和重度(GMS 10–12)尿道下裂的瘘发生率分别为2.4%、11.1%和22.6%(p < 0.001)。此外,多变量分析显示,下弯程度是瘘的独立预测因子。发现腹侧弯曲>60°的患者发生瘘的可能性是无弯曲患者的27倍(95% CI, 3.2–229)。13
表 2 GMS 评分。13
| 龟头 (G) 评分 | 尿道口 (M) 评分 | 阴茎体 (S) 评分 |
|---|---|---|
| 1. 龟头大小良好;尿道板健康,沟状明显 | 1. 龟头部 | 1. 无阴茎下弯 |
| 2. 龟头大小适中;尿道板尚可,有沟状 | 2. 冠状沟 | 2. 轻度(< 30°)阴茎下弯 |
| 3. 龟头较小;尿道板狭窄,部分纤维化或扁平 | 3. 阴茎体中段或远端 | 3. 中度(30–60°)阴茎下弯 |
| 4. 龟头极小;尿道板不清晰,非常狭窄或扁平 | 4. 阴茎体近端,阴茎阴囊部 | 4. 重度(> 60°)阴茎下弯 |
对尿道板的评估也很重要,因为狭窄的尿道板预示着较差的预后(图3)。指导我们决定如何修复近端型尿道下裂的两个主要因素是尿道板的质量,以及(或许更为重要的)存在的腹侧弯曲程度。
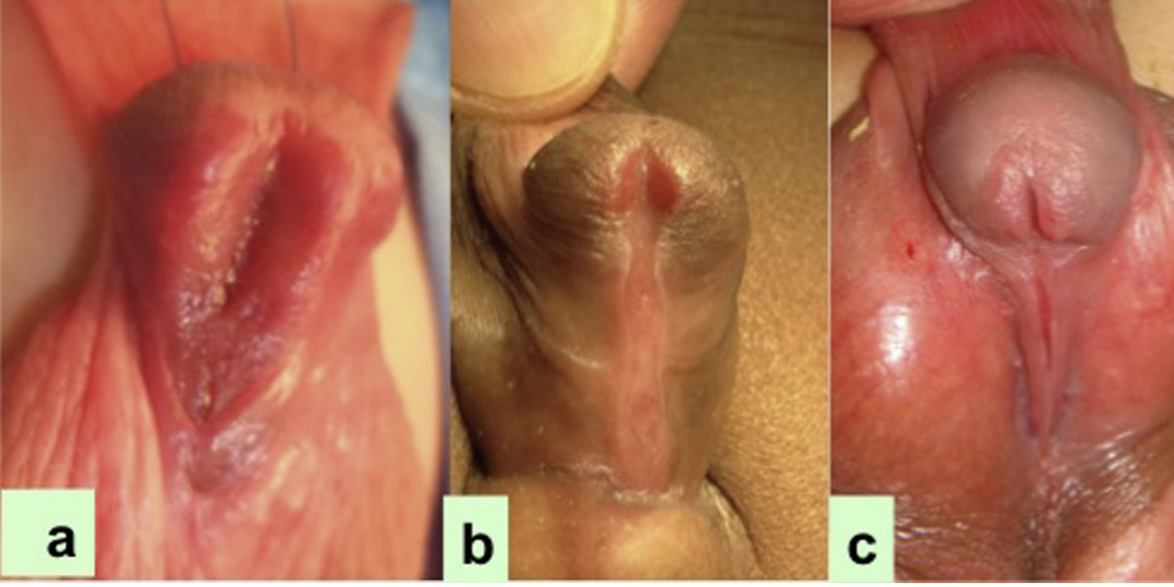
图 3 在近端型尿道下裂患者中,尿道板的宽度从 a 到 c 减小。14
检查
影像学检查
- 在近端尿道下裂病例中应行超声检查,以排除伴发的肾脏畸形,尽管此类畸形极为罕见。12 如有反复尿路感染病史,应进行排尿性膀胱尿道造影。另外,在真正的外生殖器不明确病例中,MCU 可帮助评估是否存在苗勒管残余。这些患者通常无症状,不需要常规手术切除这些残余。偶尔因反复尿路感染、滴尿或结石形成,可能需要切除前列腺小囊。12 为近端尿道下裂患者手术时,前列腺小囊有时会妨碍导尿管进入膀胱,使导尿管更倾向于停留在小囊内。可通过以下方法处理:i) 双导管法,其中第一根导管误入前列腺小囊,然后经尿道外口置入一根更小号的 French 导管,后者几乎总是进入尿道;ii) 使用 Clutton sound 引导尿道导管;iii) 在困难病例中,可先在膀胱镜辅助下将软导丝置入膀胱,然后沿导丝推进一根开放端导管进入膀胱。15
核型分析
AUA 隐睾症指南建议,所有合并单侧或双侧隐睾且具有重度近端尿道下裂的男孩,应接受额外检查以排除性发育异常(DSD),因为在这些情况下其发生率显著更高。9,10 2006年发布的指南将重度尿道下裂纳入为46,XY DSD的一种形式。16 对于合并尿道下裂且睾丸不可触及的男孩,对DSD的担忧尤为强烈。Kaefer 等人10研究了79例有尿道下裂和隐睾病史的患者。无论单侧还是双侧,睾丸不可触及者被确诊合并DSD的风险增加三倍(约50% vs. 15%)。与远端尿道下裂相比,近端尿道下裂的DSD风险显著增高(64% vs. 7%)。10 正常的46, XY 核型可能具有误导性,尤其在最重型的男孩中。作者也倾向于对这类合并重度尿道下裂和UDT的患者进行核型分析。
术前雄激素
术前使用二氢睾酮(DHT)或睾酮,可通过局部应用,或更常见地通过肌内注射进行,能够增加阴茎的长度和宽度,并可使龟头尺寸增大。对于小阴茎患者,睾酮已被证明有助于促进阴茎生长。不同机构的应用方案可能有所差异。建议将2%丙酸睾酮乳膏每日3次局部涂抹于阴茎,连续3周。12 这种睾酮给药途径易于实施,且反应良好。然而,疗效存在差异,取决于每日用药的依从性以及实际涂抹的药量。过量可能导致全身性吸收,极端情况下可出现声音变低和男孩的行为改变。至少应在手术日期前3周停止局部用药。肌肉注射睾酮按2 mg/kg/次,共3次、每次间隔3周,最后一次至少在手术日期前2周完成,是一种更为可靠的给药途径。
手术知情同意
在就计划中的手术以及最适用于个体病例的可能替代方案提供适当、充分且及时的信息之后,必须取得充分知情的书面同意。很多时候,手术方案可能会根据麻醉下检查的结果而改变,因此,应当事先将各种手术选项的可能性告知家长。必须清楚说明预期疗效、美容外观结果以及可能的并发症(瘘管形成、狭窄或裂开)。对于近端型尿道下裂,家长必须明白孩子很可能需要分期修复。因此,有必要让家庭和患儿为恰当的手术做好准备,进行准确的解剖学评估,并就手术结局和潜在并发症进行坦诚的讨论。7
