
4: Avaliação Urodinâmica Pediátrica
Este capítulo levará aproximadamente 21 minutos para ler.
Introdução
A avaliação urodinâmica da função do trato urinário inferior (LUT) compreende o uso de métodos apropriados de avaliação durante as fases de enchimento vesical e de micção. A instrumentação adequada dos estudos proporciona o entendimento fisiopatológico de entidades urológicas que podem afetar crianças e adolescentes, com o objetivo de otimizar seu manejo terapêutico.
A urodinâmica pediátrica requer uma equipe treinada que deve implementar uma metodologia apropriada em um ambiente adaptado ao universo pediátrico, a fim de lidar corretamente com situações de estresse e obter o máximo possível de informações clínicas urológicas.
O estudo urodinâmico do trato urinário inferior pode ser realizado de forma invasiva ou não invasiva. De modo geral, a tendência atual consiste em manejar as afecções do trato urinário inferior com avaliação urodinâmica não invasiva e utilizar métodos invasivos apenas nos casos de disfunção neuro-urológica ou malformações urológicas complexas.
Avaliação Urodinâmica Não Invasiva
As condições do trato urinário inferior (LUT) em crianças englobam um grupo de entidades com sintomas urinários sobrepostos. Essas condições resultam de distúrbios na fase de armazenamento, na fase de esvaziamento, ou de uma combinação de ambas, com diferentes graus de comprometimento. Sintomas do trato urinário inferior (LUT) podem ser observados em até 20% de crianças em idade escolar.1
A avaliação adequada é determinada pelo pediatra, e outros especialistas dão continuidade a essa avaliação. Essa abordagem é iniciada quando a criança tem por volta de 4 anos de idade, e será mais robusta se os seguintes dados puderem ser obtidos:
- Diário miccional (2-3 dias).2
- Escala de fezes de Bristol / Critérios de Roma IV / Distúrbios gastrointestinais funcionais.3,4
- Questionários (opcional): hábitos miccionais e evacuatórios, ingestão de líquidos, qualidade de vida.5
- Exame físico dos genitais, região lombo-sacra, região glútea, períneo, membros inferiores, reflexos.
- Exame de urina / urocultura: proteinúria / glicosúria.
- Urofluxometria / mensuração do resíduo urinário pós-miccional (PVR).
- Eletromiografia (EMG) do assoalho pélvico com eletrodos de superfície (adesivos)
- Ultrassonografia do trato urinário superior, características da bexiga, sinais de constipação.
- Estudos urodinâmicos / videourodinâmicos (não necessários, a menos que os pacientes sejam refratários ao tratamento inicial).
- Cistouretrografia miccional (VCUG) para detectar refluxo vesicoureteral
Existe uma variedade de questionários para a avaliação e mensuração das disfunções vesical e intestinal, da qualidade de vida e das comorbidades comportamentais, que incluem indicações e possíveis dificuldades. A ferramenta mais útil será escolhida pelo médico, considerando a avaliação clínica, o tempo disponível e a população de pacientes em estudo.5
Os distúrbios gastrointestinais funcionais em crianças ocorrem de diferentes formas e podem estar presentes em crianças de 3 ou 4 anos de idade, podendo posteriormente associar-se a disfunção vesical e infeções urinárias.6,7
Urofluxometria
Urofluxometria (com mensuração do resíduo pós-miccional) pode ser combinada com eletromiografia do assoalho pélvico (EMG) para confirmar micção disfuncional com falta de coordenação entre o detrusor e o esfíncter uretral. Estudos urodinâmicos são reservados para pacientes refratários ao tratamento inicial.8,9
A urofluxometria é um procedimento não invasivo utilizado para medir o fluxo urinário e é definida como o volume de urina que passa pela uretra por unidade de tempo, expresso em mL/s. As variáveis avaliadas são o fluxo máximo (Qmax), o fluxo médio (Qavg), o volume total urinado e o tempo total de micção. Esse método também mostra a morfologia da curva obtida durante a micção. Um fluxo normal se apresenta como uma curva em forma de sino (Figura 1). É um dos estudos iniciais usados para avaliar o esvaziamento vesical, pois fornece informações sobre a contratilidade do detrusor e o trato de saída vesical. Com essa técnica é possível evitar exames invasivos e monitorar as respostas terapêuticas.
