
32: Hipospadias proximal
Este capítulo durará aproximadamente 29 minutos para leer.
Introducción
La hipospadias se define como una abertura del meato uretral en la cara ventral del cuerpo del pene, proximal a la punta del glande. Como se mencionó en el capítulo anterior, la hipospadias se clasifica según la localización del meato uretral como distal, media y proximal. La variedad posterior (grave), que representa el 20% de los casos, se extiende a través del tercio proximal del cuerpo del pene hasta el periné. Puede subclasificarse además como peneana posterior (en la base del cuerpo), penoescrotal (en la base del cuerpo delante del escroto), escrotal (en el escroto o entre las prominencias genitales) o, la variedad más grave, la perineal (detrás del escroto y detrás de las prominencias genitales, Figura 1).1 Aunque la clasificación de la hipospadias en distal, porción media del cuerpo y proximal se ha basado históricamente en la localización del meato en el preoperatorio, la clasificación correcta se realiza mejor en el momento de la cirugía, ya que la localización del meato puede cambiar en función de una uretra hipoplásica más proximal. La hipospadias grave suele asociarse con curvatura ventral del pene conocida como chordee, un prepucio “en capucha” o incompleto, y un cuerpo esponjoso abortivo. La hipospadiología, término acuñado por John W. Duckett, Jr., es el estudio de todos los aspectos de esta afección y abarca una disciplina en continua evolución y expansión.2 La incidencia de la hipospadias es de aproximadamente 1:200–300 nacidos vivos en los EE. UU.3,4 El reciente aumento de la incidencia puede atribuirse a la prematuridad, a los recién nacidos pequeños para la edad gestacional, al bajo peso al nacer y a la edad materna de 35 años o más.1
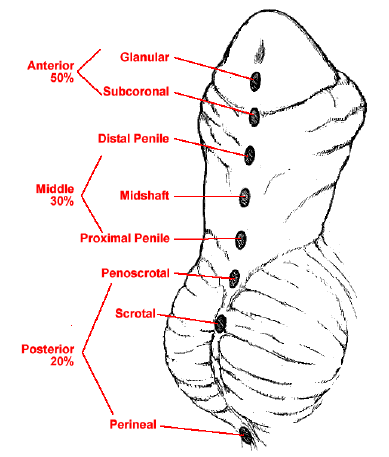
Figura 1 Espectro de las formas de presentación del hipospadias.
Embriología
Los genitales externos masculinos desarrollan progresivamente características reconocibles hacia el 3er mes de gestación. Normalmente, el orificio del seno urogenital se extiende hacia la cara ventral del tubérculo genital como el surco uretral. El orificio urogenital primitivo y el surco uretral están delimitados a ambos lados por los pliegues uretrales.5 El tubérculo genital se alarga para formar el falo, y los pliegues uretrales comienzan a fusionarse desde el orificio urogenital hacia la punta del falo, lo que da lugar a la formación de la uretra peneana al final de la 14.ª semana. Los cuerpos cavernosos aparecen como columnas mesenquimatosas pares dentro del eje del pene en la 7.ª semana. El cuerpo esponjoso resulta de la diferenciación de las masas mesenquimatosas alrededor de la uretra peneana.5 En los casos de hipospadias proximal, se considera que existe una falta de fusión de estos pliegues uretrales. Debido a la detención de la tubularización, se produce un crecimiento diferencial del pene en la cara ventral en comparación con la cara dorsal.
Una comprensión de la anatomía del pene ayudará en gran medida a comprender la reparación del hipospadias (Figura 2).
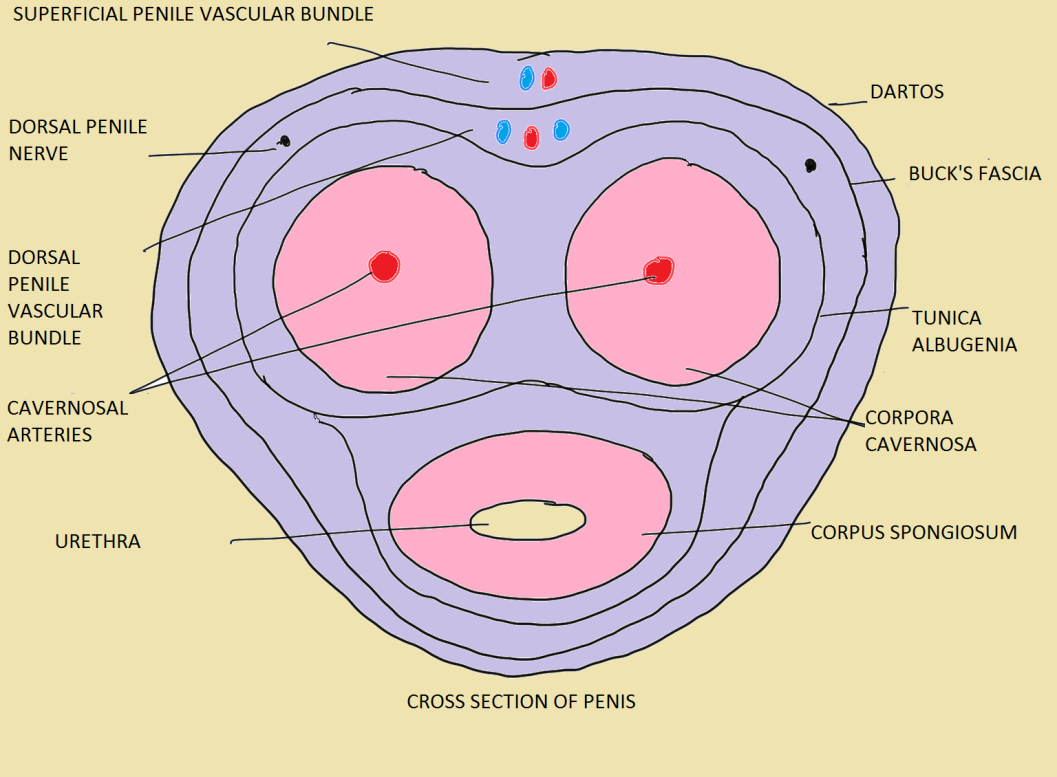 Figura 2 Las capas del pene en un adulto normal.6
Figura 2 Las capas del pene en un adulto normal.6
Hipospadias grave y otras afecciones genitourinarias asociadas
Debido a una embriopatía común, el hipospadias proximal se asocia con mayor frecuencia a otras afecciones congénitas, a saber, criptorquidia en el 10% de los casos,7 hernia inguinal en hasta el 32% de los varones,8 trastornos del desarrollo sexual en hasta el 27,3%9 y utrículo prostático.
En presencia de hipospadias grave y de un testículo no palpable, se debe descartar un trastorno del desarrollo sexual.10 En estos casos, es imprescindible obtener un cariotipo. La hipospadias escrotal por sí sola debe hacer sospechar un trastorno del desarrollo sexual, más aún cuando se asocia a criptorquidia bilateral.11 Se sospechan genitales ambiguos en pacientes con hipospadias y gónadas impalpables; hipospadias con micropene y una o ninguna gónada palpable; recién nacidos con genitales externos femeninos y una masa gonadal en los labios o fusión labial y/o aumento del clítoris.12
Evaluación
Tabla 1 Puntos a tener en cuenta al evaluar un caso de hipospadias.6
| Historia | Historia adicional | Examen | Examen adicional |
|---|---|---|---|
| edad, criado como varón | antecedentes de cambio de voz, desarrollo mamario | longitud fálica en estiramiento | hábitus (masculino o femenino) |
| antecedentes de micción por la cara inferior del pene | antecedentes de ingesta materna de hormonas durante el embarazo | curvatura peneana (chordee) (ausente/leve <30˚/severa >30˚) | desarrollo mamario (estadios de Tanner) |
| curvatura ventral del pene | antecedentes familiares de hipospadias | meato (estenosado/ no estenosado) | vello axilar (presente o ausente, desarrollo de tipo masculino o femenino) |
| chorro urinario desviado de la línea media o estrecho | antecedentes de pérdidas fetales repetidas o enfermedad aguda y vómitos en el período neonatal | ubicación del meato (glandular/coronal/peniana distal/peniana media/peniana proximal/penoescrotal/escrotal) | vello púbico (presente o ausente, desarrollo de tipo masculino o femenino) |
| antecedentes de cirugía genital | glande (redondeado/cónico) | ambigüedad de los genitales externos (estadios de Prader en un caso de DSD) | |
| testículo no descendido | surco uretral (superficial/profundo) | ||
| antecedentes de erecciones y curvatura en un adolescente mayor | placa uretral (ancha/estrecha/cicatrizada/elástica) | ||
| prepucio (capucha dorsal/adecuado para reconstrucción/ausente) | |||
| localización de los testículos | |||
| tamaño de los testículos | |||
| escroto (bien desarrollado/transposición penoescrotal/hipoplásico/repliegue penoescrotal) |
Además, la puntuación GMS (glande, meato y tronco peneano) parece correlacionarse con el riesgo de complicaciones quirúrgicas. La puntuación GMS se basa en el tamaño del glande/calidad de la placa uretral, la ubicación del meato y el grado de curvatura. Arlen et al demostraron un aumento estadísticamente significativo en la probabilidad de cualquier complicación posoperatoria por cada unidad de incremento en la puntuación GMS total Tabla 2.13 En su estudio, 262 niños (edad media 12.3 ± 13.7 meses) sometidos a reparación primaria de hipospadias presentaron una puntuación GMS media de 7 ± 2.5 (G 2.1 ± 0.9, M 2.4 ± 1, S 2.4 ± 1) y un seguimiento clínico medio de 17.7 ± 9.3 meses. Encontraron que 37 niños desarrollaron 45 complicaciones. Se observó una relación significativa entre la puntuación GMS total y la presencia de cualquier complicación (p < 0.001); por cada unidad de aumento en la puntuación GMS, las probabilidades de cualquier complicación posoperatoria aumentaron 1.44 veces (IC del 95%, 1.24–1.68).13 El desarrollo de una fístula uretrocutánea se observó en 21 de 239 (8.8%) reparaciones en un solo tiempo y fue la complicación más frecuente. Aquellos con hipospadias leve (GMS 3–6), moderado (GMS 7–9) y grave (GMS 10–12) tuvieron tasas de fístula de 2.4%, 11.1% y 22.6% (p < 0.001), respectivamente. Asimismo, el grado de curvatura se observó como un predictor independiente de fístula en el análisis multivariante. Encontraron que los pacientes con curvatura ventral mayor de 60° tenían 27 veces más probabilidades de desarrollar una fístula que los pacientes sin curvatura (IC del 95%, 3.2–229).13
Tabla 2 La puntuación GMS.13
| Puntuación del glande (G) | Puntuación del meato (M) | Puntuación del eje (S) |
|---|---|---|
| 1. Glande de buen tamaño; placa uretral sana, profundamente acanalada | 1. Glandular | 1. Sin curvatura |
| 2. Glande de tamaño adecuado; placa uretral adecuada, acanalada | 2. Surco coronal | 2. Curvatura leve (< 30°) |
| 3. Glande de tamaño pequeño; placa uretral estrecha, con cierta fibrosis o plana | 3. Eje medio o distal | 3. Curvatura moderada (30–60°) |