手术时机
美国儿科学会 [AAP]7,17 建议将初次择期修复手术的时间安排在生后6至12个月之间,该建议基于多项研究,这些研究强调需要在以下因素之间取得平衡:手术可能带来的不良心理影响、对患儿的麻醉风险、可促进成功修复的阴茎发育程度,以及随着男童年龄增长而出现的伤口愈合差异。18 Belman 等人 表明,与在较大年龄接受修复的男童相比,12个月龄之前接受修复的男童焦虑更少,且性心理结局更佳。19
重建的目标
- 实现以正常速度且呈层流的排尿,
- 在阴茎笔直的情况下获得令人满意的性功能,并且
- 从美容角度实现裂隙样外尿道口并使龟头对合良好。20
重建的阶段
- 腹侧弯曲矫正
- 尿道成形术
- 龟头成形术
- 皮肤覆盖
手术修复技术
在近端尿道下裂中,这些最常通过分期修复来实现。关于近端尿道下裂修复有两种观点:
- 皮瓣的应用
- 分期移植手术
这些取决于腹侧弯曲的矫正情况。极少数情况下,皮肤脱套后不再存在进一步的腹侧弯曲,此时可选择切开尿道板管状化(TIP)修复或贴敷岛状皮瓣进行尿道成形术,但由于远期并发症,长段TIP修复较少采用。如果仍有残余弯曲,一些外科医生倾向于分期修复:第一期切断尿道板并置入包皮移植片,如不可得则置入口腔黏膜移植(BMG),第二期将移植片管状化。若皮肤脱套后腹侧弯曲仍超过30度,则在第一期进行弯曲矫正,可采用鞘膜瓣(TVF)、鞘膜移植(TVG)、SIS、真皮,或按Snodgrass21所述的多处横向海绵体切开术。随后根据腹侧弯曲矫正所采用的技术,在第二期或第三期行尿道成形术。
简而言之,如果在皮肤去套剥离后,存在阴茎下弯< 30, 则有2种选择:TIP修复(多数外科医生并不首选),以及仅背侧皮瓣。
如果阴茎弯曲 > 30˚,则将尿道板(UP)离断。若离断后无弯曲,可采用背侧包皮瓣作为嵌入式或管状化(按 Duckett 法),也可使用包皮或BMG移植物。
阴茎腹侧弯曲的矫正
阴茎下弯概述
无论采取分期还是一期手术,阴茎下弯的矫正都是修复近端尿道下裂最重要的初始步骤。在第一阶段,去套样剥离阴茎皮肤后,通过人工勃起试验评估阴茎弯曲程度。若用直尺或量角器测得弯曲角度超过30°(图4),下一步应切断尿道板,通常在靠近龟头水平的远端进行。在此阶段,纠正腹侧弯曲,修复阴茎阴囊移位,去套剥离阴茎体皮肤,并切断尿道板以矫正弯曲。
Moscardi et al.22 指出,仅通过去套剥离阴茎、处理缩短的腹侧皮肤以及腹侧纤维化的Dartos筋膜,就可使相当比例的阴茎弯曲得到解决。Braga et al.23 回顾了在137例尿道下裂患者中剥离皮肤及Dartos筋膜后阴茎弯曲的纠正率7,其中9例为轻度(<30°)、44例为中度(30–45°)、85例为重度(>45°)。在去套剥离阴茎后,轻度、中度及重度弯曲组的完全矫正率分别为70%、30%和2.4%。23
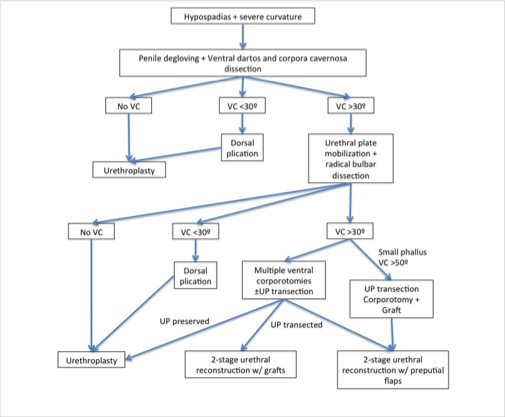
图 4 阴茎近端型尿道下裂伴阴茎弯曲患者的管理。22
阴茎下弯程度的测量
阴茎体的矫直程度通过人工勃起试验(即 Gittes 和 McLaughlin 技术)进行测量。24 在该试验中,通过细针(25–27 号)向阴茎海绵体的侧方或向龟头内注射生理盐水,并在阴茎根部放置止血带 (图 5).
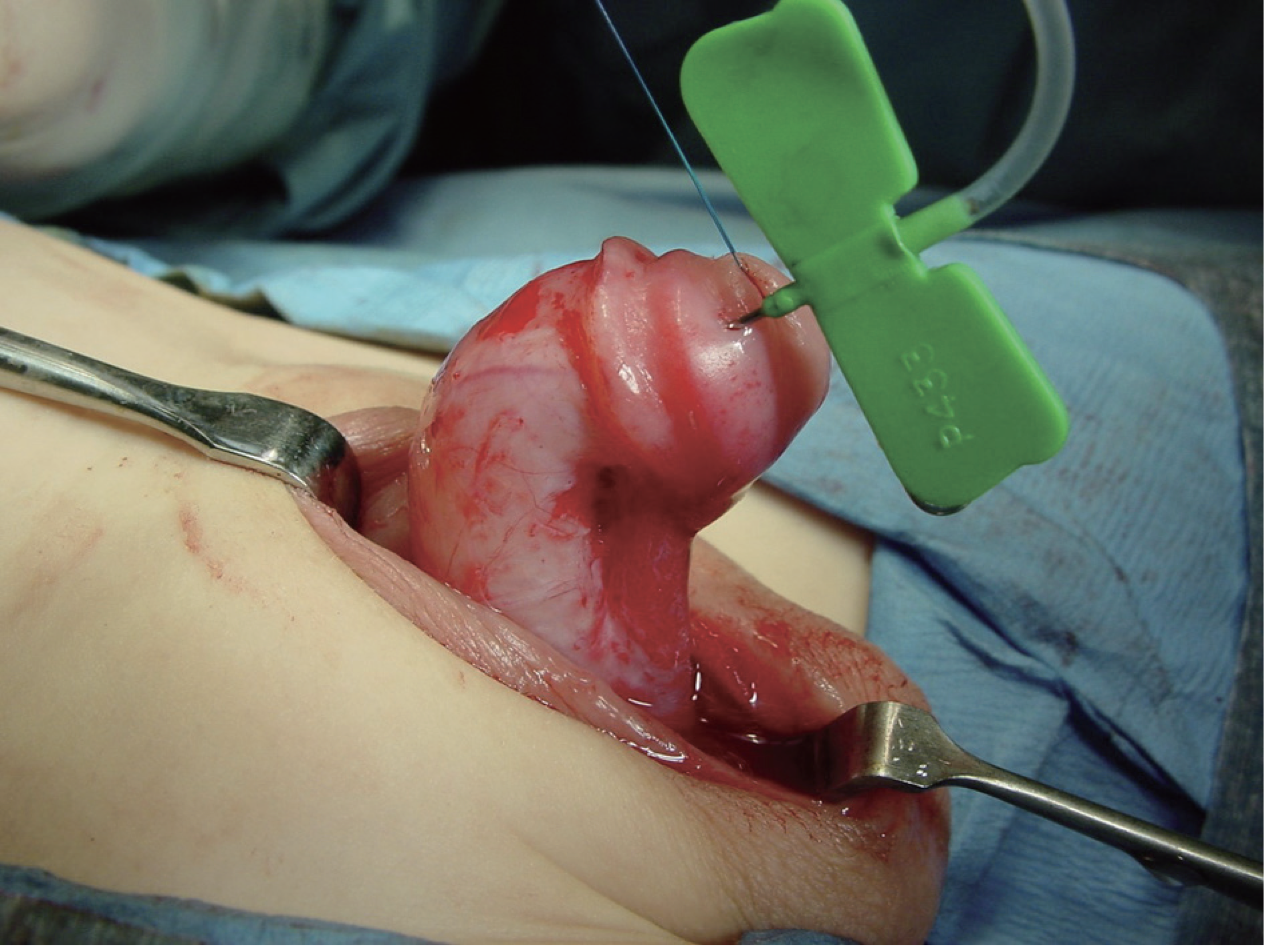
图 5 术中阴茎弯曲程度的测量。
然而,在相当高比例的近端型尿道下裂中,去套剥离后,若人工勃起显示超过30度的弯曲,则在靠近龟头的远端将UP切断,并游离近端尿道,以使阴茎变直、改善阴茎长度,并避免因短而纤维化的尿道板导致的回缩。22 阴茎延长技术包括在阴茎海绵体白膜腹侧进行多处横行切开,或进行单一横行切开并应用鞘膜瓣或移植物、SIS移植物,或真皮移植物 (图 6).