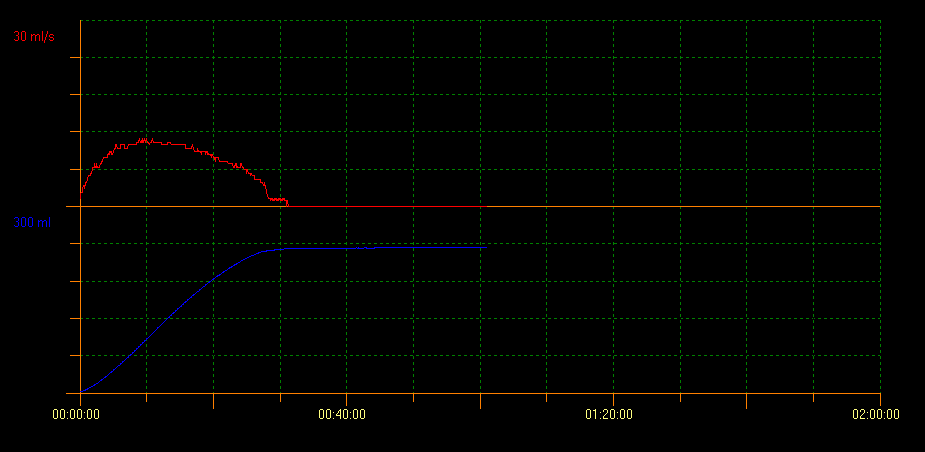
Figura 1 Fluxo normal mostrando curva em forma de sino
A urofluxometria associada à medida do resíduo pós-miccional (RPM) por ultrassonografia avalia a capacidade de esvaziamento vesical. Com esse método, diversos padrões de curva que indicam diferentes condições podem ser identificados. Um padrão em torre é indicativo de bexiga hiperativa; um padrão em staccato demonstra micção disfuncional, e um padrão de fluxo interrompido pode ser sugestivo de bexiga hipoativa. Um padrão de curva em platô é geralmente observado em pacientes com obstrução vesical anatômica (Figura 2, Figura 3, e Figura 4).10
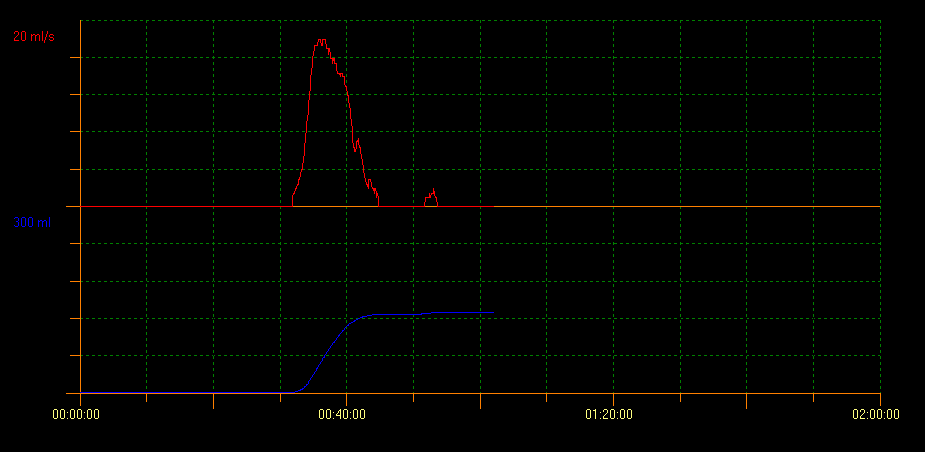
Figura 2 Padrão de curva em torre
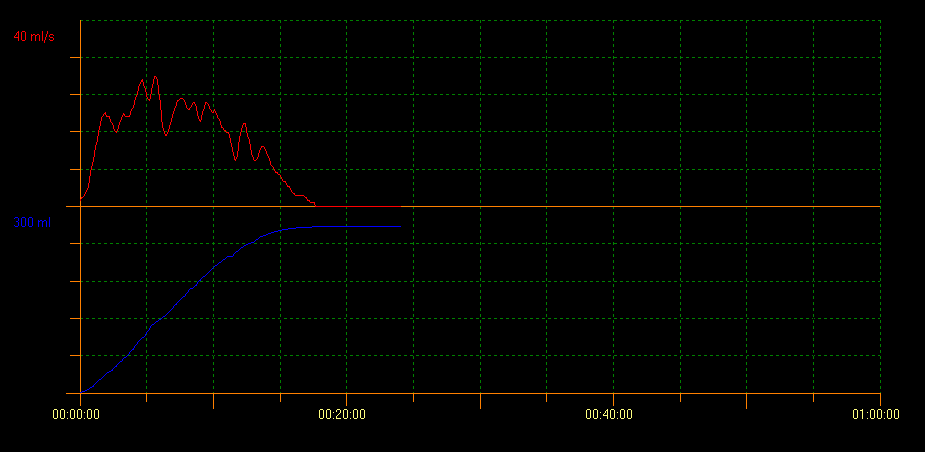
Figura 3 Padrão de curva em staccato
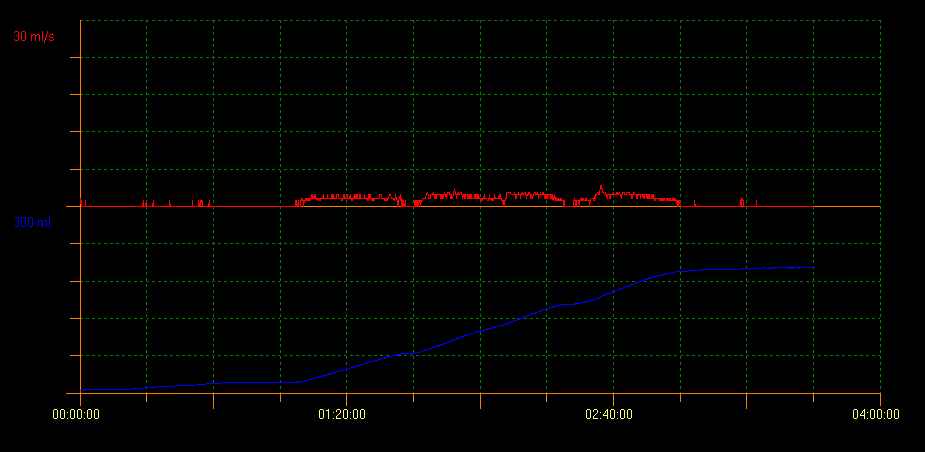
Figura 4 Padrão de curva em platô
Há uma considerável variedade de resultados entre observadores, especialmente no caso de testes de urofluxometria anormais, e essa é uma das principais limitações dessa ferramenta. Franco et al desenvolveram o conceito de índice de fluxo (FI). O FI foi criado como uma medida da taxa de fluxo real em relação à taxa de fluxo esperada: AQavg/EQavg ou AQmax/EQmax) para obter uma avaliação quantitativa do esvaziamento vesical. Assim, o FI pode ajudar a prever a taxa de fluxo estimada de forma confiável, dado um volume urinário específico dentro de parâmetros razoáveis; ajuda a comparar as taxas de fluxo reais com as ideais e, portanto, proporciona maior objetividade à análise das curvas.11 Um FI mais alto é indicativo de micção eficiente e de um padrão de curva em torre, ao passo que um FI mais baixo indica micção disfuncional e um padrão de curva em platô.
Urofluxometria e EMG do assoalho pélvico
Embora o urofluxo em staccato seja o padrão mais comum observado em crianças com diagnóstico de disfunção miccional, conforme evidenciado por urofluxo/EMG positivo durante a micção, quase um terço da população pediátrica apresenta padrão de urofluxo interrompido ou misto na disfunção miccional. Portanto, é importante incorporar eletrodos de EMG de superfície no estudo de urofluxometria, especialmente quando há suspeita de disfunção miccional por dissinergia detrusor-esfíncteriana.12 A urofluxometria associada ao EMG do assoalho pélvico não é útil apenas para diagnosticar condições específicas do LUT, mas também para monitorar objetivamente a eficácia do tratamento.13 Isso é mostrado na Figura 5.