| 4. Glande muy pequeño; placa uretral indistinta, muy estrecha o plana | 4. Eje proximal, penoescrotal | 4. Curvatura grave (> 60°) |
La evaluación de la placa uretral también es importante, ya que una placa uretral estrecha augura un peor pronóstico (Figura 3). Los dos factores predominantes que guían nuestra decisión sobre cómo reparar un hipospadias proximal son la calidad de la placa uretral y, quizá más importante, el grado de curvatura ventral presente
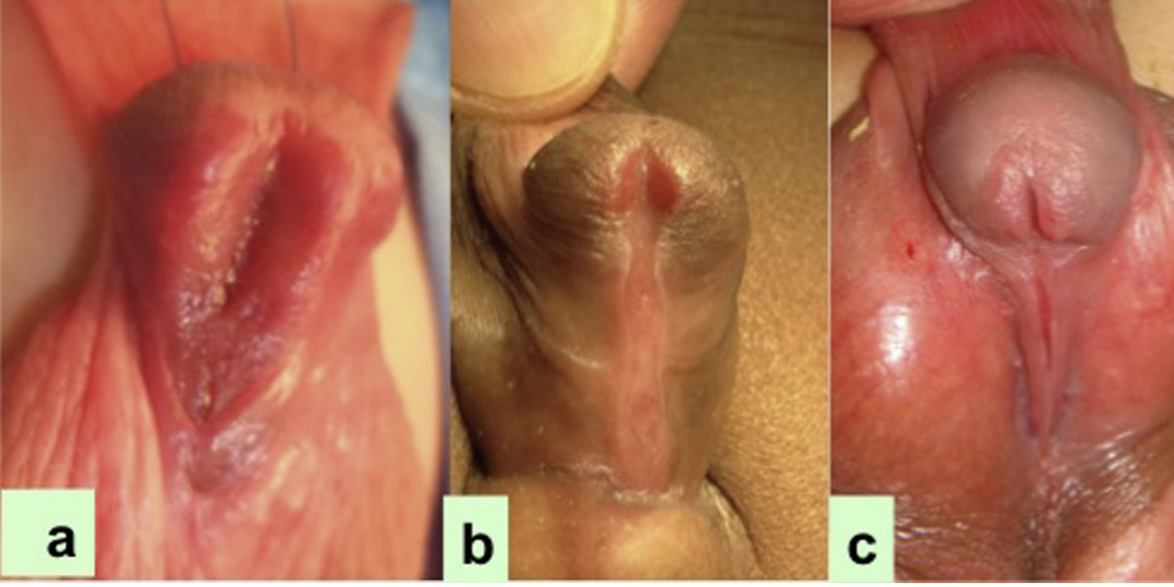
Figura 3 El ancho de la placa uretral disminuye de a a c en los pacientes con hipospadias proximal.14
Investigaciones
Imágenes
- La ecografía debe realizarse en casos de hipospadias proximal para descartar anomalías renales asociadas, aunque tales anomalías son extremadamente raras.12 Si existe antecedente de infección del tracto urinario recurrente, debe realizarse una cistouretrografía miccional. Asimismo, en casos de ambigüedad genital verdadera, la MCU puede ayudar a evaluar la presencia de remanentes müllerianos. Estos pacientes suelen ser asintomáticos y no requieren resección quirúrgica rutinaria de los remanentes. Ocasionalmente, puede ser necesaria la resección del utrículo debido a infección del tracto urinario recurrente, goteo urinario o formación de cálculos.12 Durante la cirugía en pacientes con hipospadias proximal, el utrículo prostático a veces puede impedir la colocación del catéter en la vejiga, alojándose el catéter preferentemente en el propio utrículo. Esto puede solucionarse mediante cualquiera de los siguientes métodos i) el método del doble catéter, en el que el primer catéter entra inadvertidamente en el utrículo prostático, luego se inserta por el meato uretral un catéter French de menor calibre y éste entra invariablemente en la uretra; ii) la sonda de Clutton para guiar el catéter uretral; iii) en casos difíciles, puede pasarse primero a la vejiga una guía blanda asistida por cistoscopia y, a continuación, avanzar sobre la guía un catéter de extremo abierto hasta la vejiga.15
Cariotipado
La guía de la AUA sobre criptorquidia recomienda que todos los niños con testículos no descendidos unilaterales o bilaterales y hipospadias proximal grave deben someterse a pruebas adicionales para descartar un trastorno de la diferenciación sexual (DSD), que ocurre con mucha mayor frecuencia en estos contextos .9,10 Las guías introducidas en 2006 incluyeron el hipospadias grave como una forma de DSD 46,XY.16 La preocupación por DSD es particularmente alta en un niño con hipospadias y un testículo no palpable. Kaefer et al.10 examinaron a 79 pacientes con antecedente de hipospadias y criptorquidia. Aquellos con testículo(s) no palpable(s), ya fuera unilateral o bilateral, presentaron un riesgo tres veces mayor de que se identificara un diagnóstico subyacente de DSD (aproximadamente 50% vs. 15%). Hubo un riesgo significativamente mayor de DSD con hipospadias proximal en comparación con hipospadias distal (64% vs. 7%) .10 Un cariotipo 46, XY normal puede ser engañoso, particularmente en niños con las variantes más graves. Los autores también prefieren investigar a estos pacientes con hipospadias grave y UDT mediante cariotipado.
Andrógeno preoperatorio
El uso preoperatorio de DHT o de testosterona puede ser mediante aplicación local o, con mayor frecuencia, por inyección intramuscular; puede conducir a un aumento de la longitud y el grosor del pene y puede causar un aumento del tamaño del glande. En pacientes con micropene, la testosterona ha demostrado ser beneficiosa para estimular el crecimiento del pene. El protocolo de aplicación puede variar en diferentes instituciones. Se recomienda la aplicación local de crema de propionato de testosterona al 2% en el pene tres veces al día durante 3 semanas.12 Esta vía de administración de testosterona es fácil de aplicar y muestra buena respuesta. Sin embargo, la respuesta es variable dependiendo del cumplimiento de la aplicación diaria y de la cantidad de crema aplicada. Un exceso puede provocar absorción sistémica, profundización de la voz y cambios en el comportamiento de los niños en casos extremos. La aplicación debe suspenderse al menos 3 semanas antes de la fecha de la cirugía. La testosterona intramuscular, 2 mg/kg/dosis, un total de tres dosis a intervalos de 3 semanas, administrándose la última dosis al menos 2 semanas antes de la fecha de la cirugía, es una vía de administración más fiable.
Consentimiento para la cirugía
Debe obtenerse un consentimiento informado por escrito tras proporcionar información adecuada, suficiente y oportuna sobre el procedimiento planificado y los posibles procedimientos alternativos que mejor se apliquen al caso individual. En muchas ocasiones, el procedimiento puede cambiar en función de la exploración bajo anestesia y, por lo tanto, debe informarse de antemano a los padres sobre la posibilidad de diversas opciones quirúrgicas. Debe proporcionarse una explicación clara del resultado, los resultados estéticos y las posibles complicaciones (formación de fístulas, estenosis o dehiscencia). En los casos de hipospadias proximal, los padres deben comprender que su hijo muy probablemente requerirá una reparación en múltiples tiempos. Por lo tanto, es necesaria la preparación de la familia y del paciente para el procedimiento adecuado, una evaluación anatómica precisa y una conversación honesta sobre los resultados quirúrgicos y las posibles complicaciones.7
Momento de la cirugía
El momento de la reparación primaria electiva se recomienda que ocurra entre los 6 y 12 meses de edad por la Academia Estadounidense de Pediatría [AAP]7,17 con base en estudios que destacan el equilibrio entre los posibles efectos psicológicos adversos de la cirugía, el riesgo anestésico para el niño, el grado de desarrollo peneano que facilitará una reparación exitosa y las diferencias en la cicatrización de las heridas a medida que los niños varones crecen.18 Belman et al demostraron que los niños sometidos a reparación antes de los 12 meses de edad presentaron menos ansiedad y tuvieron mejores resultados psicosexuales en comparación con los niños sometidos a reparación a edades mayores.19
Objetivos de la reconstrucción
- Permitir la micción con velocidad normal y flujo laminar,
- Obtener una función sexual satisfactoria con un pene recto, y
- Logro de un meato en forma de hendidura con un glande bien coaptado, desde el punto de vista estético.20
Etapas de la reconstrucción
- Corrección de curvatura ventral
- Uretroplastia
- Glanuloplastia
- Cobertura cutánea
Técnicas de reparación quirúrgica
En el hipospadias proximal, estos se logran con mayor frecuencia mediante una reparación por etapas. Existen dos escuelas de pensamiento en cuanto a la reparación del hipospadias proximal:
- uso de colgajos
- procedimientos de injerto por etapas
Estas dependen de la corrección de la curvatura ventral. En raras ocasiones, tras el despegamiento cutáneo no hay más curvatura ventral, y se utiliza para la uretroplastia ya sea la reparación de placa incisa tubularizada (TIP) o un colgajo en isla tipo Onlay, aunque la reparación TIP larga es menos preferida debido a complicaciones a largo plazo. Si queda curvatura residual, algunos cirujanos prefieren la reparación por etapas en la que, tras dividir la placa uretral, colocan un injerto prepucial y, si no está disponible, un injerto de mucosa bucal (BMG) en la primera etapa y luego tubulizan el injerto en la segunda etapa. Si tras el despegamiento cutáneo persiste una curvatura ventral superior a 30 grados, entonces la corrección de la curvatura, ya sea mediante colgajo de túnica vaginal (TVF), o injerto de túnica vaginal (TVG), o SIS, o dérmico, o mediante corporotomías transversas múltiples como explicó Snodgrass21 se utiliza en la primera etapa. Luego, la uretroplastia se realiza en la segunda o tercera etapa de la reparación, según la técnica para corregir la curvatura ventral.
