
54: Lesão uretral
Este capítulo levará aproximadamente 7 minutos para ler.
Introdução
Os traumatismos uretrais fazem parte das emergências urológicas que frequentemente requerem coavaliação multidisciplinar. Em caso de sintomas sépticos, todos os possíveis traumatismos em outros órgãos e fontes de infecção também devem ser considerados. Em caso de sintomas agudos do escroto ou hematúria macroscópica, é necessária avaliação urológica imediata. O tratamento depende da gravidade da lesão; as opções variam desde a sondagem primária com cateter, possivelmente sob visão direta, até uma anastomose cirúrgica término-terminal.
As lesões uretrais são causadas principalmente por acidentes de trânsito. Em princípio, o mecanismo do trauma pode ser classificado como contuso ou penetrante. Além disso, há lesões uretrais após intervenções iatrogênicas (cateterismo, cistoscopia etc.) ou decorrentes da introdução de corpos estranhos no lúmen uretral. Além disso, as lesões iatrogênicas são muito mais comuns em crianças devido à uretra mais frágil e vulnerável. Consequentemente, a instrumentação transuretral deve ser realizada apenas por urologistas experientes, e o tratamento endoscópico de cálculos não deve visar à extração primária; se possível, deve-se realizar litotripsia in situ antes da extração.
Diferentes graus de lesão de uma lesão uretral são definidos:
- Laceração leve com preservação da continuidade epitelial
- Ruptura parcial do epitélio uretral
- Avulsão completa da uretra
Avaliação
O exame físico frequentemente revela sensibilidade dolorosa perineal e hematoma.
Sangue no ou proveniente do meato uretral, dificuldade/incapacidade para miccionar, hematoma perineal/perianal de crescimento rápido ou urinoma, e tumefação peniana após lesão da fáscia de Buck devem indicar a presença de uma lesão uretral.
O paciente pode queixar-se de hematúria macroscópica e de possível dificuldade miccional, podendo chegar à retenção urinária. No entanto, a gravidade da lesão não pode ser avaliada com base na hematúria.
A ruptura da uretra proximal (acima do esfíncter) com subsequente retenção urinária é frequentemente observada no contexto de uma fratura do anel pélvico próxima à sínfise.
Hematúria
Hematúria macroscópica é um possível sinal de lesões uretrais e vesicais. Em casos extremos, pode ocorrer aumento da formação de coágulos (tamponamento vesical), com possível retenção urinária. Em caso de sangramento excessivo, também pode ocorrer choque hemorrágico. Mioglobinúria, terapêutica com rifampicina ou o consumo de determinados alimentos, como beterraba ou mirtilos, também podem provocar alteração da cor da urina e devem ser considerados na anamnese. A fonte mais comum de sangramento é na bexiga ou na próstata; menos frequentemente, na uretra ou no trato urinário superior. A urina permanece constantemente vermelha na hematúria macroscópica total proveniente da bexiga ou do trato urinário superior. Qualquer sintoma associado, como disúria, indica uma causa inflamatória.
O sangramento uretral após a tração acidental de um cateter urinário também é possível. Geralmente, as lesões são leves, mas o sangramento pode parecer muito acentuado. A recolocação de um cateter urinário de grande calibre por alguns dias é a opção de tratamento de escolha. A pressão gerada sobre a lesão uretral geralmente leva a uma rápida cessação do sangramento.
Se a hematúria for acompanhada de proteinúria ou de eritrócitos dismórficos ao microscópio, um nefrologista deve avaliar urgentemente uma patologia glomerular.
No caso de hematúria indolor, deve-se recomendar uma avaliação urológica imediata com cistoscopia e, se necessário, urografia por TC para excluir um tumor maligno do trato urinário.
Exames de imagem
Um exame ultrassonográfico da bexiga é útil. Em caso de bexiga cheia, a descompressão com um cateter suprapúbico é preferível. Além disso, a inserção cuidadosa de um cateter transuretral, guiada por uretrocistografia retrógrada, ajuda a avaliar a localização da lesão. A uretrografia retrógrada é o padrão-ouro para o diagnóstico de traumas uretrais, especialmente em meninos. Por via endoscópica, a uretra pode ser realinhada utilizando um cateter transuretral inserido sobre um fio-guia.