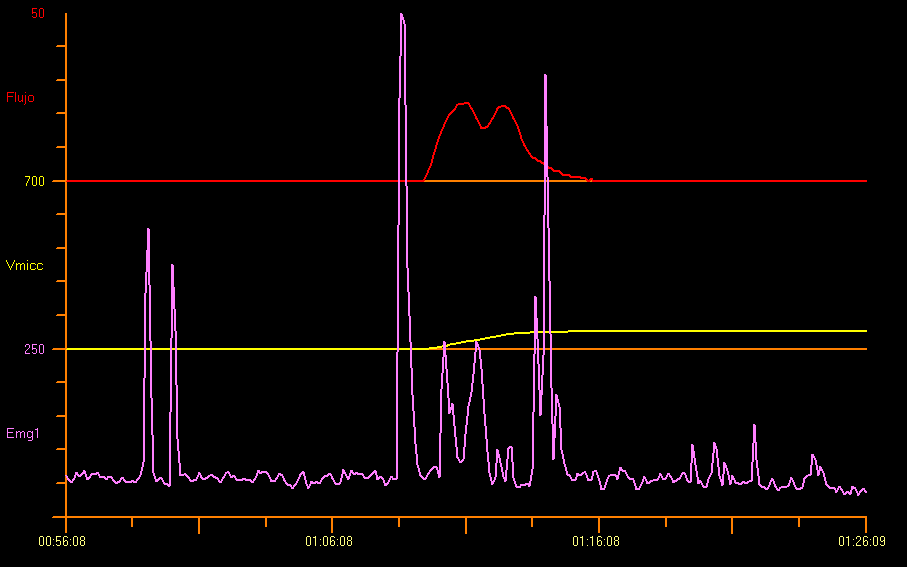
Figura 5 Fluxometria e Eletromiografia Perineal (EMG)
O tempo de latência do EMG do assoalho pélvico é definido como o intervalo entre o início do relaxamento do assoalho pélvico e o início da curva de fluxo urinário. Essa medida não invasiva, em segundos, não é útil para rastrear condições como disfunção primária do colo vesical, entre outras.13,14 Veja Figura 6 para uma explicação gráfica do tempo de latência.
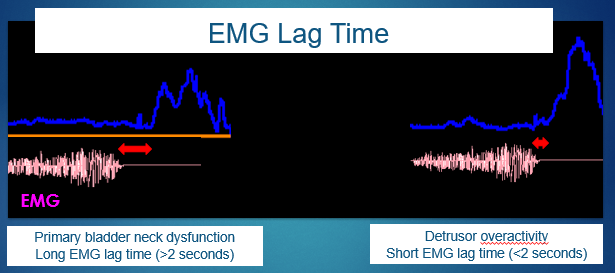
Figura 6 Tempo de latência da eletromiografia (EMG).
Mesmo ao se considerar as limitações do uso de EMG com eletrodos de superfície, é possível correlacionar o FI e o tempo de defasagem da EMG para definir o diagnóstico específico das condições do trato urinário inferior. Um tempo de defasagem próximo de 0 segundos está associado a um FI maior, o que representa hiperatividade, comumente observada no padrão de fluxo em torre. Entretanto, crianças que apresentam um tempo de defasagem superior a 6 segundos ou mesmo valores negativos de tempo de defasagem inferiores a 4 segundos apresentaram um FI menor, o que implica uma micção hipoeficiente e um padrão de fluxo em platô.15
Resíduo pós-miccional na ultrassonografia
As medições do resíduo pós-miccional em crianças neurologicamente íntegras são altamente variáveis. Em crianças de 4–6 anos de idade, uma PVR isolada > 30 ml ou > 21% da capacidade vesical (BC), em que a BC é determinada como volume urinado (VV) + PVR e expressa como percentual da capacidade vesical esperada (EBC = [idade (anos)+1] × 30 mL), recomenda-se realizar uma PVR repetida com medições em duplicata, e uma PVR repetida > 20 mL ou > 10% BC é considerada significativamente elevada. Em crianças de 7–12 anos de idade, uma PVR isolada > 20 ml ou 15% BC, ou PVR repetida > 10 ml ou 6% BC é considerada elevada. Devem ser aplicadas condições padronizadas à medição da PVR: a bexiga não deve estar subdistendida (< 50%) nem sobredistendida (> 115%) em relação à EBC, e a PVR deve ser obtida imediatamente após a micção (< 5 min).16
Quando há uma condição do trato urinário inferior, está indicada uma ultrassonografia do trato urinário superior para descartar outras anomalias, como hidronefrose e sistemas coletores duplos. A presença de alterações na parede vesical, como espessamento, trabeculação ou divertículos, pode ser um marcador de disfunção crônica do trato urinário inferior.