图 6 采用海绵体切开术矫正阴茎弯曲,并以SIS移植物覆盖创面。
Up 切开后残余的阴茎下弯
在切断UP后进行人工勃起试验仍存在阴茎弯曲的情况下,处理残余弯曲有两种方法:其一为海绵体切开术,即在腹侧行3个横向切口,切口不很深,且不以任何移植物覆盖;另一种方法(作者亦采用)为行一个大的横向切口,然后以真皮移植片、SIS、TVG或TV FLAP覆盖(图7)。21
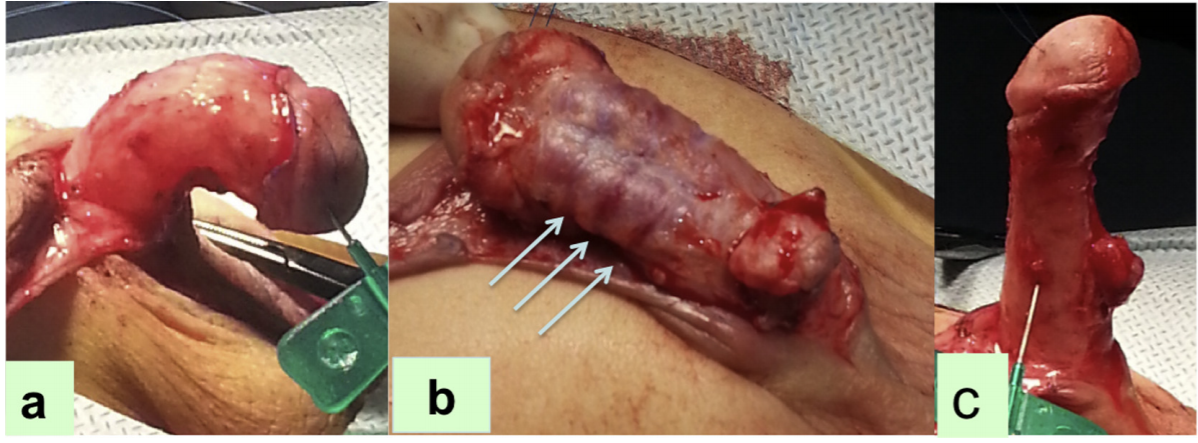
图 7 (a) 人工勃起试验显示阴茎下弯的程度,(b) 多个横向海绵体切开术,(c) 在重复测试时阴茎弯曲被矫直。 [来源:An alternative for ventral lengthening in children with severe penile curvature that allows graft coverage during staged hypospadias repair. Bruno Leslie, Bryce Weber, Rodrigo Romao, Walid Farhat, Darius Bagli, Armando Lorenzo, Joao Pippi Salle. J Urol 第 221 卷,第 11 页,2011]
在第一种技术中,于腹侧进行三处横向海绵体切开,首先在最大弯曲点从4点到8点,另外两处分别在距第一处近端5 mm和远端5 mm处,切开穿过白膜直至可见海绵体组织,然后再次进行测试。这些切口可在近端游离后用原有的近端尿道覆盖,或用包皮移植物或BMG覆盖。21,25
Snodgrass 对43名近端尿道下裂且在去套剥离后腹侧弯曲≥30°的男孩进行了研究,并行尿道板切断。对于仍持续腹侧弯曲≥30°者,为矫直而在腹侧行3处海绵体切开,未进行海绵体移植修补。分期移植性尿道成形术采用包皮或唇黏膜。21,25,26 结果显示,平均腹侧弯曲角度为70°,其中65%接受了海绵体切开,88%使用包皮移植;其余患者的海绵体切开处以真皮移植覆盖。未报告这些患者出现腹侧弯曲复发,然而在随访中有10例(23%)发生并发症,9例接受了再次手术。26 据此,现行的 STraighten And Close(STAC)尿道下裂修复或 Straighten and Graft(STAG)的理念已由 Snodgrass 和 Bush 推广开来(图 8)。

图 8 分期管状自体移植(STAG)修复术。(A)第一期手术时,经阴茎白膜在腹侧行1至3处海绵体切开,其中中间切口位于最大弯曲点的对侧。(B)标记并切取包皮移植片。(C)将包皮移植片置于阴茎干腹侧,随后缝合固定到位(D)。底部面板显示修复术的第二期。(E)标记尿道成形术切口,并沿阴囊正中线向下延伸。(F)分离形成龟头翼。(G)行两层尿道成形术,随后以鞘膜作为屏障层覆盖。(H)关闭后的外观 [摘自:Snodgrass W: Staged tubularized autograft repair for primary proximal hypospadias. J Urol 198:680–686, 2017]。
皮瓣存在所述的局限性:其边缘血供受限,由于与下方海绵体的固定较差,狭窄发生的机会更多,憩室形成的发生率也更高。这些缺点可通过移植技术加以克服;移植物获得较为均匀的血供,并能很好地固定于下方海绵体,因此分别降低了狭窄形成和憩室形成的风险。Moscardi et al 提出的流程图有助于针对伴近端尿道下裂的重度阴茎弯曲患者实施个体化管理(图 4)。22
背侧褶皱术
在部分患者中,当弯曲仍然存在或仅有龟头倾斜,或阴茎下弯小于30°时,可行背侧褶皱术,此术式先前由Baskin推广。目前,大多数外科医生实施Nesbit手术或改良Nesbit手术。在该技术中,于最大弯曲点切除背外侧阴茎白膜的菱形楔形组织,随后用不可吸收缝线(如proline)横向缝合该缺损。27 已报道对此技术的多种改良,包括在不切除阴茎筋膜的情况下进行背侧褶皱。
一期尿道下裂修复术
这通常包括行背侧褶叠缝合以矫正阴茎腹侧弯曲,并结合多种不同的尿道成形术技术,具体取决于修复所用的组织;包皮皮肤;局部皮肤;或颊黏膜移植。7 一些一期尿道下裂修复术包括:
横向包皮岛状皮瓣(Duckett 管);28 在该术式中,取用包皮岛状皮瓣,并将其管状化用于替代性尿道成形。此术式由 Asopa 修改,29 即并非在将皮瓣固定于阴茎干之前先行管状化,而是将皮瓣左侧固定于阴茎干腹侧,位于中线左侧。7 随后采用间断 Lembert 缝合在中线关闭皮瓣,可降低修复层下方上皮暴露的风险。缝线延伸至龟头中部。随后,小心将皮瓣覆于缝合线之上,并将龟头两翼覆盖于尿道成形与带血供的皮瓣之上。管状化皮瓣的基底固定于原生尿道的远端范围(图 9)。2,7 实施双层管状化,始终保持均匀的管腔口径。对于在皮肤分离及尿道板离断后纠正了严重弯曲的患者,此方法可能有帮助。7
Onlay 岛状皮瓣术:OIF 适用于在阴茎去套剥离后弯曲畸形得以矫正的男孩,且对于相对较薄、否则无法成管化的尿道板,无需行切开。7 该术式及其他一期尿道下裂修复技术的要点如下。
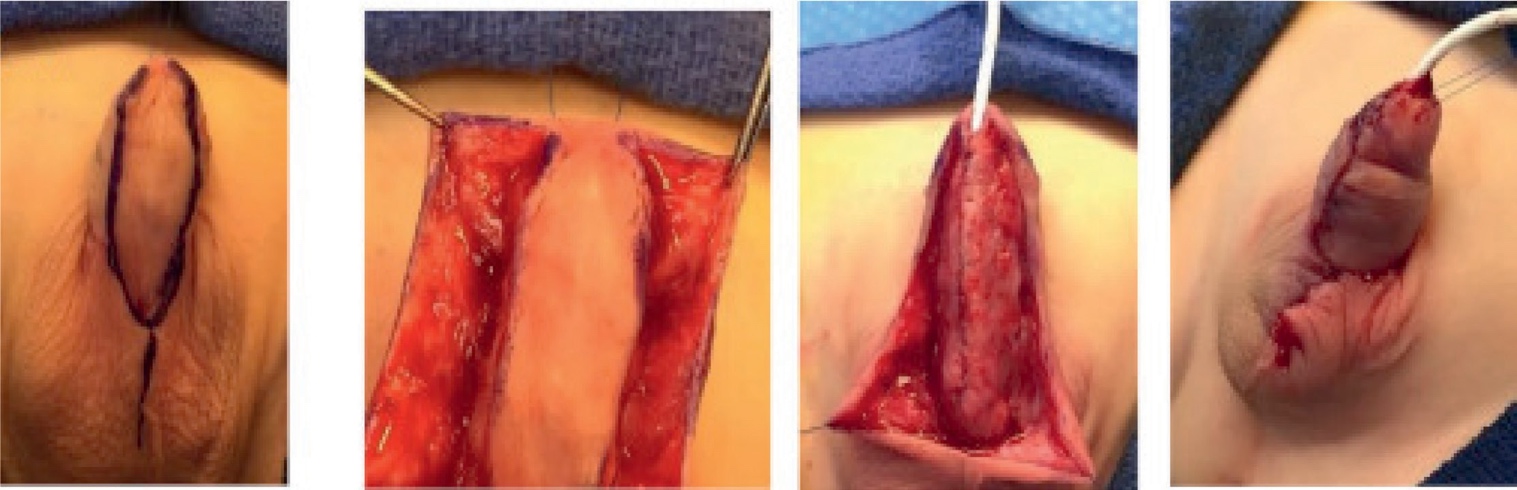
图 9 岛状管型尿道下裂修复术。 (A) 术前外观。粉红、光亮的腹侧皮肤提示腹侧尿道海绵体变薄。尽管为冠下尿道口,这仍属近端型。 (B) 脱套剥离后,尿道口位于阴茎阴囊交界处,并以 8-Fr 饲管插管。 (C) 背侧褶皱缝合后行人工勃起试验显示无残余阴茎弯曲。 (D) 游离包皮岛状皮瓣,同时沿阴茎体皮肤向阴茎根部分离并获取柔软的达托氏筋膜蒂。 (E) 将皮瓣一侧锚定于白膜。 (F) 将皮瓣修剪至宽 12 mm,切除多余上皮。随后于分流管上闭合皮瓣,使上皮缘与此前锚定的皮瓣部分对合。 (G) 修复完成。 [引自 Kraft KH, Shukla AR, Canning DA: 尿道下裂。Urol Clin North Am 2010; 37: 167–181.]