En resumen, si, tras el despegamiento cutáneo, hay curvatura < 30, entonces hay 2 opciones: reparación TIP (no preferida por la mayoría de los cirujanos), y el colgajo únicamente dorsal.
Si la curvatura es > 30˚, entonces se divide la placa uretral (UP). Ahora, si después de la división no hay curvatura, podemos usar un colgajo prepucial dorsal como inlay o como tabularizado (según Duckett) o podemos usar injerto prepucial o BMG.
Corrección de la curvatura ventral del pene
Descripción general de la curvatura del pene
La corrección de la cordea es el paso inicial más importante en la reparación del hipospadias proximal, ya sea por etapas o en un solo tiempo. En la primera etapa, tras el despegamiento circunferencial de la piel del pene, se evalúa el grado de curvatura peneana mediante la prueba de erección artificial. Si la cordea es superior a 30 grados, medidos con regla o goniómetro (Figura 4), el siguiente paso sería dividir la placa uretral, lo cual se realiza en la mayoría de los casos en el extremo distal, cerca del nivel del glande. En esta etapa se corrige la curvatura ventral, se repara la transposición penoescrotal, se realiza el despegamiento de la piel del cuerpo del pene y se divide la placa uretral para corregir la curvatura.
Moscardi et al.22 señalaron que un alto porcentaje de curvaturas peneanas se resolvieron únicamente mediante el desenfundamiento del pene, de la piel ventral acortada y del dartos ventral fibrótico. Braga et al.23 revisaron la tasa de resolución de la curvatura peneana tras la disección de la piel y de la fascia de dartos en 137 pacientes con hipospadias7 en los que 9 tenían leve (<30°), 44 moderada (30–45°) y 85 tenían curvatura severa (>45°). La tasa de resolución completa de la curvatura, tras el desenfundamiento del pene fue del 70% en el grupo leve, del 30% en el moderado y del 2.4% en el grupo de curvatura severa.23
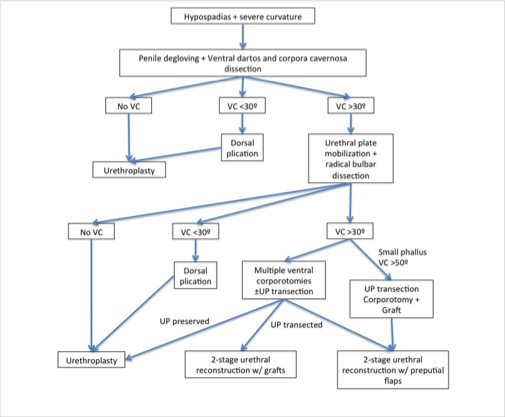
Figura 4 Manejo en pacientes con hipospadias peneano proximal y curvatura peneana.22
Medición del grado de incurvación peneana
El enderezamiento del eje peneano se mide utilizando la prueba de erección artificial, es decir, la técnica de Gittes y McLaughlin.24 En esta prueba, se inyecta solución salina a través de una aguja fina (calibre 25–27) en el aspecto lateral de los cuerpos cavernosos o en el glande, con un torniquete en la base del pene (Figura 5).
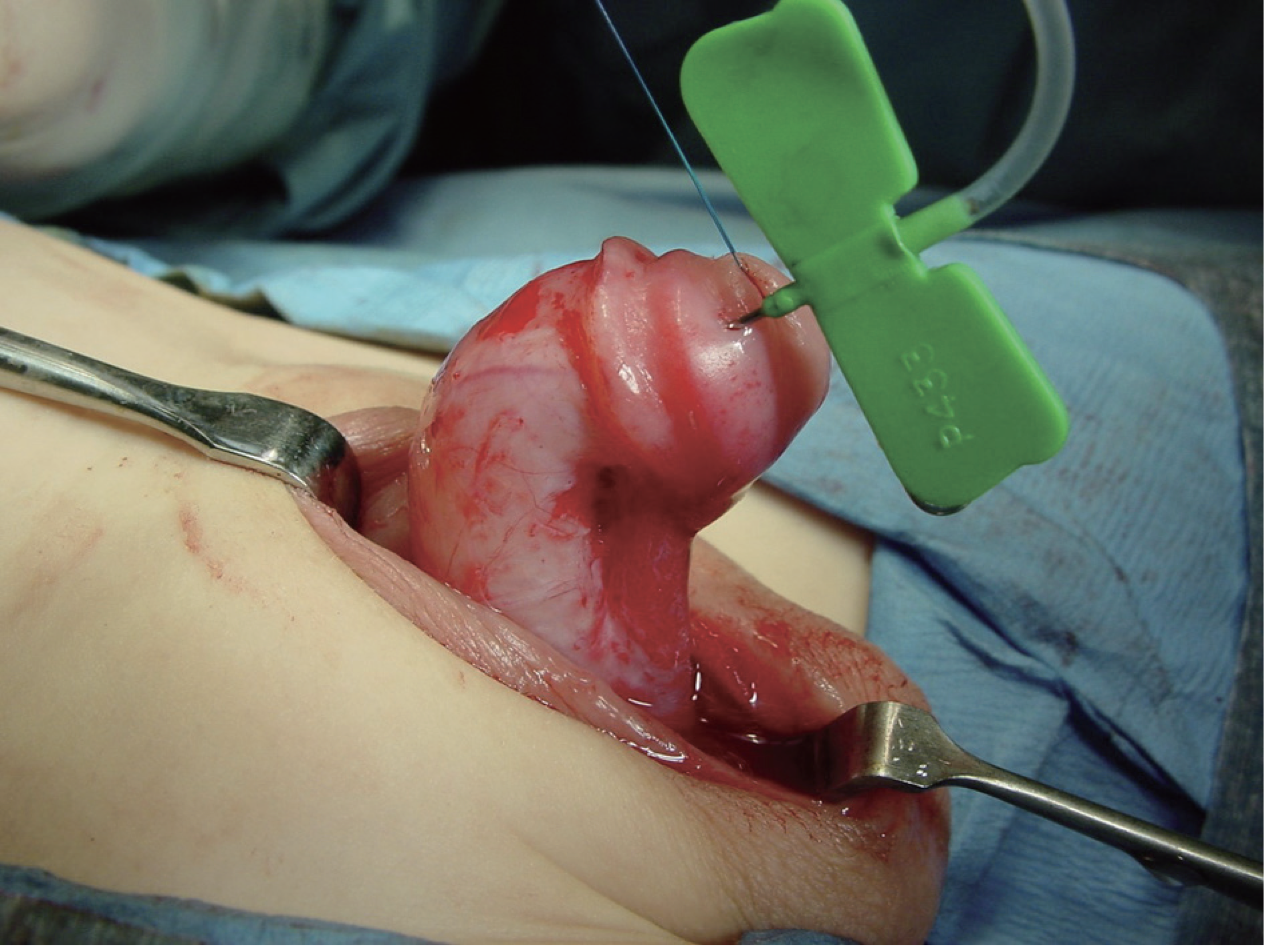
Figura 5 Medición del grado de curvatura peneana intraoperatoria.
Sin embargo, en un alto porcentaje de hipospadias proximales, tras el despegamiento, si una erección artificial muestra más de 30 grados de curvatura (chordee), entonces la UP se divide en el extremo distal, cerca del glande, y se diseca la uretra proximal para enderezar el pene, mejorar la longitud peneana y evitar la retracción por la placa uretral corta y fibrótica.22 Las técnicas de elongación peneana incluyen la realización de múltiples incisiones transversales en la cara ventral de la túnica albugínea o, realizando una única incisión transversal y aplicando un injerto o colgajo de túnica vaginal, injerto de SIS, o de dermis (Figura 6).

Figura 6 Corrección de la curvatura peneana mediante corporotomía y uso de un injerto de SIS para cubrir el área cruenta.