Avaliação urodinâmica invasiva—Cistometria
Os estudos urodinâmicos geralmente não são utilizados para avaliar sintomas do trato urinário inferior (LUT) em crianças neurologicamente íntegras, e raramente fornecem informações adicionais que justifiquem o seu uso. Esses estudos são utilizados quando há achados patológicos em exames não invasivos, se os tratamentos não são eficazes e quando sintomas como incontinência ou infecções urinárias se agravam.17
No entanto, a urodinâmica invasiva é rotineiramente utilizada na avaliação inicial, no acompanhamento de crianças com bexiga neurogênica devido à espinha bífida, quando há suspeita de disfunção neurogênica detrusor-esfincteriana (disrafismo espinhal oculto), obstrução (em válvulas uretrais posteriores), anomalias geniturinárias (extrofia, epispádias), disfunção vesical não neurogênica ou resíduo pós-miccional significativo de etiologia desconhecida.9
Durante a cistometria, a relação pressão/volume intravesical é medida para documentar a função de armazenamento e micção. Na primeira etapa do estudo, obtêm-se estes dados: estabilidade do detrusor, pressões do ponto de perda, sensação vesical e capacidade vesical. Na fase de esvaziamento, medem-se outros parâmetros: pressão miccional; pressão de abertura do colo vesical e do esfíncter urinário; eficiência e sustentação da contração do detrusor; padrão do fluxo urinário e sinergia no EMG. Por meio de um cateter retal com balão, avaliam-se as variações da pressão abdominal e sua influência na pressão vesical.
A padronização e a nomenclatura definidas pelas Diretrizes da International Children's Continence Society (ICCS) foram utilizadas.9 A pressão intravesical é medida com um cateter de duplo lúmen de 6-French colocado através da uretra. A pressão intra-abdominal foi medida utilizando um cateter de 8-French e um cateter balão de vinil colocados no reto. A bexiga foi preenchida com solução salina a 0,9% a 37,5° Celsius a uma taxa de 5–10% da capacidade vesical teórica ou esperada da criança por minuto, até uma taxa máxima de 10 mL/min.
São avaliadas as seguintes variáveis urodinâmicas: capacidade cistométrica máxima (MCC em mL); pressão detrusora ao final do enchimento (Pdet em cm de água) e pressão do ponto de vazamento do detrusor (DLPP em cm de água). Calculamos a capacidade vesical esperada (EBC) segundo a fórmula: 30 × (idade em anos + 1) mL. Capacidade vesical reduzida foi definida como < 65% da EBC.7 Definimos a capacidade cistométrica máxima quando interrompemos o enchimento pelos seguintes motivos: contração do detrusor com volume significativo de perdas; perdas que excedem a taxa de enchimento (> 10 ml / sec); pressões de risco (> 40 cm de água) refluxo vesicoureteral de alto grau em estudos vídeo-urodinâmicos, e dilatação do trato urinário. Hiperatividade do detrusor foi definida pela presença de duas ou mais contrações do detrusor maiores que 15 cm de água.18 Esvaziamento vesical ineficiente é definido por hipoatividade do detrusor ou detrusor neurogênico acontrátil.7
Fase anterior aos estudos urodinâmicos
É importante explicar em detalhe os procedimentos aos pais e aos pacientes e mostrar-lhes o serviço de urodinâmica e o material a utilizar. As instalações devem estar adaptadas a pacientes pediátricos e deve haver pessoal treinado capaz de lidar com crianças acordadas. O ambiente ideal incluiria entretenimento disponível, como jogos, tablets, televisão e videojogos, de acordo com a idade. Além disso, vale a pena salientar a importância de se obter um reto vazio, especialmente no caso de crianças com obstipação.
Recomenda-se iniciar o procedimento com uma urocultura negativa colhida no máximo 15 dias antes. Em crianças que vão iniciar cateterismo intermitente limpo (CIC), a urocultura pode não ser necessária, pois, se houver bacteriúria assintomática, isso não é considerado um fator de risco adicional e, em geral, não requer profilaxia antibiótica. A incidência global de infecções do trato urinário (ITUs) após estudos urodinâmicos é baixa (0.7%). Pacientes sem urocultura prévia à realização da urodinâmica não apresentam aumento significativo de ITUs.19
Se o paciente controla os esfíncteres, não está em programa de cateterismo intermitente limpo e está com a bexiga cheia, realiza-se urofluxometria livre com instrumentação prévia. Esses dados complementariam o relatório final sobre esse paciente.