旁置岛状皮瓣
- 从包皮内板制备岛状皮瓣
- 尿道板与皮瓣的合并宽度应为12 mm或更小,并据此修剪;尤其应将近端皮瓣变窄,以防在新生尿道与原生尿道吻合处形成憩室
- 背侧皮肤的血供不依赖于皮下组织
- 可用于阴囊/会阴型尿道下裂
- 无狭窄
- 瘘发生率降至15%
外侧蒂
- 在近端型尿道下裂伴轻度阴茎下弯的情况下30
- 龟头较小或扁平
- 皮瓣宽度由尿道板决定
- 将皮瓣远端缝合于距龟头尖端2mm处
- 在与右侧缘分离之前,先缝合左侧缘
管状化岛状皮瓣修复术
- 需要切除尿道板的重度尿道下裂病例
- 管状化尿道板背腹转移尿道成形术(DVTPTU)
- 憩室发生率高
- 瘘形成发生率低
延长型TIP尿道成形术
- 描述于这样一种情形:一名男童,其阴茎弯曲可通过皮肤分离或褶皱缝合予以矫正,且具备适宜的尿道板31
- 为扩大其适用性,在去手套样剥离后仍存在超过30度的持续腹侧弯曲时,可采取技术改良,包括尿道板游离和横向海绵体切开。
- 然而,Snodgrass et al.32 的分析提示,过于激进的尿道板游离可能导致血运受损,从而增加狭窄形成的风险,最终限制了在合并阴茎弯曲的重度尿道下裂中近端TIP的适用性。由于并发症风险更高,该技术此后已不再受青睐,而改用其他两期修复方式,如Byars皮瓣或STAG修复。
两期尿道下裂修复术
重度尿道下裂最常实施的术式
- Byars 两期修复术:
- 在第一期
- 阴茎弯曲矫正
- 行阴茎矫直,切除腹侧牵拉的尿道板
- 将分裂背侧皮肤形成的包皮皮瓣旋转以覆盖腹侧缺损
- 广泛开放龟头并放置足量的皮瓣
- 在第二期
- 将该区域管状化为尿道管
- 至少在第一期术后6个月进行
- 在第一期
Shukla 等人 在11年期间对700名男童采用Byars皮瓣技术进行近端尿道下裂修复。33 他们报告其中21例(3%)发生瘘管。无一例出现完全断裂、尿道憩室或尿道外口狭窄。在其系列中,我们研究的患者年龄范围为3–12岁,第二期手术在第一次手术后至少1年实施。作者强调了Byars皮瓣的优点:1)作为带血供的皮瓣,他们认为用于第一期时可靠;同时,尚有充足的带血供皮肤可用于覆盖因阴茎弯曲矫正所形成的创面,2)手术完成后可获得包皮环切样外观,3)与移植不同,他们的研究未报告收缩或丢失。33
- 两期 Bracka 颊黏膜/包皮移植尿道下裂修复术34
- 在第1期 (图 10):
- 既往瘢痕组织(如有)予以切除
- 龟头翼予以动员
- 将颊黏膜移植片或游离包皮移植片缝贴固定以覆盖切除瘢痕后的腹侧区域
- 颊黏膜供区通常为口唇或颊部
- 不建议对取材后形成的黏膜缺损进行缝合。
- 在第2期:
- 将尿道板卷管成形,通常在 6 个月后完成
- 是进行尿道成形术翻修的良好术式
- 在第1期 (图 10):
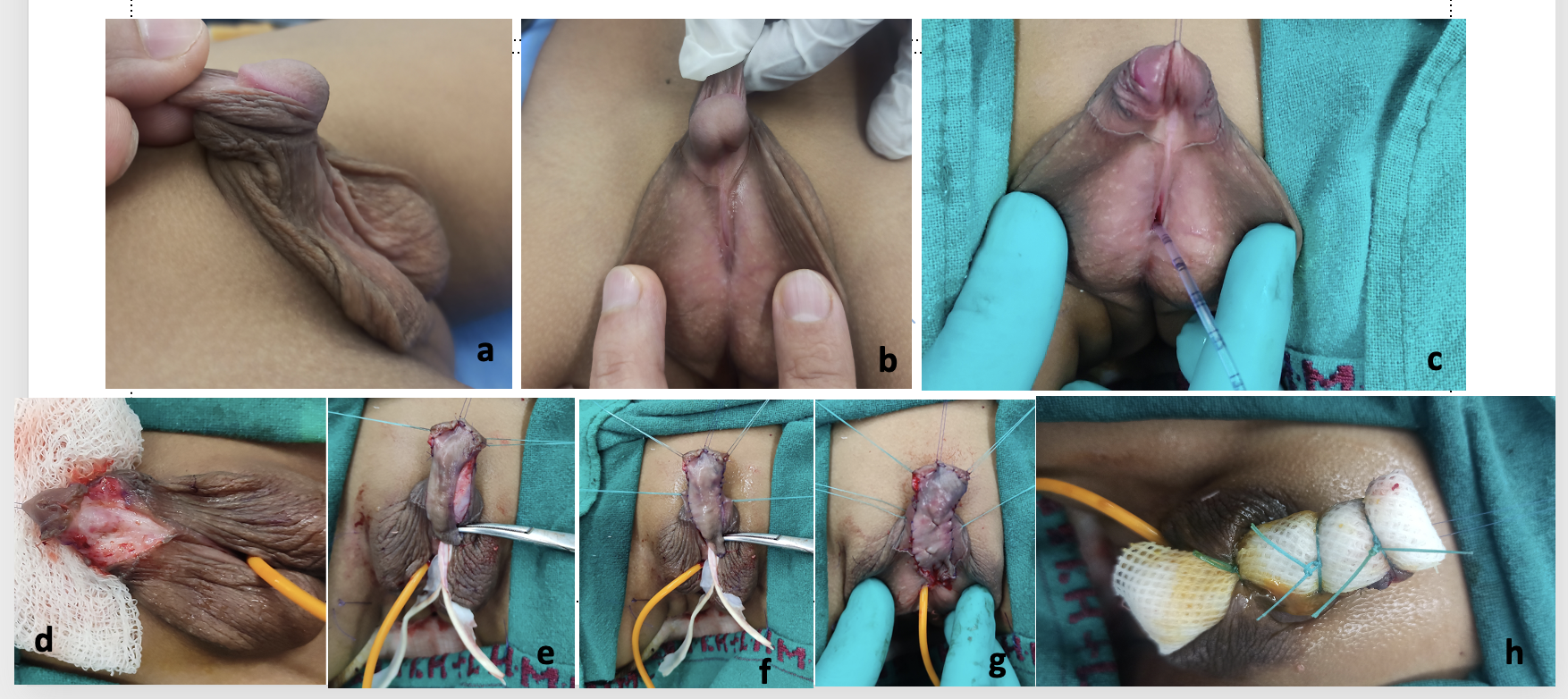
图 10 图片致谢 Dr. Vikram Khanna,新德里 Lady Harding Medical College 和 Kalawati Saran Children’s Hospital 小儿外科副教授,a) 术前照片显示阴茎阴囊型尿道下裂伴阴茎阴囊转位、阴茎下弯、阴茎短小及背侧帽状包皮,b) 侧位显示阴茎下弯程度及尿道板,c) 采用双导管法将饲管作为支架插入
d) 阴茎体脱套并矫正阴茎下弯,e) 取包皮皮肤移植片,f) 将移植片缝合于分开的龟头翼之间及尿道板与阴茎海绵体区域,g) 对移植片完成绗缝固定,h) 在移植片上行系带加压敷料固定,并将导管留置体内 1 周。
Bracka 描述了两期尿道下裂修复的概念。34 在第一期修复术后至少6个月即可进行第二期手术。在该次手术中,矫正任何残余的阴茎弯曲,进行移植片的管状化,构建新尿道,并完成尿道口成形术和龟头成形术。尿道成形术以达尔托斯筋膜瓣或鞘膜瓣覆盖。在当今时代,这一方法已被广泛接受为近端型尿道下裂伴阴茎弯曲患者的主要治疗。Bracka 报道的两期尿道下裂修复系列共纳入457名儿童(369例初次修复,88例继发或挽救性修复)和143名成人(22例初次修复,121例继发修复),其中5.7%35 发生尿道皮肤瘘,7%14 出现狭窄,4.6%29 出现晚发性狭窄。34,35
来自包皮内板的皮肤作为移植材料是极佳的选择,因为移植物薄、柔韧、无毛,且能耐受湿润环境。取材后去除达氏筋膜(dartos)层,然后将其腹侧吻合于阴茎海绵体以形成新尿道板。移植物的管状化一般在6个月后再进行。其中一个问题
关于包皮移植物的问题是该移植物的可获得性。这是因为许多患有近端尿道下裂并伴腹侧弯曲的患者阴茎皮肤匮乏,而且在初期阶段,所有皮肤都需要并被用于阴茎表面重建。尽管在尿道下裂修复中使用移植物多用于再手术,但也有一些病例系列报告称,在初次近端尿道下裂矫治中采用包皮移植物进行分期修复同样取得了良好结局。36,37
在包皮皮肤不能使用或不可获得的情况下,可自颊内侧和/或下唇齿槽区取颊黏膜(图 11),并将其移植至阴茎海绵体。其特性包括弹性蛋白含量更高、相对的刚性可提供良好支撑,并最终减少尿道憩室和尿道口脱垂的发生,38,39 使其适用于尿道下裂手术。取颊黏膜移植片时,应避免跨越口角进入下唇,从而避免面部美容畸形。其次,从颊内侧取黏膜时,应注意避开腮腺管(Stensen 管)。
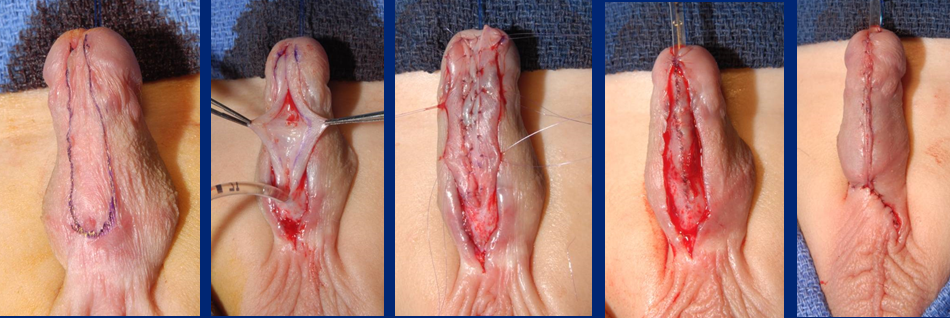
图 11 颊黏膜嵌入移植片的管状化
根据现有文献,在原发病例中,包皮移植物是首选方法,其他可用的移植物包括舌黏膜移植和颊黏膜移植。40,41 在近端尿道下裂病例中,大多数情况下,我们可以使用包皮黏膜(并非真正的包皮皮肤,且表面光亮)作为移植物,并且在第一期我们不会发现皮肤不足,因为在移植物置入的第一期,我们并不以皮肤覆盖阴茎。