Curvatura peneana residual tras incisión UP
En aquellos casos en los que la curvatura aún persiste en la prueba de erección artificial, tras seccionar la UP, hay dos formas de tratar la curvatura residual: corporotomías, es decir, realizar 3 incisiones transversales ventralmente, no muy profundas, sin cobertura con ningún injerto, o la otra forma, que los autores también utilizan, es hacer una gran incisión transversal y luego cubrirla con injerto dérmico, SIS, TVG o TV FLAP (Figura 7).21
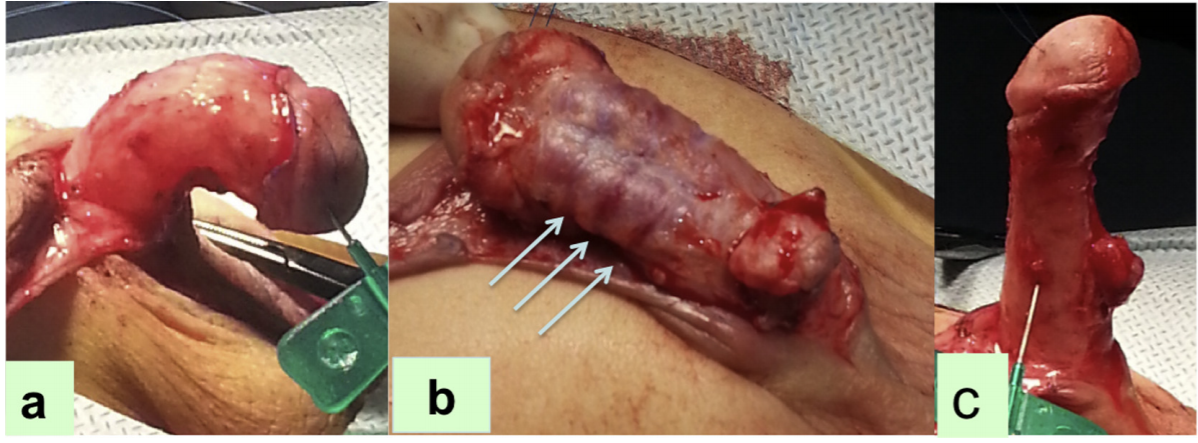
Figura 7 (a) La prueba de erección artificial que demuestra el grado de curvatura peneana, (b) Múltiples corporotomías transversas, (c) Enderezamiento de la curvatura peneana al repetir la prueba. [De: Una alternativa para el alargamiento ventral en niños con curvatura peneana severa que permite la cobertura con injerto durante la reparación por etapas de la hipospadias. Bruno Leslie, Bryce Weber, Rodrigo Romao, Walid Farhat, Darius Bagli, Armando Lorenzo, Joao Pippi Salle. J Urol Vol 221, pág. 11, 2011]
En la primera técnica, se realizan ventralmente tres corporotomías transversales, primero en el punto de máxima curvatura de las 4 a las 8 horas, y dos más 5 mm proximal y 5 mm distal a la primera, a través de la túnica albugínea hasta que el tejido eréctil sea visible, y luego se repite la prueba. Estas corporotomías pueden cubrirse utilizando la uretra proximal nativa, tras la disección proximal, o cubrirse con injerto prepucial o BMG.21,25
Snodgrass realizó un estudio en 43 niños con hipospadias proximal y curvatura ventral de 30 grados o más en quienes, tras el desenfundamiento, se efectuó la transección de la placa uretral. Aquellos pacientes con curvatura ventral persistente de 30 grados o más también fueron sometidos a 3 corporotomías ventrales sin injerto corporal para el enderezamiento. Se realizó uretroplastia por etapas con injerto utilizando prepucio o mucosa labial.21,25,26 Encontraron que la curvatura ventral media fue de 70 grados, se practicó corporotomía en el 65% de ellos y los injertos prepuciales se utilizaron en el 88%; en el resto de los pacientes, la corporotomía se cubrió con injertos dérmicos. No se informó recidiva de la curvatura ventral en ninguno de estos pacientes, aunque 10 (23%) presentaron complicaciones durante el seguimiento y 9 se sometieron a reoperaciones.26 Con ello, el concepto actual de reparación del hipospadias STraighten And Close (STAC) o Straighten and Graft (STAG) ha sido popularizado por Snodgrass y Bush (Figura 8).

Figura 8 La reparación con autoinjerto tubularizado en etapas (STAG). (A) En el momento de la primera etapa, se realizan de una a tres corporotomías ventrales a través de la túnica albugínea, con la incisión media opuesta al punto de máxima curvatura. (B) Se marca y se toma el injerto prepucial. (C) El injerto prepucial se coloca en la cara ventral del eje peneano y luego se fija con suturas de acolchado (D). El panel inferior muestra la segunda etapa de la reparación. (E) Se marcan las incisiones de la uretroplastia y se extienden a lo largo de la línea media del escroto. (F) Se desarrollan las alas del glande. (G) Se realiza una uretroplastia en dos capas y posteriormente se cubre con una capa de barrera con túnica vaginal. (H) Aspecto tras el cierre [De: Snodgrass W: Staged tubularized autograft repair for primary proximal hypospadias. J Urol 198:680–686, 2017].
Los colgajos presentan la mencionada limitación del aporte sanguíneo en los bordes, mayor probabilidad de estenosis y una tasa aumentada de formación de divertículos, ya que están menos fijados a los cuerpos cavernosos subyacentes. Estas deficiencias se superan con la técnica de injerto, en la que existe un aporte sanguíneo uniforme al injerto, que queda bien fijado a los cuerpos cavernosos subyacentes y, por tanto, con menor probabilidad de formación de estenosis y de divertículos, respectivamente. El diagrama de flujo de Moscardi et al es útil para individualizar el manejo de la curvatura peneana severa en pacientes con hipospadias proximal (Figura 4).22
Plicatura dorsal
En algunos pacientes en los que la curvatura aún persiste o solo hay una inclinación del glande, o si la incurvación es menor de 30 grados, puede realizarse una plicatura dorsal, como fue popularizada previamente por Baskin. En la actualidad, la mayoría de los cirujanos realizan el procedimiento de Nesbit o Nesbit modificado. En esta técnica, se reseca una cuña romboidal de albugínea dorsolateral en el punto de máxima curvatura y posteriormente el defecto se sutura en sentido transversal con una sutura no absorbible como proline.27 Se han descrito varias modificaciones de esta técnica, incluida la plicatura dorsal sin resección de la fascia peneana.
Reparación de hipospadias en un tiempo
Esto suele implicar una plicatura dorsal para corregir la curvatura ventral peneana en conjunto con varias técnicas diferentes de uretroplastia, dependiendo del tejido utilizado en la reparación; piel prepucial; piel local; o un injerto bucal.7 Algunas de las reparaciones de hipospadias en una sola etapa son:
Colgajo de isla prepucial transversal (tubo de Duckett);28 En este, se eleva un colgajo en isla prepucial y se tubulariza para una uretroplastia de sustitución. Esto fue modificado por Asopa,29 donde, en lugar de tubularizar el colgajo antes de fijarlo al eje peneano, el lado izquierdo del colgajo se ancla a la superficie ventral del eje peneano, justo a la izquierda de la línea media.7 Luego se utilizan suturas de Lembert interrumpidas para cerrar el colgajo en la línea media. Esto reduce el riesgo de exponer el epitelio por debajo de la reparación. Las suturas se extienden hasta la porción media del glande. Luego, el colgajo se coloca cuidadosamente sobre la línea de sutura, y las alas del glande se llevan sobre la uretroplastia y el colgajo vascular. La base del colgajo tubularizado se ancla al extremo distal de la uretra nativa (Figura 9).2,7 Se realiza una tubularización en dos capas, manteniendo un calibre uniforme en toda su longitud. En pacientes con curvatura severa corregida tras la disección cutánea y la sección de la placa uretral, este abordaje puede ser útil.7
El procedimiento de colgajo en isla onlay: OIF está indicado en niños en quienes la curvatura se corrige tras el despegamiento peneano y no se requiere la sección de una placa uretral relativamente delgada que, de otro modo, no podría tubularizarse.7 A continuación se presentan las características más destacadas de este procedimiento y de otras técnicas de reparación del hipospadias en una sola etapa.
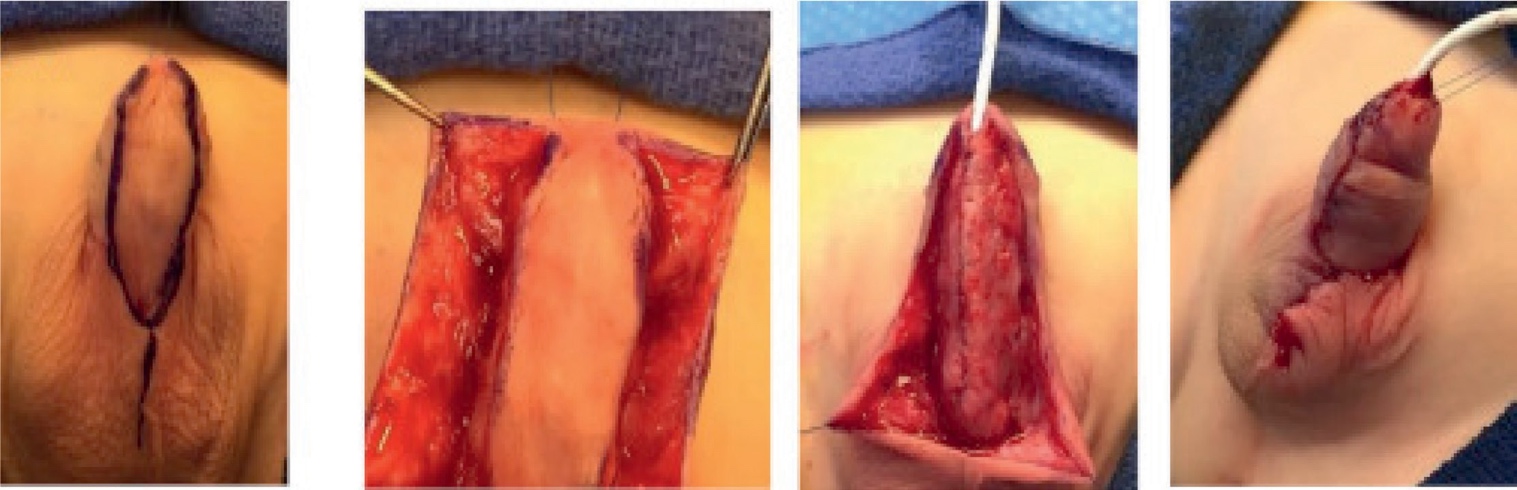
Figura 9 Reparación de hipospadias con tubo en isla. (A) Aspecto preoperatorio. La piel ventral rosada y brillante sugiere adelgazamiento de la espongiosa ventral. A pesar del meato subcoronal, se trata de una variante proximal. (B) Tras el despegamiento cutáneo, el meato se localiza en la unión penoescrotal y se canaliza con una sonda de alimentación de 8 Fr. (C) La erección artificial tras la plicatura dorsal no muestra curvatura peneana residual. (D) Se moviliza el colgajo prepucial en isla, disecando un pedículo de dartos laxo, despegándolo de la piel del cuerpo del pene en dirección a la base. (E) Uno de los bordes del colgajo se ancla a la túnica albugínea. (F) Se ajusta el colgajo a un ancho de 12 mm mediante escisión del epitelio redundante. Luego, el colgajo se cierra sobre una sonda de derivación, aproximando el borde epitelial a la porción del colgajo previamente anclada. (G) Reparación completada. [De Kraft KH, Shukla AR, Canning DA: Hypospadias. Urol Clin North Am 2010; 37: 167–181.]