A sedação com midazolam administrado por uma das três vias, oral, nasal ou retal, é um método seguro e eficaz e uma opção conveniente durante a cistometria, especialmente no grupo de pacientes jovens que podem sentir-se assustados e estressados ao se depararem com o procedimento a ser realizado. A maioria dos pacientes fica satisfeita com a aplicação da sedação, conforme relatado por Özmert. Nesse relatório, o grupo que recebeu início mais rápido da sedação e as menores doses, aplicadas por via nasal, apresentou desfechos mais favoráveis, apesar de ardor nasal, em comparação com o grupo que recebeu sedação oral. Outra vantagem da sedação foi que a cistometria foi realizada em menor tempo nos pacientes sedados em comparação com o grupo controle, e a cistometria não foi alterada pelo midazolam.20 O hidrato de cloral, como sedativo, é amplamente utilizado em crianças em procedimentos diagnósticos ou terapêuticos. A solução oral é uma alternativa eficaz e apropriada para sedação em crianças.21
Instrumentação urodinâmica
Em geral, um cateter transuretral de duplo lúmen 6-French é inserido após a aplicação de xilocaína como anestésico. Em alguns casos, como em crianças não colaborativas, naquelas com dificuldades de compreensão ou sensibilidade uretral preservada, ou na suspeita de obstrução uretral (válvulas uretrais posteriores), a colocação de um cateter suprapúbico de duplo lúmen 24 horas antes do exame possibilita uma melhor realização do estudo.22 Também é possível colocar um cateter de duplo lúmen em uma vesicostomia ou ureterostomia e, em seguida, fechar o estoma com um cateter de Foley com balão de silicone.
Cateteres transuretrais e retais devem ser fixados com fita adesiva ao orifício cutâneo e, por meio de tubos de conexão, são conectados aos transdutores de pressão externos e nivelados à altura da sínfise púbica. Antes de o paciente ser colocado em posição sentada e após a limpeza da pele do períneo, dois eletrodos de EMG de superfície são conectados de forma simétrica, à esquerda e à direita da área perianal, a fim de registrar a atividade dos músculos do assoalho pélvico. Além disso, um terceiro eletrodo de referência é colocado sobre uma proeminência óssea. A cistometria de enchimento é geralmente realizada em posição sentada; no entanto, também é aceitável a posição supina ou a criança nos braços da mãe.23 Consulte Figura 7 para um exemplo de posicionamento.

Figura 7 Posição do paciente
Em crianças neurologicamente íntegras e com idade suficiente para responder, a sensação de enchimento deve ser determinada seguindo a sequência padrão definida pela ICS (Sociedade Internacional de Continência): “primeira sensação de enchimento”, “primeiro desejo miccional” e “forte desejo miccional”. Após o término do ciclo miccional e dependendo da qualidade da curva, deve-se considerar se é necessário repetir o exame. Após a remoção dos cateteres e dos eletrodos de EMG, os pacientes são orientados a aumentar a ingestão de líquidos para reduzir o risco de infecção do trato urinário,23 e, em caso de desconforto, usar medicação analgésica.
Interpretação dos Resultados Urodinâmicos
É essencial saber que grande parte do tempo do estudo é despendida na fase de enchimento e uma proporção menor do tempo na fase de esvaziamento. Ciclo vesical na Figura 8.
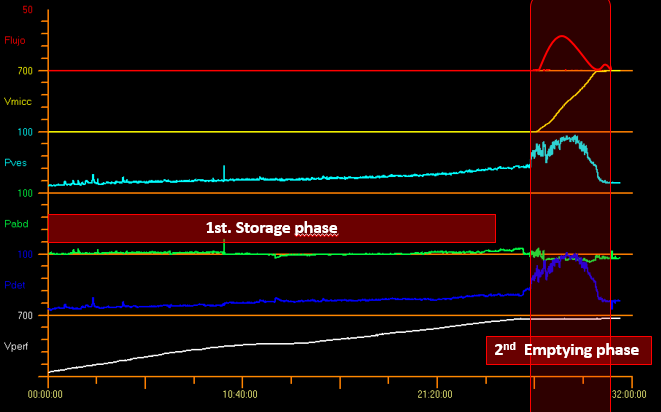
Figura 8 Ciclo vesical.
Fase de enchimento
A sensibilidade vesical pode ser um parâmetro relevante apenas no caso de crianças que são capazes de miccionar voluntariamente. A partir dos 4 anos, os seguintes dados podem ser documentados: “primeiro desejo de urinar” e “forte desejo de urinar”. A criança geralmente expressa um desejo normal de urinar quando encolhe os dedos dos pés. Além disso, a sensibilidade vesical pode ser classificada como normal, aumentada (hipersensível), reduzida (hipossensível) ou ausente.