在一项包含43名完成两期手术并进行了术后随访的男童的系列研究中,Snodgrass 和 Bush 得出结论:对于最严重的近端尿道下裂,分期管状化自体移植术在77%的男童中可获得阴茎变直并形成位于正常位置的新尿道口。26 在因并发症进行1次或2次再次手术后,该比例升至98%。在他们的系列中,还发现于未行海绵体补片的情况下实施3处海绵体切开术后未见腹侧弯曲复发 [Snodgrass]。这些患儿的阴茎平均腹侧弯曲为70度,65%的病例行海绵体切开术,88%的病例使用了包皮移植。26
术后管理与护理
尿液引流
术后应留置婴儿喂养管以确保引流。我们通常对幼儿使用6F或8F的IFT,对年长儿童、青少年和成人使用10F至12F。置管时应注意将支架尖端置于膀胱内,既避免因刺激膀胱三角区而引起膀胱痉挛,也避免因导尿管留置过长而在体内打结。最佳选择是使用硅胶导尿管。
敷料
在对修复后的阴囊区域进行充分垫衬后,将敷料以环形方式包覆于阴茎轴周围。敷料不应过紧也不应过松,并且龟头顶端应可见或暴露,以便在术后期间进行目视检查。
另一种选择可以是覆盖敷料,并用无菌塑料薄膜敷贴或Elastoplast的三明治式敷料将其固定在腹壁上。
在分期修复中,当于第一期使用移植物时,我们采用缝线捆扎加压敷料(图10)来固定移植物,并于一周后拆除。移植物通过绗缝缝合固定于其下方的阴茎海绵体。该缝线捆扎加压敷料有助于消除移植物与下方海绵体之间的任何潜在腔隙,清除多余液体,并促使移植物组织更好贴合。
并发症
修复后的主要并发症简要概述可大致分为与尿道成形术相关的并发症和与皮肤相关的并发症。7
尿道成形术并发症
- 瘘
- 龟头裂开
- 尿道口狭窄的梗阻症状(用力排尿、排尿时间延长、尿路感染和/或尿潴留)
- 尿道狭窄
- 尿道憩室
皮肤并发症
- 皮肤坏死
- 阴茎扭转 > 30 度- 正常与真正垂直的龟头平面之间的角度距中线 >30 度 (注明顺时针或逆时针)
- 包皮瘘 - 包皮皮肤中的瘘样缺损,与尿道腔不相通
- 包皮重建后包皮裂开: 包皮皮肤的缺损,形成不完整的包皮
- 硬化性苔藓
这些还可界定为早期并发症,表现为龟头缺血、包皮瓣坏死、导尿管阻塞、导尿管过早脱出以及伤口感染。晚期并发症包括尿道皮肤瘘形成、龟头裂开、尿道口狭窄、复发性或残余阴茎弯曲、尿道狭窄、尿道裂开以及尿道憩室。
表3 已突出标示各种两期移植研究的并发症,a 仅有48例(共140例)采用包皮移植物行两期手术治疗,b 15例(30%)出现多种并发症,c 44例为初次病例,8例为翻修(再手术)病例。
| 研究 | 患者人数 | 平均随访(月) | 尿道口位置 | 修复类型 | 总体并发症(%) | 尿道口狭窄(%) | 裂开(%) | 尿道狭窄(%) | 尿道憩室(%) | 尿瘘(%) | 残余弯曲(%) | 其他 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferro, 200236 | 34 | 1–48(范围) | 近端 | 两期 包皮移植 | 8 (24%) | 0 | 4 (11.7%) | 1 (3%) | 1 (3%) | 2 (6%) | — | — |
| Johal, 200637 | 62 | 26(中位数) | 中段/近端 | 两期 移植 | 11 (18%) | 3 (5%) | 3 (5%) | 0 | 0 | 0 | 3 (5%) | 尿流偏斜 2 (3%) |
| Pippe Salle, 201614 | 48a | 29.6(中位数) | 近端 | 两期 移植 | 16 (33.3%) | 0 | 7 (14.5%) | 1 (2%) | 1 (2%) | 5 (10.4%) | 2 (4.1%) | — |
| Faure, 201642 | 52 | 34(中位数) | 近端/翻修 | 两期 移植(包皮/BMG) | 20 (38.4%) | 8 (15.3%) | 1 (1.9%) | 4 (7.6%) | 1 (1.9%) | 8 (15.3%) | 0 | — |
| Sakr, 201743 | 23 | 12 | 翻修 | 两期(舌黏膜移植) | 3 (13%) | 0 | 1 | 0 | 0 | 2 | 0 | — |
| Snodgrass, 201726 | 43 | 22 | 近端 | 两期 | 10 (24%) | 0 | 7 (16.2%) | 0 | 1 (2.3%) | 2 (4.6%) | 0 | — |
| Lanciotti, 201740 | 50 | 63.6 | 近端 | 两期(膀胱移植) | 23 (46%)b | 4 (8%) | 0 | 15 (30%) | 6 (12%) | 9 (18%) | 5 (10%) | 尿道口脱垂 7 (14%) |
表4 各种两期皮瓣修复研究的并发症已被突出显示。a 结合远端TIP与管状化Byars皮瓣的两期技术,b - 在两期过程中通过人工勃起对VC重新评估,c 37例分两次分期,d 6例采用膀胱管、颊黏膜移植物等,e 仅有12例(共140例)使用两期包皮皮瓣处理,f 81例(共167例)使用两期包皮皮瓣处理,TPIF=横向包皮岛状皮瓣;BILAB=双侧蒂皮瓣。
| 研究 | 患者人数 | 平均随访(个月) | 尿道口位置 | 修复类型 | 总体并发症(%) | 尿道口狭窄(%) | 裂开(%) | 尿道狭窄(%) | 尿道憩室(%) | 尿瘘(%) | 残余阴茎弯曲(%) | 其他 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Greenfield, 199444 | 39 | 16 | 龟头下至会阴 | 两期皮瓣(belt-fuqua) | 16 (41%) | 0 | 0 | 7 (17.9%) | 8 (20.5%) | 1 (2.5%) | — | - |