Colgajo en isla onlay
- Colgajo en isla obtenido de la hoja interna del prepucio
- La anchura combinada de la placa uretral y el colgajo debe ser de 12 mm o menos, y se recorta en consecuencia; en particular, se estrecha el colgajo proximal para prevenir un divertículo en la unión de la anastomosis entre la neouretra y la uretra nativa
- La irrigación de la piel dorsal no depende del tejido subcutáneo
- Puede realizarse en hipospadias escrotal/perineal
- Sin estenosis
- La tasa de fístulas se redujo al 15%
De base lateral
- En hipospadias proximal con poca curvatura peneana30
- Glande pequeño o plano
- El ancho del colgajo lo determina la placa uretral
- Suture el extremo distal del colgajo a 2mm de la punta del glande
- El borde izquierdo se sutura primero antes de separarlo del borde derecho
Reparación con colgajo en isla tubularizado
- Casos de hipospadias severos cuando es necesario resecar la placa uretral
- Transferencia Dorso Ventral de uretroplastia de placa tubularizada (DVTPTU)
- Alta incidencia de divertículos
- Baja incidencia de formación de fístulas
Uretroplastia de placa incisa tubularizada extendida
- Descrita en el contexto de un niño cuya curvatura se corrige con disección cutánea o plicatura en combinación con una placa uretral adecuada31
- Modificaciones técnicas que incluyen la movilización de la placa uretral y corporotomías transversas, en el contexto de una curvatura ventral persistente mayor de 30 grados tras el desenfundamiento, para aumentar su aplicabilidad.
- Sin embargo, el análisis de Snodgrass et al.32 sugirió que la movilización agresiva de la placa uretral puede provocar desvascularización, aumentando el riesgo de formación de estenosis, lo que en última instancia limita la aplicabilidad del TIP proximal en el contexto de hipospadias severo con curvatura. Debido a un mayor riesgo de complicaciones, esta técnica ha caído en desuso en favor de otras reparaciones en dos tiempos, como el colgajo de Byars o la reparación STAG.
Reparación del hipospadias en dos tiempos
Procedimientos más frecuentemente realizados para el hipospadias grave
- Reparación en dos tiempos de Byars:
- En el primer tiempo
- Corrección del chordee
- Se realiza enderezamiento del pene con resección de la placa uretral ventral fijada
- Colgajo prepucial formado mediante la división de la piel dorsal se rota para cubrir el defecto ventral
- Abrir el glande ampliamente y colocar un colgajo cutáneo adecuado
- En el segundo tiempo
- El área se tubulariza en un tubo uretral
- Se realiza al menos 6 meses después del primer tiempo
- En el primer tiempo
Shukla et al realizaron la reparación del hipospadias proximal mediante la técnica del colgajo de Byar en 700 niños durante un período de 11 años.33 Informaron fístula en 21 (3%) de estos pacientes. Ninguno presentó dehiscencia completa, divertículos uretrales ni estenosis meatal. En su serie, el rango de edad de los pacientes en nuestro estudio fue de 3–12 años y la segunda etapa se realizó al menos 1 año después de la primera cirugía. Los autores enfatizaron las ventajas de un colgajo de Byar: 1) al ser un colgajo cutáneo vascularizado, lo consideraron fiable cuando se utilizó en la primera etapa y, al mismo tiempo, quedaba piel vascularizada abundante para recubrir el área cruenta que se había creado como resultado de la corrección del chordee, 2) al finalizar el procedimiento, se obtenía un aspecto circuncidado, 3) en su estudio no se observaron contracción ni pérdida, a diferencia de lo que ocurre con un injerto.33
- Reparación de hipospadias con injerto bucal/prepucial de Bracka en dos etapas34
- En la etapa 1 (Figura 10):
- Se reseca el tejido cicatricial previo, si lo hubiera
- Se movilizan las alas glandulares
- Se fija con suturas de acolchado el injerto bucal o el injerto prepucial libre para cubrir el área ventral de la cicatriz resecada
- El sitio donante para la mucosa bucal suele ser el labio o la mejilla
- No se recomienda suturar el defecto mucoso tras la extracción del injerto.
- En la etapa 2:
- Se tubulariza la placa, por lo general se realiza después de 6 meses
- Buen procedimiento para reoperar uretroplastias
- En la etapa 1 (Figura 10):
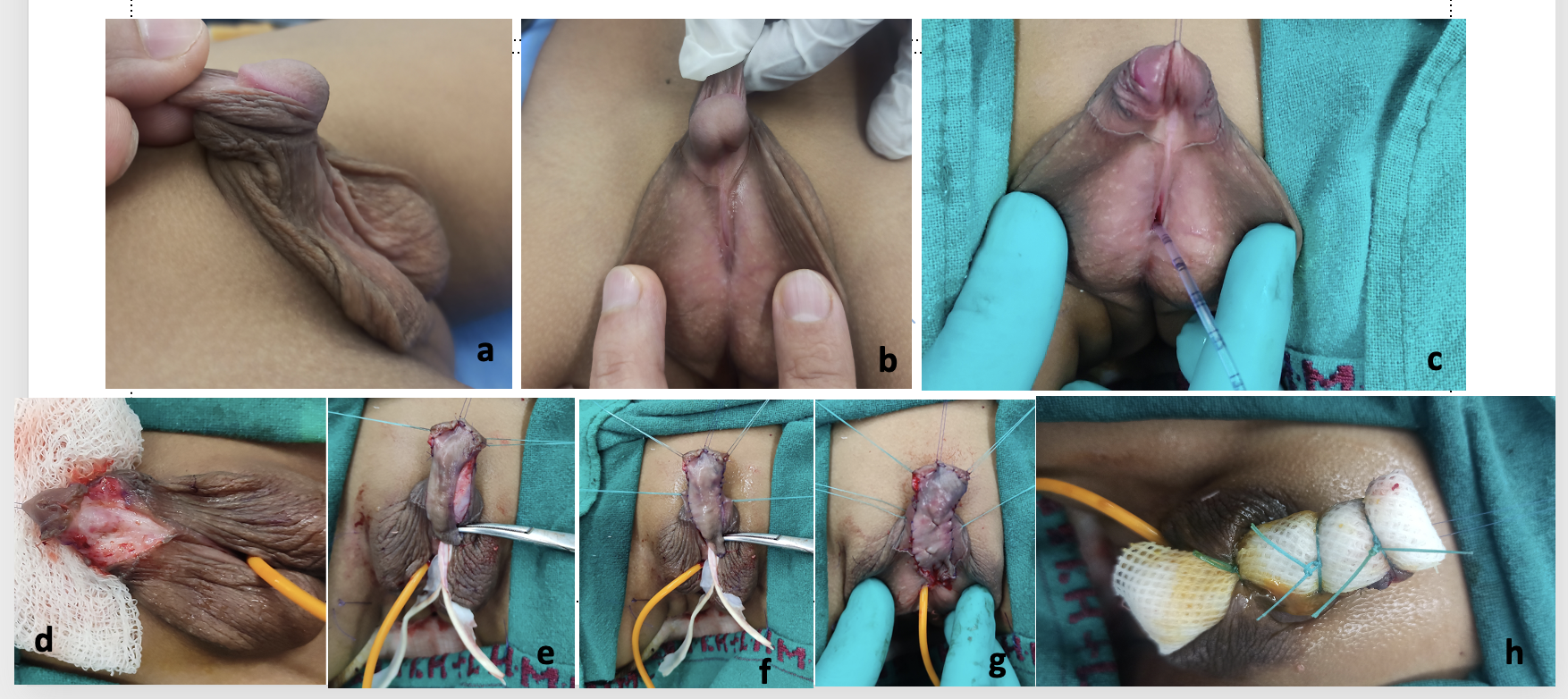
Figura 10 Cortesía del Dr. Vikram Khanna, Profesor Asociado , Cirugía Pediátrica, Lady Harding Medical College y Hospital Infantil Kalawati Saran, Nueva Delhi, a) Imagen preoperatoria que muestra hipospadias penoescrotal con transposición penoescrotal, curvatura peneana y falo corto con prepucio en capucha dorsal, b) Perfil lateral que muestra el grado de curvatura peneana y la placa uretral, c) sonda de alimentación insertada como stent utilizando el método de doble catéter
d) Desenfundamiento del tronco peneano y corrección de la curvatura peneana, e) Injerto de piel prepucial obtenido, f) Injerto suturado a la zona de las alas de la glande separadas y la zona de la placa uretral y de los cuerpos cavernosos, g) Fijación completa del injerto con quilting realizada, h) Vendaje tie-over realizado sobre el injerto y catéter dejado in situ durante 1 semana.
Bracka describió el concepto de la reparación del hipospadias en 2 tiempos.34 Tras al menos 6 meses desde la primera etapa de la reparación, puede realizarse la segunda etapa. Durante esta reparación, se corrige cualquier curvatura peneana residual, se realiza la tubularización del injerto, se crea la neouretra y se llevan a cabo la meatoplastia y la glanuloplastia. La uretroplastia se cubre con un colgajo de dartos o un colgajo de túnica vaginal. En la era actual, se ha aceptado ampliamente como tratamiento primario para pacientes con hipospadias proximal y curvatura peneana. En la serie de Bracka de reparación de hipospadias pediátrica en dos tiempos, que incluyó a 457 niños (369 reparaciones primarias y 88 reparaciones secundarias o de rescate) y 143 adultos (22 primarias y 121 secundarias), 5.7%35 desarrollaron fístulas uretrocutáneas, 7%14 desarrollaron estenosis y 4.6%29 desarrollaron estenosis de aparición tardía.34,35
El uso de la piel de la hoja interna del prepucio es una excelente opción, ya que el injerto es delgado, flexible, sin vello y resiste un medio húmedo. Se obtiene el injerto, se elimina la capa de dartos y se anastomosa ventralmente a los cuerpos cavernosos para formar la placa neouretral. La tubularización del injerto generalmente se realiza más tarde, después de 6 meses. Uno de los problemas
con el injerto de prepucio es la disponibilidad de este injerto. Esto se debe a que muchos pacientes con hipospadias proximal y curvatura ventral tienen piel peneana escasa y, toda la piel es necesaria y se utiliza para la cobertura cutánea del pene en la etapa inicial. Aunque el uso de injertos para la reparación de hipospadias se empleó principalmente en reoperaciones, algunas series también han informado buenos resultados con la reparación por etapas utilizando injertos prepuciales para la corrección primaria del hipospadias proximal.36,37
En los casos en que la piel prepucial no puede utilizarse o no está disponible, la mucosa bucal (Figura 11) se obtiene de la cara interna de la mejilla y/o de la región alveolar labial inferior y se injerta sobre los cuerpos cavernosos. Sus propiedades incluyen un mayor contenido de elastina, una rigidez relativa que proporciona buen soporte y, en última instancia, disminuye la aparición de divertículo uretral y prolapso meatal,38,39 lo que la hace adecuada para su uso en la cirugía del hipospadias. Durante la obtención del injerto de mucosa bucal, se debe evitar cruzar la comisura de la boca hacia el labio inferior, evitando así deformidades estéticas faciales. En segundo lugar, se debe tener cuidado de evitar el conducto de Stenon al obtener la mucosa de la cara interna de la mejilla.