Os parâmetros medidos durante a fase de armazenamento incluem: pressão intravesical (Pves), pressão abdominal (Pabd) e pressão detrusora (Pdet), em que Pdet = Pves - Pabd (Figura 8).
A pressão detrusora de enchimento (Pdet fill) é a pressão detrusora durante a fase de enchimento, e a pressão detrusora alcançada ao final do enchimento é chamada de pressão detrusora máxima (Pdet fill max). A elasticidade da parede vesical, ou complacência da parede, normalmente aumenta progressivamente durante a fase de enchimento e pode ser calculada com base nos pontos inicial e final da fase de enchimento (considerando a pressão de repouso em caso de hiperatividade detrusora). Assim, a complacência vesical é definida como a relação entre a variação do volume vesical e a variação da pressão detrusora (C= ΔV/ΔP; valor normal: > 10 mL/cm H2O).24 O volume de enchimento não leva em consideração a quantidade de diurese efetivamente produzida durante o teste. Para integrar esse volume, a capacidade cistométrica máxima (MCC) é calculada com o volume miccional e o volume residual pós-miccional. A variabilidade da complacência depende de vários fatores, tais como: segmento da curva utilizado para o cálculo; formato da bexiga, espessura e propriedades mecânicas/viscoelásticas da parede vesical; capacidade de relaxamento do detrusor, contratilidade e grau de resistência da via de saída vesical.25
Além disso, a forma da curva de enchimento deve ser considerada, pois fornece informação sobre a laxidade vesical. Normalmente, a pressão do detrusor permanece relativamente estável durante o enchimento vesical, o que resulta numa curva linear. Em condições patológicas, a curva de enchimento é “não linear”, com aumento da pressão do detrusor, e essas alterações devem ser documentadas.7 De modo geral, há pouca ou nenhuma alteração de pressão durante a fase de enchimento, quando a complacência é assegurada, mas não há valores de corte para definir complacência patológica. Em crianças sem lesões neuropáticas, a complacência não deve exceder em 0,05 Y mL/cm H2O a pressão vesical basal (Y = capacidade cistométrica [mL] em função da idade). Não há relato na literatura sobre a relação entre a capacidade vesical esperada (EBC) e a capacidade vesical cistométrica. Apesar disso, alguns autores sugerem que a Pdet não deve exceder 30 cm H2O na EBC.26 No nosso centro, consideramos patológicas as pressões a partir de 20 cm de água até a capacidade vesical esperada (Figura 9).

Figura 9 Padrão de complacência reduzida
Devido a essa limitação, podemos extrapolar e usar a pressão detrusora atingida na capacidade vesical esperada e Pdet fill max. Tarcan et al estudaram as pressões vesicais em crianças com mielomeningocele aos 3 anos de idade e concluíram que um valor de corte de DLPP de 20 cm H2O apresentou maior sensibilidade na predição de lesão do trato urinário superior, ao passo que uma DLPP entre 20 e 40 cm H2O não foi confiável em termos de predição de lesão. Assim, no estudo de Tarcan, 57.1% das crianças com DLPP entre 20 e 40 cm H2O, e 62.2% das crianças com DLPP maior que 40 cm H2O tinham trato urinário superior normal. Portanto, o valor de corte de DLPP usado como parâmetro único para prever lesão do trato urinário em crianças com mielomeningocele não é confiável nem preciso. É provável que coexistam outros fatores de risco, tais como baixa capacidade vesical, baixa complacência da parede vesical, pressão de enchimento elevada, dissenergia detrusor-esfincteriana e adesão à cateterização vesical, entre outros.27