| Retik, 199445 | 58 | — | 阴囊/会阴 | 两期皮瓣 | 3 (5%) | 0 | 0 | — | — | 3 (5%) | — | - |
| Cheng, 200346 | 14 | 6–36(范围) | 近端 | 两期a | 4 (28.5%) | 0 | 0 | 0 | 2 (14%) | 1 (7%) | 0b | 尿道口退缩 1(7%) |
| Hadidi, 201439 | 63c | 43 | 会阴 | 单期/两期 BILAB | 9 (14.2%) | — | 3 (4.7%) | — | 2 (3%) | 1 (1.5%) | — | 瘢痕挛缩 3(4.7%) |
| McNamara, 201547 | 134d | 45.6(中位数) | 近端 | 两期皮瓣 | 71 (53%) | 17 (12.7%) | 19 (14.2%) | 16 (11.9%) | 12 (9%) | 39 (29.1%) | 3 (2.2%) | - |
| Stanasel, 201548 | 56 | 38.6 | 近端 | 两期皮瓣 | 38 (68%) | 5 (9%) | 3 (5%) | 8 (14%) | 8 (14%) | 32 (57%) | — | - |
| Tiryaki, 201649 | 34 | 44.8 | 近端 | 两期 Byars 皮瓣 | 32 (95%) | 0 | 0 | 0 | 24 (70%) | 23 (67%) | 1 (3%) | 27 尿道脱垂 |
| Pippe Salle, 201614 | 12e | 29.6 | 近端 | 两期皮瓣 | 4 (41.6%) | 0 | 3 (25%) | — | 0 | 2 (16.6%) | 1 (8.3%) | - |
| Chen, 201650 | 87 | TPIF - 38(中位数)Byars – 36(中位数) | 近端 | 分期 TPIF,42 2-Stage Byars flap45 | TPIF 9.5%, Byars 33% | — | 0, 3 (6.6%) | 1 (2.3%), 2 (4.4%) | 1 (2.3%), 0 | 2 (4.6%), 10 (22.2%) | 0b,0b | - |
| Long, 201736 | 81f | 27.7(中位数) | 近端 | 两期 Byars 皮瓣 | 40 (49%) | 5 (6%) | 6 (7%) | — | 5 (6%) | 30 (37%) | 3 (4%) | - |
| Jayanthi, 201737 | 34 | 15.2 | 近端 | 改良 Ulaanbaatar | 5 (14.7%) | 0 | 0 | 0 | 4 (12%) | 0 | — | 复发性附睾炎 1(2.7%) |
在费城儿童医院(CHOP)于1996–2006年间进行的一项研究中,比较了连续665名接受尿道下裂修复术男童的结果,发现所有尿道下裂的并发症发生率为17%。51 在这665例中,86例(13%)为近端尿道下裂,其定义为在手术室行阴茎去套剥离后,尿道口位于阴茎中段的近端。他们观察到不成比例地多的并发症(35%)发生在近端尿道下裂男童中,且近端尿道下裂的并发症发生率为39/86(45%)。51 这与总体17%的并发症发生率形成鲜明对比。51
大多数近端型尿道下裂修复患儿需要更长、更密切的随访,以便对并发症进行详尽且如实的报告。尿道下裂致残患儿可界定为初次修复失败后,常常需要多次、复杂手术以纠正其后遗症的男孩。52 由于重建尿道管段较长,狭窄风险更高;或者由于重建尿道在排尿时未能随之扩张,显著增加尿流阻力,最终导致瘘和/或尿道憩室形成,正如 Braga et al. 所强调的。53 因此,以往对近端型尿道下裂并发症的报告存在低报。
为改善近端尿道下裂修复的疗效,Long 和 Canning51 指出可以使用一种标准化系统,系统地量化尿道下裂表型的严重程度,以创建一种通用的尿道下裂语言,从而促进跨机构协作。当前所使用的评分系统包括 HOSE、HOPE 和 GMS13,54,其中涵盖多种因素,如龟头宽度、阴茎弯曲程度以及尿道板的质量,用于针对特定患者计算相应的评分。这在一定程度上简化了结局分析中的比较,但仍受一些与患者相关因素及观察者/术者间差异的限制。
他们还强调,在外科干预后将患者及家庭的评估与外科医生的分析加以汇总的重要性51,因为二者未必总是吻合。阴茎感知评分考虑到了这一局限性。55 Weber 等人55在其研究中评估了77名(6–17岁)接受过尿道下裂修复术的男孩,就其对阴茎在尿道口、龟头、皮肤及整体外观方面的自我感知进行评价。他们发现,在男孩、家长和泌尿科医生中,这些条目“尿道口”“龟头”“皮肤”与“整体外观”之间的相互相关性良好。尿道下裂患者对阴茎外观的满意度较高,且与年龄匹配的对照相比无显著差异。然而有趣的是,家长和泌尿科医生对阴茎外观的满意度低于患者本人。55 这凸显了除手术医生之外,由患者及其家长进行自我评估的重要性。
Long et al 提出的另一种方法是通过指导与团队合作51,利用诸如会议、学术会议、工作坊、在封闭小组中对录制视频进行批判性分析、反馈与讨论等各种机会。这无疑将增加接触机会,并推进对近端尿道下裂这一复杂且罕见疾病的认识。
参考文献
- Baskin LS. Chapter 121 - Hypospadias. In: Coran AG, In, editors. Pediatric Surgery (Seventh Edition). Mosby; 2012. DOI: 10.1016/b978-0-323-07255-7.00121-5.