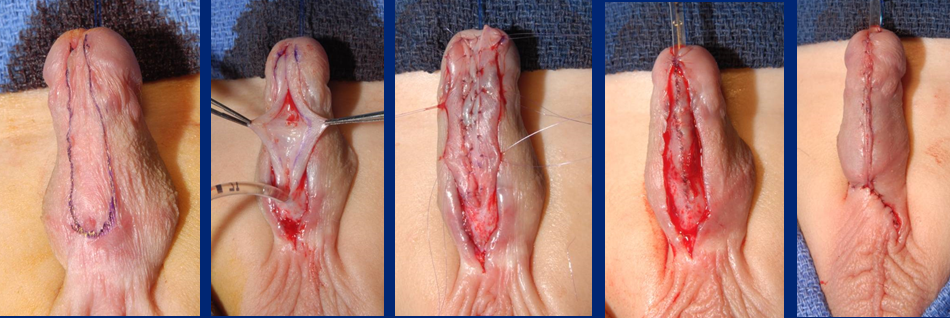
Figura 11 Tubulización del injerto inlay de mucosa bucal
Según la literatura disponible, el injerto prepucial en casos primarios es el método preferido, los otros injertos disponibles son el injerto lingual y los injertos de mucosa bucal.40,41 En los casos de hipospadias proximales, la mayoría de las veces podemos utilizar la mucosa prepucial, que no es realmente piel prepucial, es brillante, como injerto, y no encontramos deficiencia de piel en la primera etapa, ya que no estamos cubriendo el pene con piel en la primera etapa de colocación del injerto.
En una serie de 43 niños que completaron ambas etapas con seguimiento posoperatorio, Snodgrass y Bush concluyeron que el autoinjerto tubularizado en etapas resultó en un pene recto con un neomeato en posición normal en niños con el hipospadias proximal más grave en el 77%.26 Esta cifra aumentó al 98% tras 1 o 2 reoperaciones por complicaciones. En su serie, también observaron que no hubo recurrencia de la curvatura ventral después de realizar 3 corporotomías sin injerto corporal [Snodgrass]. La curvatura ventral media de estos penes fue de 70 grados, y se realizó corporotomía en el 65%, se utilizaron injertos prepuciales en el 88%.26
Manejo y cuidados posoperatorios
Drenaje urinario
Se debe asegurar el drenaje mediante una sonda de alimentación para lactantes (IFT) dejada in situ tras la reparación. Generalmente utilizamos una IFT de 6F u 8F para niños pequeños y de 10F a 12F para niños mayores, adolescentes y adultos. Se debe tener cuidado de colocar la punta del stent dentro de la vejiga de manera que no se produzcan espasmos vesicales por la irritación del trígono y que no haya anudamiento interno debido a una longitud excesiva del catéter dejado en el interior. Lo mejor es utilizar un catéter de silicona.
Apósito
El vendaje se aplica en forma circular alrededor del eje peneano tras colocar un acolchado adecuado sobre la región escrotal reparada. No debe estar ni demasiado apretado ni demasiado flojo, y la punta del glande debe quedar visible o expuesta para la inspección visual durante el período posoperatorio.
Otra alternativa podría ser aplicar un apósito y fijarlo a la pared abdominal con un apósito plástico estéril o un apósito en sándwich con Elastoplast.
Durante la reparación por etapas, cuando usamos el injerto en la primera etapa, utilizamos un vendaje tie-over (Figura 10), para fijar el injerto, y este se retira una semana después. El injerto por debajo se fija al cuerpo cavernoso subyacente mediante suturas de acolchado. El vendaje tie-over ayuda a obliterar cualquier espacio libre entre el injerto y los cuerpos cavernosos subyacentes, elimina el exceso de líquido y favorece una mejor aposición del tejido del injerto.
Complicaciones
El breve panorama de las principales complicaciones posteriores a la reparación puede estar relacionado con la uretroplastia o con complicaciones cutáneas.7
Complicaciones de la uretroplastia
- Fístula
- Dehiscencia del glande
- Síntomas obstructivos de estenosis meatal (esfuerzo miccional, micción prolongada, infección del tracto urinario y/o retención urinaria)
- Estenosis uretral
- Divertículo uretral
Complicaciones cutáneas
- Necrosis cutánea
- Torsión peneana > 30 grados- ángulo entre el plano vertical glandular normal y el verdadero >30 grados desde la línea media (especifique en sentido horario o antihorario)
- Fístula prepucial - defecto tipo fístula en la piel prepucial que no tiene contacto con la luz uretral
- Dehiscencia prepucial tras reconstrucción prepucial: defecto en la piel prepucial que recrea un prepucio incompleto
- Liquen escleroso
Estas también podrían definirse como precoces, en forma de isquemia del glande, necrosis del colgajo prepucial, obstrucción del catéter, expulsión prematura del catéter e infección de la herida. Las complicaciones tardías incluyen la formación de fístula uretrocutánea, dehiscencia del glande, estenosis meatal, curvatura peneana recurrente o residual, estenosis uretral, dehiscencia uretral y divertículo uretral.
Tabla 3 Se han destacado las complicaciones de diversos estudios de injerto en dos etapas, a Solo 48 (de 140) pacientes fueron tratados en dos etapas utilizando injerto prepucial, b 15 (30%) pacientes presentaron múltiples complicaciones, c 44 fueron casos primarios, con 8 de reoperación.
| Estudio | Número de pacientes | Seguimiento medio (meses) | Localización del meato | Tipo de reparación | Complicaciones globales (%) | Estenosis meatal (%) | Dehiscencia (%) | Estenosis uretral (%) | Divertículos uretrales (%) | Fístula (%) | Curvatura residual (%) | Otros |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferro, 200236 | 34 | 1–48 (rango) | proximal | injerto prepucial en 2 etapas | 8 (24%) | 0 | 4 (11.7%) | 1 (3%) | 1 (3%) | 2 (6%) | — | — |
| Johal, 200637 | 62 | 26 (mediana) | mediopeneano / proximal | injerto en 2 etapas | 11 (18%) | 3 (5%) | 3 (5%) | 0 | 0 | 0 | 3 (5%) | Chorro desviado 2 (3%) |
| Pippe Salle, 201614 | 48a | 29.6 (mediana) | proximal | injerto en 2 etapas | 16 (33.3%) | 0 | 7 (14.5%) | 1 (2%) | 1 (2%) | 5 (10.4%) | 2 (4.1%) | — |
| Faure, 201642 | 52 | 34 (mediana) | proximal / reoperación | injerto en 2 etapas (prepucial/BMG) | 20 (38.4%) | 8 (15.3%) | 1 (1.9%) | 4 (7.6%) | 1 (1.9%) | 8 (15.3%) | 0 | — |
| Sakr, 201743 | 23 | 12 | reoperación | en 2 etapas (injerto lingual) | 3 (13%) | 0 | 1 | 0 | 0 | 2 | 0 | — |
| Snodgrass, 201726 | 43 | 22 | proximal | en 2 etapas | 10 (24%) | 0 | 7 (16.2%) | 0 | 1 (2.3%) | 2 (4.6%) | 0 | — |
| Lanciotti, 201740 | 50 | 63.6 | proximal | en 2 etapas (injerto vesical) | 23 (46%)b | 4 (8%) | 0 | 15 (30%) | 6 (12%) | 9 (18%) | 5 (10%) | Prolapso del meato 7 (14%) |
Tabla 4 Se han resaltado las complicaciones de diversos estudios de reparación por colgajo en dos tiempos. a técnica combinada en dos tiempos con TIP distal y colgajo de Byars tubularizado, b - VC reevaluada durante el segundo tiempo con una erección artificial, c 37 se realizaron en 2 procedimientos, d 6 tuvieron tubo vesical, injertos bucales, etc., e solo 12 (de 140) pacientes fueron tratados con colgajos prepuciales en dos tiempos, f 81 (de 167) pacientes fueron tratados con colgajos prepuciales en dos tiempos, TPIF=colgajo prepucial transverso en isla; BILAB=colgajo cutáneo de base bilateral.