Lesões uretrais em meninas geralmente se apresentam como uma laceração parcial da parede anterior, raramente como uma laceração completa da uretra proximal ou distal. Em casos de suspeita, a uretrocistoscopia está indicada para avaliação.
Manejo
Como o trauma uretral não é uma lesão com risco de vida, ele não se torna a principal prioridade no manejo na emergência. No entanto, é essencial considerar que esse tipo de lesão determina a qualidade de vida do paciente a longo prazo. Esse tipo de lesão está associado a altas taxas de estenose, infecções do trato urinário recorrentes, múltiplas reoperações, impotência e incontinência.
Devem ser fornecidas prontamente informações sobre possíveis complicações e riscos: quanto mais proximal for a lesão uretral, maior o risco de incontinência, impotência e formação de estenose a longo prazo.
Se houver suspeita de lesões uretrais, o cateter não deve ser inserido sem avaliação urológica especializada prévia. Deve-se garantir a drenagem urinária, e a prevenção de infecções é essencial para acelerar o processo de cicatrização.
As lesões uretrais em crianças diferem das lesões em pacientes adultos porque as crianças têm uma pelve imatura, e a bexiga encontra-se relativamente mais intra-abdominal.
Quando ocorre uma fratura pélvica, a fratura torna-se mais instável. Uma avulsão completa da uretra posterior é mais comum do que em adultos. A coexistência de lesões da bexiga e da uretra em crianças é observada em cerca de 20% dos traumatismos, e as lacerações longitudinais anteriores são detectadas com o dobro de frequência. Meninas pré-púberes têm quatro vezes mais probabilidade de ter uma lesão uretral com fraturas pélvicas do que uma mulher adulta. A incidência de lesão da uretra anterior em crianças é menor do que a lesão da uretra posterior.
Lesões da uretra feminina
Lesões leves por cavalgamento da uretra ou da vagina podem ocasionalmente resultar em hemorragia perineal significativa. Exame externo e exame endoscópico sob anestesia, fechamento das lacerações com sutura e drenagem por cateter, se necessário, são as melhores opções de manejo.
Lesões significativas são geralmente relacionadas a trauma grave e fratura pélvica e podem resultar em trauma longitudinal do colo vesical e da uretra ou deiscência uretral total por fragmentos ósseos. Em caso de dificuldade na passagem do cateter, os pacientes devem ser submetidos prontamente a cistoscopia, vaginoscopia e exame do reto.
Pacientes estáveis devem ser submetidos prontamente a uretroplastia com realinhamento uretral, reparo do colo vesical e reparo de laceração vaginal, bem como a colostomia de derivação se houver lesão retal.
Lesões da uretra masculina
Lesões anteriores da uretra masculina
As complicações da circuncisão estão entre as principais lesões uretrais distais masculinas. As circuncisões podem resultar em lesão uretral significativa, com progressão para fístulas uretrocutâneas e estenose uretral. Por outro lado, a estenose meatal pode ocorrer em decorrência de circuncisão rotineira.
Amputação da glande é uma complicação potencialmente grave da circuncisão. Métodos de circuncisão com clampe, como os dispositivos Gomco e Plastibell, ganharam popularidade devido à sua praticidade. Tais lesões são consideradas consequência do descolamento incompleto das aderências balano-prepuciais ao redor do frênulo. Os cirurgiões devem verificar se a mucosa foi completamente descolada da glande antes de inserir um clampe de circuncisão para evitar esse problema.
Se a reimplantação imediata for impossível ou o tecido amputado não estiver disponível, a reparação com enxertos de mucosa bucal deve ser realizada após a cicatrização da lesão inicial.
As lesões da uretra bulbar podem, frequentemente, ser tratadas apenas com drenagem por cateter ou com observação em caso de lesão menor. Uretrografias retrógradas e endoscopias não são essenciais, a menos que haja sangramento uretral significativo ou histórico de tentativas mal-sucedidas de instrumentação com sangue no meato uretral. Apesar do manejo precoce, podem ocorrer estenoses uretrais tardias. Incisões endoscópicas podem ser utilizadas para tratar essas estenoses se forem muito curtas.
Lesões da uretra posterior masculina
As lesões uretrais posteriores são comumente associadas a trauma contuso e fraturas pélvicas.