- Samuel M, Capps S, Worth A. Proximal Hypospadias. Eur Urol 2011; 40 (4): 463–468. DOI: 10.1159/000049817.
- Baskin L, Erol A, Jegatheesan P, Li Y, Liu W, Cunha G. Urethral seam formation and hypospadias. Cell Tissue Res 2001; 305 (3): 379–387. DOI: 10.1007/s004410000345.
- Baskin L, Shen J, Sinclair A, Cao M, Liu X, Liu G, et al.. Development of the human penis and clitoris. Differentiation 2018; 103: 74–85. DOI: 10.1016/j.diff.2018.08.001.
- Smith DR, Tanagho EA, McAninch JW. Smith’s General Urology. Norwalk, Conn: Appleton & Lange; Chap; 1992.
- Wein AJ, Kavoussi LR, Campbell MF. 1. 2012.
- Gerasaro TS, Brock WA, Kaplan GW. Upper Urinary Tract Anomalies Associated With Congenital Hypospadias: Is Screening Necessary? J Urol 1986; 135 (3): 537–538. DOI: 10.1016/s0022-5347(17)45729-6.
- Rajfer J, Walsh PC. The Incidence of Intersexuality in Patients with Hypospadias and Cryptorchidism. J Urol 1976; 116 (6): 769–770. DOI: 10.1016/s0022-5347(17)59004-7.
- Kaefer M, Diamond D, Hendren WH, Vemulapalli S, Bauer SB, Peters CA, et al.. The Incidence Of Intersexuality In Children With Cryptorchidism And Hypospadias: Stratification Based On Gonadal Palpability And Meatal Position. J Urol 1999; 162 (3 Part 2): 1006–1007. DOI: 10.1016/s0022-5347(01)68049-2.
- Ahmed SF, Achermann JC, Arlt W, Balen A, Conway G, Edwards Z. Society for Endocrinology UK guidance on the initial evaluation of an infant or an adolescent with a suspected disorder of sex development. 2015; 4 (5): 71–88. DOI: 10.1111/j.1365-2265.2011.04076.x.
- Hadidi AT, Azmy AF. Hypospadias surgery: an illustrated guide. 2004. DOI: 10.1111/j.1440-1754.2005.571_3.x.
- Shoor G, Acharya SK. Bedside clinics and Round questions in Pediatric Surgery. 2022.
- Arlen AM, Kirsch AJ, Leong T, Broecker BH, Smith EA, J.M.. Faculty Opinions recommendation of Further analysis of the Glans-Urethral Meatus-Shaft (GMS) hypospadias score: correlation with postoperative complications. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 11. DOI: 10.3410/f.725403208.793522967.
- Abbott JE, Heinemann A, Badalament R, Davalos JG. A clever technique for placement of a urinary catheter over a wire. Urol Ann 2015; 7 (3): 367. DOI: 10.4103/0974-7796.157959.
- Hughes IA, Houk C, Ahmed SF, Lee PA, Group LWPESC, Group ESPEC. Consensus Statement on Management of Intersex Disorders. Pediatric Clinical Practice Guidelines &Amp; Policies 2006; 91 (7): 1317–1317. DOI: 10.1542/9781610021494-part06-consensus_statement2.
- Urology S on. Timing of Elective Surgery on the Genitalia of Male Children With Particular Reference to the Risks, Benefits, and Psychological Effects of Surgery and Anesthesia. Pediatrics 1996; 97 (4): 590–594. DOI: 10.1542/peds.97.4.590.
- Bermudez DM, Canning DA, Liechty KW. Age and pro-inflammatory cytokine production: Wound-healing implications for scar-formation and the timing of genital surgery in boys. J Pediatr Urol 2011; 7 (3): 324–331. DOI: 10.1016/j.jpurol.2011.02.013.
- Belman AB, Kass EJ. Hypospadias Repair in Children Less than 1 Year Old. J Urol 1982; 128 (6): 1273–1274. DOI: 10.1016/s0022-5347(17)53458-8.
- Hadidi AT. History of hypospadias: Lost in translation. J Pediatr Surg 2017; 52 (2): 211–217. DOI: 10.1016/j.jpedsurg.2016.11.004.
- Snodgrass W, Prieto J. Straightening Ventral Curvature While Preserving the Urethral Plate in Proximal Hypospadias Repair. J Urol 2009; 182 (4s): 1720–1725. DOI: 10.1016/j.juro.2009.02.084.
- Moscardi PRM, Gosalbez R, Castellan MA. Management of High-Grade Penile Curvature Associated With Hypospadias in Children. Front Pediatr 2017; 5 (189). DOI: 10.3389/fped.2017.00189.
- Braga LHP, Pippi Salle JL, Dave S, Bagli DJ, Lorenzo AJ, Khoury AE. Outcome Analysis of Severe Chordee Correction Using Tunica Vaginalis as a Flap in Boys With Proximal Hypospadias. J Urol 2007; 178 (4s): 1693–1697. DOI: 10.1016/j.juro.2007.03.166.
- Gittes RF, McLaughlin AP. Injection technique to induce penile erection. Urology 1974; 4 (4): 473–474. DOI: 10.1016/0090-4295(74)90025-9.
- Castellan M, Gosalbez R, Devendra J, Bar-Yosef Y, Labbie A. Ventral corporal body grafting for correcting severe penile curvature associated with single or two-stage hypospadias repair. J Pediatr Urol. 2011;7:289-93. . DOI: 10.1016/j.jpurol.2012.02.009.
- Snodgrass W, Bush N. Staged Tubularized Autograft Repair for Primary Proximal Hypospadias with 30-Degree or Greater Ventral Curvature. J Urol 2017; 198 (3): 680–686. DOI: 10.1016/j.juro.2017.04.019.
- Nesbit RM. Operation for Correction of Distal Penile Ventral Curvature with or Without Hypospadias. J Urol 1966; 97 (4): 720–722. DOI: 10.1016/s0022-5347(17)63105-7.
- Duckett JW. Transverse Preputial Island Flap Technique for Repair of Severe Hypospadias. Urol Clin North Am 1980; 7 (2): 423–430. DOI: 10.1016/s0094-0143(21)01243-x.
- Ascopa HS, Elhence IP, Atri SP, Bansal NK. One stage correction of penile hypospadias using a foreskin tube. Plast Reconstr Surg 1971; 49 (1): 104–105. DOI: 10.1097/00006534-197201000-00044.