| Estudio | Número de pacientes | Seguimiento medio (meses) | Localización del meato | Tipo de reparación | Complicaciones globales (%) | Estenosis meatal (%) | Dehiscencia (%) | Estenosis uretral (%) | Divertículos uretrales (%) | Fístula (%) | Curvatura residual (%) | Otros |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Greenfield, 199444 | 39 | 16 | Subglandular a perineal | Colgajo en 2 tiempos (belt-fuqua) | 16 (41%) | 0 | 0 | 7 (17.9%) | 8 (20.5%) | 1 (2.5%) | — | - |
| Retik, 199445 | 58 | — | Escrotal/perineal | Colgajo en 2 tiempos | 3 (5%) | 0 | 0 | — | — | 3 (5%) | — | - |
| Cheng, 200346 | 14 | 6–36 (rango) | proximal | 2 tiemposa | 4 (28.5%) | 0 | 0 | 0 | 2 (14%) | 1 (7%) | 0b | Recesión meatal 1 (7%) |
| Hadidi, 201439 | 63c | 43 | perineal | BILAB en 1 tiempo/2 tiempos | 9 (14.2%) | — | 3 (4.7%) | — | 2 (3%) | 1 (1.5%) | — | Contracción cicatricial 3 (4.7%) |
| McNamara, 201547 | 134d | 45.6 (mediana) | proximal | Colgajo en 2 tiempos | 71 (53%) | 17 (12.7%) | 19 (14.2%) | 16 (11.9%) | 12 (9%) | 39 (29.1%) | 3 (2.2%) | - |
| Stanasel, 201548 | 56 | 38.6 | proximal | Colgajo en 2 tiempos | 38 (68%) | 5 (9%) | 3 (5%) | 8 (14%) | 8 (14%) | 32 (57%) | — | - |
| Tiryaki, 201649 | 34 | 44.8 | proximal | Colgajo de Byars en 2 tiempos | 32 (95%) | 0 | 0 | 0 | 24 (70%) | 23 (67%) | 1 (3%) | 27 prolapso uretral |
| Pippe Salle, 201614 | 12e | 29.6 | proximal | Colgajo en 2 tiempos | 4 (41.6%) | 0 | 3 (25%) | — | 0 | 2 (16.6%) | 1 (8.3%) | - |
| Chen, 201650 | 87 | TPIF - 38 (mediana)Byars – 36 (mediana) | proximal | TPIF en etapas,42 colgajo de Byars en 2 tiempos45 | TPIF 9.5%, Byars 33% | — | 0, 3 (6.6%) | 1 (2.3%), 2 (4.4%) | 1 (2.3%), 0 | 2 (4.6%), 10 (22.2%) | 0b,0b | - |
| Long, 201736 | 81f | 27.7 (mediana) | proximal | Colgajo de Byars en 2 tiempos | 40 (49%) | 5 (6%) | 6 (7%) | — | 5 (6%) | 30 (37%) | 3 (4%) | - |
| Jayanthi, 201737 | 34 | 15.2 | proximal | Ulaanbaatar modificada | 5 (14.7%) | 0 | 0 | 0 | 4 (12%) | 0 | — | Epididimitis recurrente 1 (2.7%) |
En un estudio realizado en The Children’s Hospital of Philadelphia (CHOP) entre 1996–2006, que comparó los resultados de 665 niños consecutivos sometidos a reparación de hipospadias, se encontró que la tasa de complicaciones para todos los casos de hipospadias fue del 17%.51 De los 665, 86 (13%) presentaban hipospadias proximal, definido por la localización del meato uretral proximal a la porción media del cuerpo del pene tras el desenfundamiento peniano en quirófano. Observaron que un número desproporcionado de complicaciones (35%) ocurrió en los niños con hipospadias proximal, con una tasa de complicaciones de hipospadias proximal de 39/86 (45%).51 Esto contrastó marcadamente con la tasa global de complicaciones del 17%.51
La mayoría de los pacientes sometidos a reparación de hipospadias proximal requieren un seguimiento más prolongado y estrecho para un informe detallado y honesto de las complicaciones. Se puede definir un hipospadias complicado como un niño que con frecuencia requiere múltiples procedimientos complejos para corregir las secuelas de una reparación inicial fallida.52 Debido a la mayor longitud del tubo de uretroplastia, existe un mayor riesgo de estenosis o un efecto profundo derivado de la incapacidad de la uretra reconstruida para expandirse durante la micción, lo que aumenta la resistencia al flujo urinario y, en última instancia, produce fístula y/o formación de divertículo uretral, como lo destacaron Braga et al.53 Por lo tanto, anteriormente ha habido un subregistro de las complicaciones del hipospadias proximal.
Para mejorar los resultados de la reparación del hipospadias proximal, Long y Canning51 señalaron que puede utilizarse un sistema estandarizado para cuantificar de forma sistemática la gravedad del fenotipo de hipospadias a fin de crear un lenguaje universal sobre hipospadias que facilite la colaboración entre instituciones. En la actualidad, los sistemas de puntuación utilizados son el HOSE, HOPE y GMS13,54, que incluyen diversos factores como la anchura del glande, el grado de curvatura peneana y la calidad de la placa uretral, con el objeto de calcular, para un paciente determinado, una puntuación concreta. Esto ha simplificado en cierta medida la comparación para el análisis de resultados, salvo algunas limitaciones relacionadas con el paciente y la variabilidad interobservador entre cirujanos.
También destacaron la importancia de que la evaluación del paciente y la familia se integre con el análisis del cirujano después de la intervención quirúrgica51 ya que puede que no siempre coincidan. La puntuación de percepción del pene tiene en cuenta esta limitación.55 Weber et al55 en su estudio evaluaron a 77 niños (6–17 años) que se habían sometido a reparación de hipospadias respecto de su autopercepción del pene en relación con el meato, el glande, la piel y la apariencia general. Encontraron que la intercorrelación de estos ítems “meato,” “glande” y “piel” con “apariencia general” fue buena entre los niños, los padres y los urólogos. Los pacientes con hipospadias expresaron una alta satisfacción con la apariencia del pene, que no difirió significativamente de la de sus controles pareados por edad. Sin embargo, curiosamente, los padres y los urólogos estaban menos satisfechos con la apariencia del pene que los propios pacientes.55 Esto resalta la importancia de la autoevaluación por parte del paciente y de los padres, además de la realizada por el cirujano operador.
Otro método sugerido por Long et al es mediante mentoría y trabajo en equipo51, aprovechando diversas oportunidades como reuniones, conferencias, talleres, análisis crítico de videos grabados en un grupo cerrado, retroalimentación y discusión. Esto definitivamente incrementaría la exposición y mejoraría la comprensión de esta enfermedad compleja y poco frecuente, el hipospadias proximal.
Referencias
- Baskin LS. Chapter 121 - Hypospadias. In: Coran AG, In, editors. Pediatric Surgery (Seventh Edition). Mosby; 2012. DOI: 10.1016/b978-0-323-07255-7.00121-5.
- Samuel M, Capps S, Worth A. Proximal Hypospadias. Eur Urol 2011; 40 (4): 463–468. DOI: 10.1159/000049817.
- Baskin L, Erol A, Jegatheesan P, Li Y, Liu W, Cunha G. Urethral seam formation and hypospadias. Cell Tissue Res 2001; 305 (3): 379–387. DOI: 10.1007/s004410000345.
- Baskin L, Shen J, Sinclair A, Cao M, Liu X, Liu G, et al.. Development of the human penis and clitoris. Differentiation 2018; 103: 74–85. DOI: 10.1016/j.diff.2018.08.001.
- Smith DR, Tanagho EA, McAninch JW. Smith’s General Urology. Norwalk, Conn: Appleton & Lange; Chap; 1992.
- Wein AJ, Kavoussi LR, Campbell MF. 1. 2012.
- Gerasaro TS, Brock WA, Kaplan GW. Upper Urinary Tract Anomalies Associated With Congenital Hypospadias: Is Screening Necessary? J Urol 1986; 135 (3): 537–538. DOI: 10.1016/s0022-5347(17)45729-6.
- Rajfer J, Walsh PC. The Incidence of Intersexuality in Patients with Hypospadias and Cryptorchidism. J Urol 1976; 116 (6): 769–770. DOI: 10.1016/s0022-5347(17)59004-7.
- Kaefer M, Diamond D, Hendren WH, Vemulapalli S, Bauer SB, Peters CA, et al.. The Incidence Of Intersexuality In Children With Cryptorchidism And Hypospadias: Stratification Based On Gonadal Palpability And Meatal Position. J Urol 1999; 162 (3 Part 2): 1006–1007. DOI: 10.1016/s0022-5347(01)68049-2.
- Ahmed SF, Achermann JC, Arlt W, Balen A, Conway G, Edwards Z. Society for Endocrinology UK guidance on the initial evaluation of an infant or an adolescent with a suspected disorder of sex development. 2015; 4 (5): 71–88. DOI: 10.1111/j.1365-2265.2011.04076.x.
- Hadidi AT, Azmy AF. Hypospadias surgery: an illustrated guide. 2004. DOI: 10.1111/j.1440-1754.2005.571_3.x.
- Shoor G, Acharya SK. Bedside clinics and Round questions in Pediatric Surgery. 2022.
- Arlen AM, Kirsch AJ, Leong T, Broecker BH, Smith EA, J.M.. Faculty Opinions recommendation of Further analysis of the Glans-Urethral Meatus-Shaft (GMS) hypospadias score: correlation with postoperative complications. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 11. DOI: 10.3410/f.725403208.793522967.
- Abbott JE, Heinemann A, Badalament R, Davalos JG. A clever technique for placement of a urinary catheter over a wire. Urol Ann 2015; 7 (3): 367. DOI: 10.4103/0974-7796.157959.
- Hughes IA, Houk C, Ahmed SF, Lee PA, Group LWPESC, Group ESPEC. Consensus Statement on Management of Intersex Disorders. Pediatric Clinical Practice Guidelines &Amp; Policies 2006; 91 (7): 1317–1317. DOI: 10.1542/9781610021494-part06-consensus_statement2.
- Urology S on. Timing of Elective Surgery on the Genitalia of Male Children With Particular Reference to the Risks, Benefits, and Psychological Effects of Surgery and Anesthesia. Pediatrics 1996; 97 (4): 590–594. DOI: 10.1542/peds.97.4.590.
- Bermudez DM, Canning DA, Liechty KW. Age and pro-inflammatory cytokine production: Wound-healing implications for scar-formation and the timing of genital surgery in boys. J Pediatr Urol 2011; 7 (3): 324–331. DOI: 10.1016/j.jpurol.2011.02.013.
- Belman AB, Kass EJ. Hypospadias Repair in Children Less than 1 Year Old. J Urol 1982; 128 (6): 1273–1274. DOI: 10.1016/s0022-5347(17)53458-8.