Devido à falta de séries de grande porte em crianças, as lesões da uretra posterior masculina continuam controversas quanto ao momento e à abordagem mais adequados para o reparo. Antibióticos de amplo espectro e drenagem urinária otimizada são essenciais, independentemente do método cirúrgico escolhido.
De acordo com vários autores, três momentos para intervenção cirúrgica são descritos abaixo:
- reparação imediata: no prazo de 48 horas,
- reparação primária tardia: no prazo de 2–14 dias,
- reparação cirúrgica tardia: no prazo de três meses.
A anastomose primária é recomendada apenas em combinação com lesão do colo vesical ou lesão retal, pois tem sido associada a altas taxas tardias de incontinência e disfunção erétil.
A maioria dos defeitos uretrais posteriores são curtos e podem ser reparados com anastomose perineal. Inicialmente, estenoses longas eram reparadas em duas etapas; mesmo assim, à medida que o campo da reconstrução uretral vem progredindo, ocorreu uma mudança de paradigma em direção ao reparo em uma única etapa, utilizando enxertos livres e pediculados de pele ou de mucosa bucal, ou uma combinação desses métodos.
Resumo
Os traumatismos uretrais em crianças são incomuns e exigem avaliação conjunta multidisciplinar para assegurar a melhor abordagem possível e evitar complicações e comorbidades a longo prazo. Os princípios de manejo estão apresentados na seção Pontos-chave abaixo.
Pontos-chave
- Lesões penetrantes decorrentes de trauma externo devem ser manejadas cirurgicamente prontamente.
- A uretrografia retrógrada é essencial para o diagnóstico de lesões uretrais.
- A drenagem urinária deve ser providenciada, e a prevenção de infecções é essencial para acelerar o processo de cicatrização.
- Recomenda-se cistostomia suprapúbica inicial para lesões uretrais graves.
- As complicações da circuncisão estão entre as principais lesões uretrais distais iatrogênicas em homens.
- O realinhamento primário pode ser realizado em pacientes estáveis com defeitos curtos.