- Hypospadias Surgery: Science and Art - V.V.S. . DOI: 10.4103/jiaps.jiaps_202_20.
- Snodgrass WT, Lorenzo A. Tubularized incised-plate urethroplasty for proximal hypospadias. BJU Int 2002; 89 (1): 90–93. DOI: 10.1046/j.1464-410x.2002.02524.x.
- Snodgrass WT, Granberg C, Bush NC. Faculty Opinions recommendation of Urethral strictures following urethral plate and proximal urethral elevation during proximal TIP hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2013; 9 (6 Pt B): 990–994. DOI: 10.3410/f.718013467.793494058.
- Singh AP, Shukla AK, Sharma P, Shukla J. Two stages repair of proximal hypospadias: Review of 700 cases. J Indian Assoc Pediatr Surg 2017; 22 (3): 158. DOI: 10.4103/0971-9261.207627.
- Bracka A. Hypospadias repair: the two-stage alternative. Br J Urol 1995; 76 (6): 31–41. DOI: 10.1111/j.1464-410x.1995.tb07815.x.
- Bracka A. Buccal Mucosa: Good But Not Perfect. J Urol 2011; 185 (3): 777–778. DOI: 10.1016/j.juro.2010.12.015.
- FERRO F, ZACCARA A, SPAGNOLI A, LUCCHETTI MC, CAPITANUCCI ML, VILLA M. Skin Graft for 2-stage Treatment of Severe Hypospadias: Back to the Future? J Urol 2002; 168 (4 Pt 2): 1730–1733. DOI: 10.1097/00005392-200210020-00018.
- Johal NS, Nitkunan T, O’Malley K, Cuckow PM. The Two-Stage Repair for Severe Primary Hypospadias. Eur Urol 2006; 50 (2): 366–371. DOI: 10.1016/j.eururo.2006.01.002.
- Dessanti A, Rigamonti W, Merulla V, Falchetti D, Caccia G. Autologous Buccal Mucosa Graft for Hypospadias Repair: An Initial Report. J Urol 1992; 147 (4): 1081–1083. DOI: 10.1016/s0022-5347(17)37478-5.
- Hadidi AT. Perineal Hypospadias: The Bilateral-Based (BILAB) Skin Flap Technique. Hypospadias Surgery 2014; 49 (1): 497–506. DOI: 10.1007/978-3-030-94248-9_32.
- Lanciotti M, Betti M, Elia A, Landi L, Taverna M, Cini C, et al.. Proximal hypospadias repair with bladder mucosal graft: Our 10 years experience. J Pediatr Urol 2017; 13 (3): 294.e1–294.e6. DOI: 10.1016/j.jpurol.2017.01.011.
- Pal DK, Gupta DK, Ghosh B, Bera MK. A comparative study of lingual mucosal graft urethroplasty with buccal mucosal graft urethroplasty in urethral stricture disease: An institutional experience. Urol Ann 2016; 8 (2): 157. DOI: 10.4103/0974-7796.172214.
- Pippi Salle JL, Sayed S, Salle A, Bagli D, Farhat W, Koyle M, et al.. Proximal hypospadias: A persistent challenge. Single institution outcome analysis of three surgical techniques over a 10-year period. J Pediatr Urol 2016; 12 (1): 28.e1–28.e7. DOI: 10.1016/j.jpurol.2015.06.011.
- Faure A, Heloury Y. Response to “Re: Faure A, Bouty A, Nyo L, O’Brian M, Heloury Y. Two-stage graft urethroplasty for proximal and complicated hypospadias in children: a retrospective study.” J Pediatr Urol 2016; 12 (5): 286 1–286 7. DOI: 10.1016/j.jpurol.2016.12.007.
- Sakr A, Elkady E, Abdalla M, Fawzi A, Kamel M, Desoky E, et al.. Lingual mucosal graft two-stage Bracka technique for redo hypospadias repair. Arab J Urol 2017; 15 (3): 236–241. DOI: 10.1016/j.aju.2017.06.002.
- Greenfield SP, Sadler BT, Wan J. The Two-Stage Repair for Severe Primary Hypospadias. Yearbook of Urology 1994; 2007 (2 Pt 1): 250. DOI: 10.1016/s0084-4071(08)70198-2.
- Retik AB, Bauer SB, Mandell J, Peters CA, Colodny A, Atala A. Management of Severe Hypospadias with a 2-Stage Repair. J Urol 1994; 152 (2 Part 2): 749–751. DOI: 10.1016/s0022-5347(17)32697-6.
- CHENG EARLY, KROPP BRADLEYP, POPE JOHNC, BROCK JOHNW. Proximal Division of the Urethral Plate in Staged Hypospadias Repair. J Urol 2003; 170 (4 Part 2): 1580–1584. DOI: 10.1097/01.ju.0000084258.93064.f4.
- Canning D. Faculty Opinions recommendation of Management of Proximal Hypospadias with 2-Stage Repair: 20-Year Experience. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (4): 1080–1085. DOI: 10.3410/f.725486894.793522961.
- Canning D. Faculty Opinions recommendation of Complications following Staged Hypospadias Repair Using Transposed Preputial Skin Flaps. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (2): 512–516. DOI: 10.3410/f.725364224.793522958.
- Tiryaki S, Əl\Elzschwakb\Elzschwarova VE, Dokumcu Z, Ergun R, Tekin A, Yagmur I, et al.. Unexpected outcome of a modification of Bracka repair for proximal hypospadias: High incidence of diverticula with flaps. J Pediatr Urol 2016; 12 (6): 395.e1–395.e6. DOI: 10.1016/j.jpurol.2016.04.046.
- Lin H, Wang Y-Y, Li S-B, Chen Z-T, Su L-J. Staged transverse preputial island flap urethroplasty for some proximal hypospadias with moderate-to-severe chordee. BMC Urol 2016; 21 (1): 1536–1540. DOI: 10.1186/s12894-021-00948-8.
- Hanna M. Faculty Opinions recommendation of Hypospadias: Are we as good as we think when we correct proximal hypospadias? Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2016: 1477513116300432–. DOI: 10.3410/f.726422269.793519822.
- Barbagli G, Sansalone S, Djinovic R, Lazzeri M. Surgical Repair of Late Complications in Patients Having Undergone Primary Hypospadias Repair during Childhood: A New Perspective. Adv Urol 2012; 2012 (705212): 1–5. DOI: 10.1155/2012/705212.
- Braga LH, Pippi Salle JL, Lorenzo AJ. Comparative Analysis of Tubularized Incised Plate Versus Onlay Island Flap Urethroplasty for Penoscrotal Hypospadias. Yearbook of Urology 2007; 2008 (1451-6): 246–247. DOI: 10.1016/s0084-4071(08)79119-x.
- Holland AJA, Smith GHH, Ross FI, Cass DT. HOSE: an objective scoring system for evaluating the results of hypospadias surgery. BJU Int 2001; 88 (3): 255–258. DOI: 10.1046/j.1464-410x.2001.02280.x.
- Merriman LS, Arlen AM, Broecker BH, Smith EA, Kirsch AJ, Elmore JM. The GMS hypospadias score: Assessment of inter-observer reliability and correlation with post-operative complications. J Pediatr Urol 2013; 9 (6): 707–712. DOI: 10.1016/j.jpurol.2013.04.006.
- F T, TP J, RP G. RE: Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A validation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients. J Pediatr Urol 2013; 9 (6): 1016. DOI: 10.1016/j.jpurol.2013.07.022.
- Weber DM, Schonbucher VB, Landolt MA, Gobet R. Faculty Opinions recommendation of The Pediatric Penile Perception Score: an instrument for patient self-assessment and surgeon evaluation after hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2008; 180 (1080-4): 1084. DOI: 10.3410/f.719560881.793500484.
最近更新时间: 2025-09-22 08:00