- Hadidi AT. History of hypospadias: Lost in translation. J Pediatr Surg 2017; 52 (2): 211–217. DOI: 10.1016/j.jpedsurg.2016.11.004.
- Snodgrass W, Prieto J. Straightening Ventral Curvature While Preserving the Urethral Plate in Proximal Hypospadias Repair. J Urol 2009; 182 (4s): 1720–1725. DOI: 10.1016/j.juro.2009.02.084.
- Moscardi PRM, Gosalbez R, Castellan MA. Management of High-Grade Penile Curvature Associated With Hypospadias in Children. Front Pediatr 2017; 5 (189). DOI: 10.3389/fped.2017.00189.
- Braga LHP, Pippi Salle JL, Dave S, Bagli DJ, Lorenzo AJ, Khoury AE. Outcome Analysis of Severe Chordee Correction Using Tunica Vaginalis as a Flap in Boys With Proximal Hypospadias. J Urol 2007; 178 (4s): 1693–1697. DOI: 10.1016/j.juro.2007.03.166.
- Gittes RF, McLaughlin AP. Injection technique to induce penile erection. Urology 1974; 4 (4): 473–474. DOI: 10.1016/0090-4295(74)90025-9.
- Castellan M, Gosalbez R, Devendra J, Bar-Yosef Y, Labbie A. Ventral corporal body grafting for correcting severe penile curvature associated with single or two-stage hypospadias repair. J Pediatr Urol. 2011;7:289-93. . DOI: 10.1016/j.jpurol.2012.02.009.
- Snodgrass W, Bush N. Staged Tubularized Autograft Repair for Primary Proximal Hypospadias with 30-Degree or Greater Ventral Curvature. J Urol 2017; 198 (3): 680–686. DOI: 10.1016/j.juro.2017.04.019.
- Nesbit RM. Operation for Correction of Distal Penile Ventral Curvature with or Without Hypospadias. J Urol 1966; 97 (4): 720–722. DOI: 10.1016/s0022-5347(17)63105-7.
- Duckett JW. Transverse Preputial Island Flap Technique for Repair of Severe Hypospadias. Urol Clin North Am 1980; 7 (2): 423–430. DOI: 10.1016/s0094-0143(21)01243-x.
- Ascopa HS, Elhence IP, Atri SP, Bansal NK. One stage correction of penile hypospadias using a foreskin tube. Plast Reconstr Surg 1971; 49 (1): 104–105. DOI: 10.1097/00006534-197201000-00044.
- Hypospadias Surgery: Science and Art - V.V.S. . DOI: 10.4103/jiaps.jiaps_202_20.
- Snodgrass WT, Lorenzo A. Tubularized incised-plate urethroplasty for proximal hypospadias. BJU Int 2002; 89 (1): 90–93. DOI: 10.1046/j.1464-410x.2002.02524.x.
- Snodgrass WT, Granberg C, Bush NC. Faculty Opinions recommendation of Urethral strictures following urethral plate and proximal urethral elevation during proximal TIP hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2013; 9 (6 Pt B): 990–994. DOI: 10.3410/f.718013467.793494058.
- Singh AP, Shukla AK, Sharma P, Shukla J. Two stages repair of proximal hypospadias: Review of 700 cases. J Indian Assoc Pediatr Surg 2017; 22 (3): 158. DOI: 10.4103/0971-9261.207627.
- Bracka A. Hypospadias repair: the two-stage alternative. Br J Urol 1995; 76 (6): 31–41. DOI: 10.1111/j.1464-410x.1995.tb07815.x.
- Bracka A. Buccal Mucosa: Good But Not Perfect. J Urol 2011; 185 (3): 777–778. DOI: 10.1016/j.juro.2010.12.015.
- FERRO F, ZACCARA A, SPAGNOLI A, LUCCHETTI MC, CAPITANUCCI ML, VILLA M. Skin Graft for 2-stage Treatment of Severe Hypospadias: Back to the Future? J Urol 2002; 168 (4 Pt 2): 1730–1733. DOI: 10.1097/00005392-200210020-00018.
- Johal NS, Nitkunan T, O’Malley K, Cuckow PM. The Two-Stage Repair for Severe Primary Hypospadias. Eur Urol 2006; 50 (2): 366–371. DOI: 10.1016/j.eururo.2006.01.002.
- Dessanti A, Rigamonti W, Merulla V, Falchetti D, Caccia G. Autologous Buccal Mucosa Graft for Hypospadias Repair: An Initial Report. J Urol 1992; 147 (4): 1081–1083. DOI: 10.1016/s0022-5347(17)37478-5.
- Hadidi AT. Perineal Hypospadias: The Bilateral-Based (BILAB) Skin Flap Technique. Hypospadias Surgery 2014; 49 (1): 497–506. DOI: 10.1007/978-3-030-94248-9_32.
- Lanciotti M, Betti M, Elia A, Landi L, Taverna M, Cini C, et al.. Proximal hypospadias repair with bladder mucosal graft: Our 10 years experience. J Pediatr Urol 2017; 13 (3): 294.e1–294.e6. DOI: 10.1016/j.jpurol.2017.01.011.
- Pal DK, Gupta DK, Ghosh B, Bera MK. A comparative study of lingual mucosal graft urethroplasty with buccal mucosal graft urethroplasty in urethral stricture disease: An institutional experience. Urol Ann 2016; 8 (2): 157. DOI: 10.4103/0974-7796.172214.
- Pippi Salle JL, Sayed S, Salle A, Bagli D, Farhat W, Koyle M, et al.. Proximal hypospadias: A persistent challenge. Single institution outcome analysis of three surgical techniques over a 10-year period. J Pediatr Urol 2016; 12 (1): 28.e1–28.e7. DOI: 10.1016/j.jpurol.2015.06.011.
- Faure A, Heloury Y. Response to “Re: Faure A, Bouty A, Nyo L, O’Brian M, Heloury Y. Two-stage graft urethroplasty for proximal and complicated hypospadias in children: a retrospective study.” J Pediatr Urol 2016; 12 (5): 286 1–286 7. DOI: 10.1016/j.jpurol.2016.12.007.
- Sakr A, Elkady E, Abdalla M, Fawzi A, Kamel M, Desoky E, et al.. Lingual mucosal graft two-stage Bracka technique for redo hypospadias repair. Arab J Urol 2017; 15 (3): 236–241. DOI: 10.1016/j.aju.2017.06.002.
- Greenfield SP, Sadler BT, Wan J. The Two-Stage Repair for Severe Primary Hypospadias. Yearbook of Urology 1994; 2007 (2 Pt 1): 250. DOI: 10.1016/s0084-4071(08)70198-2.
- Retik AB, Bauer SB, Mandell J, Peters CA, Colodny A, Atala A. Management of Severe Hypospadias with a 2-Stage Repair. J Urol 1994; 152 (2 Part 2): 749–751. DOI: 10.1016/s0022-5347(17)32697-6.
- CHENG EARLY, KROPP BRADLEYP, POPE JOHNC, BROCK JOHNW. Proximal Division of the Urethral Plate in Staged Hypospadias Repair. J Urol 2003; 170 (4 Part 2): 1580–1584. DOI: 10.1097/01.ju.0000084258.93064.f4.
- Canning D. Faculty Opinions recommendation of Management of Proximal Hypospadias with 2-Stage Repair: 20-Year Experience. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (4): 1080–1085. DOI: 10.3410/f.725486894.793522961.
- Canning D. Faculty Opinions recommendation of Complications following Staged Hypospadias Repair Using Transposed Preputial Skin Flaps. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2015; 194 (2): 512–516. DOI: 10.3410/f.725364224.793522958.
- Tiryaki S, Əl\Elzschwakb\Elzschwarova VE, Dokumcu Z, Ergun R, Tekin A, Yagmur I, et al.. Unexpected outcome of a modification of Bracka repair for proximal hypospadias: High incidence of diverticula with flaps. J Pediatr Urol 2016; 12 (6): 395.e1–395.e6. DOI: 10.1016/j.jpurol.2016.04.046.
- Lin H, Wang Y-Y, Li S-B, Chen Z-T, Su L-J. Staged transverse preputial island flap urethroplasty for some proximal hypospadias with moderate-to-severe chordee. BMC Urol 2016; 21 (1): 1536–1540. DOI: 10.1186/s12894-021-00948-8.
- Hanna M. Faculty Opinions recommendation of Hypospadias: Are we as good as we think when we correct proximal hypospadias? Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2016: 1477513116300432–. DOI: 10.3410/f.726422269.793519822.
- Barbagli G, Sansalone S, Djinovic R, Lazzeri M. Surgical Repair of Late Complications in Patients Having Undergone Primary Hypospadias Repair during Childhood: A New Perspective. Adv Urol 2012; 2012 (705212): 1–5. DOI: 10.1155/2012/705212.
- Braga LH, Pippi Salle JL, Lorenzo AJ. Comparative Analysis of Tubularized Incised Plate Versus Onlay Island Flap Urethroplasty for Penoscrotal Hypospadias. Yearbook of Urology 2007; 2008 (1451-6): 246–247. DOI: 10.1016/s0084-4071(08)79119-x.
- Holland AJA, Smith GHH, Ross FI, Cass DT. HOSE: an objective scoring system for evaluating the results of hypospadias surgery. BJU Int 2001; 88 (3): 255–258. DOI: 10.1046/j.1464-410x.2001.02280.x.
- Merriman LS, Arlen AM, Broecker BH, Smith EA, Kirsch AJ, Elmore JM. The GMS hypospadias score: Assessment of inter-observer reliability and correlation with post-operative complications. J Pediatr Urol 2013; 9 (6): 707–712. DOI: 10.1016/j.jpurol.2013.04.006.
- F T, TP J, RP G. RE: Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A validation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients. J Pediatr Urol 2013; 9 (6): 1016. DOI: 10.1016/j.jpurol.2013.07.022.
- Weber DM, Schonbucher VB, Landolt MA, Gobet R. Faculty Opinions recommendation of The Pediatric Penile Perception Score: an instrument for patient self-assessment and surgeon evaluation after hypospadias repair. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2008; 180 (1080-4): 1084. DOI: 10.3410/f.719560881.793500484.
Última actualización: 2025-09-21 13:35