- Os tratamentos de escolha para lesões de distração da uretra posterior são a uretroplastia posterior com anastomose primária e a uretroplastia posterior com anastomose em estágios.
- O objetivo da terapia deve ser prevenir complicações secundárias, como estenose uretral, incontinência, fístula uretrocutânea, divertículos periuretrais e impotência.
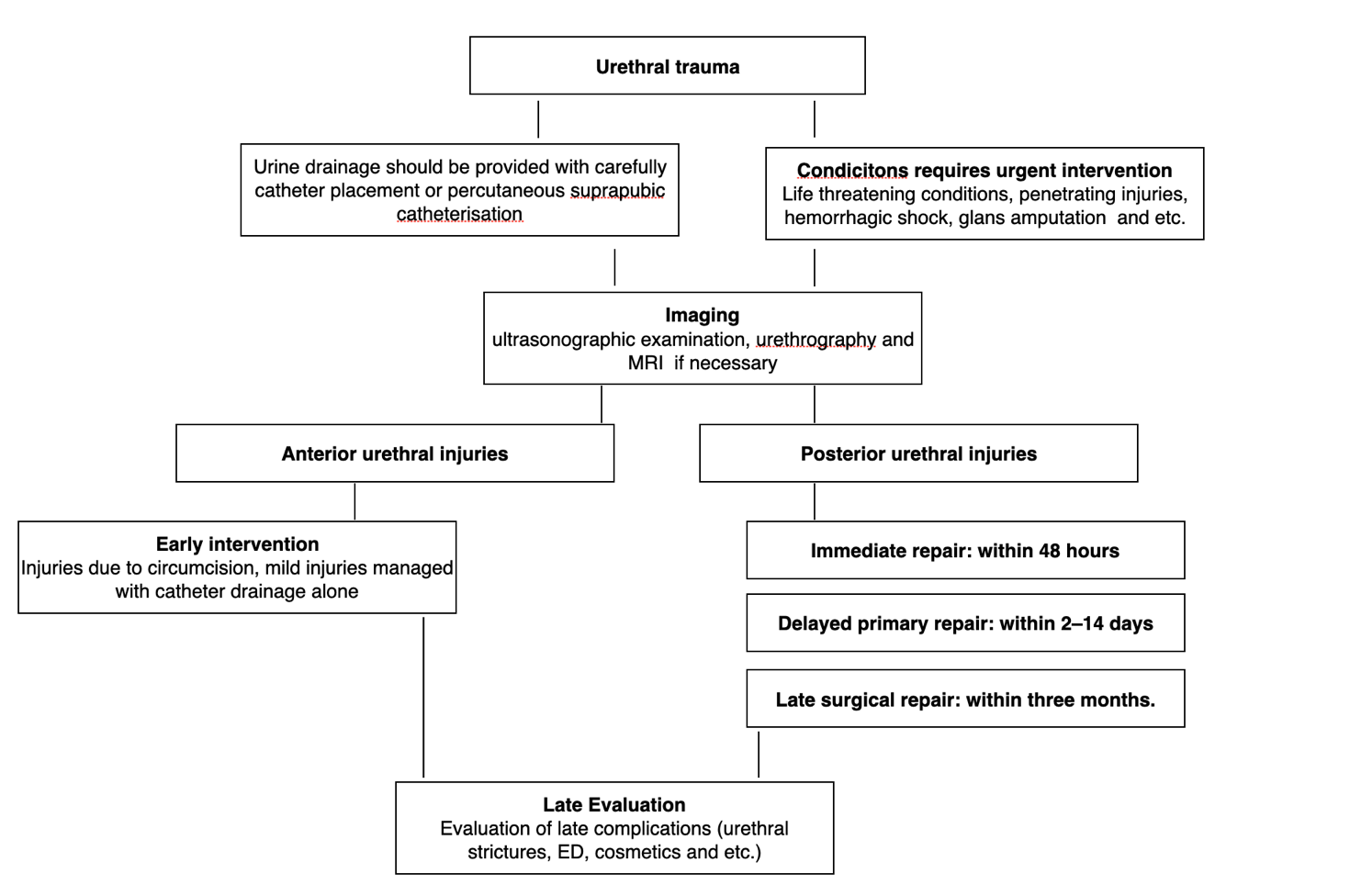
Figura 1 Avaliação e manejo de lesões uretrais.
Referências
- Chapple CR. Urethral injury. BJU Int 2000; 86 (3): 318–326. DOI: 10.1046/j.1464-410x.2000.00101.x.
- Pippi Salle JL, Jesus LE, Lorenzo AJ, Romão RLP, Figueroa VH, Bägli DJ, et al.. Glans amputation during routine neonatal circumcision: Mechanism of injury and strategy for prevention. J Pediatr Urol 2013; 9 (6): 763–768. DOI: 10.1016/j.jpurol.2012.09.012.
- Baskin LS, Canning DA, Snyder HM, Duckett JW. Surgical Repair Of Urethral Circumcision Injuries. J Urol 1997; 158 (6): 2269–2271. DOI: 10.1016/s0022-5347(01)68233-8.
- Weiss HA, Larke N, Halperin D, Schenker I. Complications of circumcision in male neonates, infants and children: a systematic review. BMC Urol 2010; 10 (1). DOI: 10.1186/1471-2490-10-2.
- PARK SANGTAE, McANINCH JACKW. Straddle Injuries to the Bulbar Urethra: Management and Outcomes in 78 Patients. J Urol 2004; 171 (2): 722–725. DOI: 10.1097/01.ju.0000108894.09050.c0.
- MD AFM, F.A.C.S., MD JS. Genital and Lower Urinary Tract Trauma. Campbell-Walsh Urology 2012 (Edition , 133): 2507–2520.e5. DOI: 10.1016/b978-1-4160-6911-9.00088-8.
- Morey AF, Broghammer JA, Hollowell CMP, McKibben MJ, Souter L. Urotrauma Guideline 2020: AUA Guideline. J Urol 2014; 205 (1): 30–35. DOI: 10.1097/ju.0000000000001408.
- BLANDY JP, SINGH MANMEET. The Technique and Results of One-stage Island Patch Urethroplasty. Br J Urol 1976; 47 (1): 83–87. DOI: 10.1111/j.1464-410x.1975.tb03922.x.
- Chapple C, Barbagli G, Jordan G, Mundy AR, Rodrigues-Netto N, Pansadoro V, et al.. Consensus statement on urethral trauma. BJU Int 2004; 93 (9): 1195–1202. DOI: 10.1111/j.1464-410x.2004.04805.x.
Ultima atualização: 2025-09-21 13:35