Qualquer aumento fásico da pressão detrusora durante a cistometria de enchimento é definido como hiperatividade do detrusor. Essa hiperatividade envolve a presença de duas ou mais contrações do detrusor superiores a 15 cm H2O18 e pode ocorrer espontaneamente ou ser causada por tosse ou Credé. Esse aumento ou hiperatividade do detrusor pode ser neurogênico ou idiopático, como na Figura 10.28,29
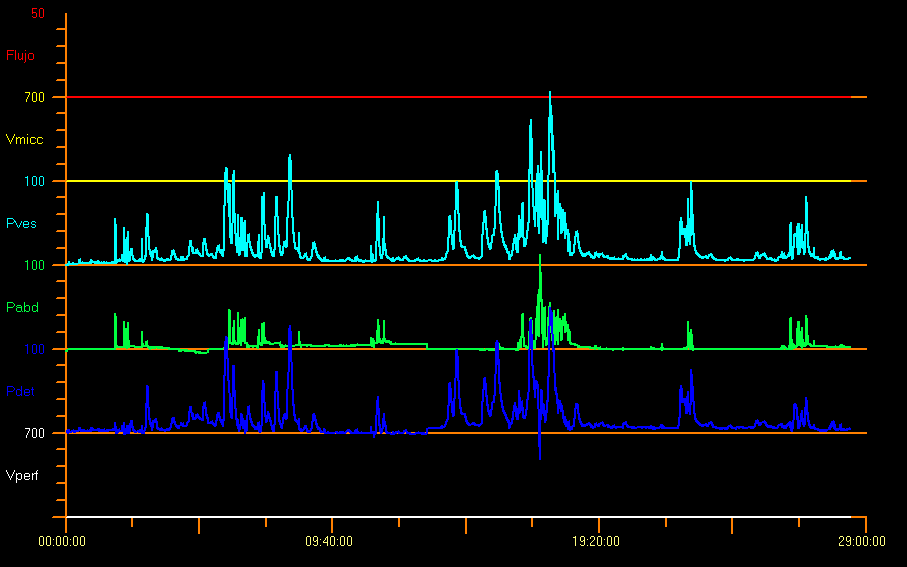
Figura 10 Padrão hiperativo
É também provável que a criança não consiga suprimir completamente essas contrações e, assim, possa ser observado um aumento da atividade eletromiográfica (EMG) do assoalho pélvico, como reflexo protetor. Alguns fatores desencadeantes, como tossir, rir, andar ou pular, podem gerar hiperatividade do detrusor. No entanto, a presença dessas contrações não implica necessariamente um distúrbio neurológico. No caso de bebês sem qualquer doença, 10% deles apresentam contrações do detrusor. Quando há contração do detrusor com pouco esforço ou sem enchimento final (quando o enchimento atinge 150% da EBC), o músculo detrusor torna-se hipoativo.9
A pressão no ponto de perda do detrusor (DLPP) indica a menor pressão detrusora na qual ocorre perda urinária na ausência de um aumento da pressão abdominal ou de uma contração do detrusor. A pressão abdominal no ponto de perda (ALPP) refere-se ao menor valor da pressão intravesical que é intencionalmente aumentado (por exemplo, devido à tosse) e que provoca perda urinária na ausência de uma contração do detrusor. Uma DLPP elevada (> 40 cm H2O) é frequentemente induzida pela diminuição da complacência da parede vesical. Uma DLPP baixa indica incompetência esfincteriana.7 A incontinência urinária de esforço está presente em adolescentes fisicamente ativos, quando a ALPP é maior do que a pressão uretral.30
Apesar dos estímulos, provavelmente será necessário remover o cateter para que a criança consiga urinar. Se o volume miccional for baixo, estamos diante de hipocontratilidade do detrusor decorrente de obstrução infravesical crônica ou de uma lesão neuropática que evolui para deterioração da micção.7
Fase de micção
A micção normal é realizada com o início voluntário de uma contração do detrusor; é sustentada e não pode ser facilmente suprimida uma vez iniciada. Durante a micção, o detrusor pode ser classificado como normal, hipoativo ou acontrátil, isto é, sem qualquer atividade durante a micção. Se a ausência de contratilidade tiver causa neurológica, é denominada arreflexia do detrusor. Caracteriza-se pela ausência completa de contração coordenada por mecanismos de controle nervoso. Quando a contração do detrusor é inadequada em magnitude e duração para esvaziar eficazmente a bexiga, estamos na presença de hipoatividade do detrusor durante a micção.9
Alguns autores relataram pressões muito superiores ao normal em crianças neurologicamente saudáveis com 1 mês de idade, com uma pressão detrusora média durante a micção de 127 cm H2O em meninos e 72 cm H2O em meninas.31 Figura 11 mostra um estudo com obstrução da saída vesical. Isso provavelmente se deve a uma atividade esfincteriana considerável e a um efeito relacionado ao cateter. No caso de crianças com medo de urinar, pode haver pressões miccionais elevadas, urofluxo interrompido ou resíduo pós-miccional (RPM) considerável.9
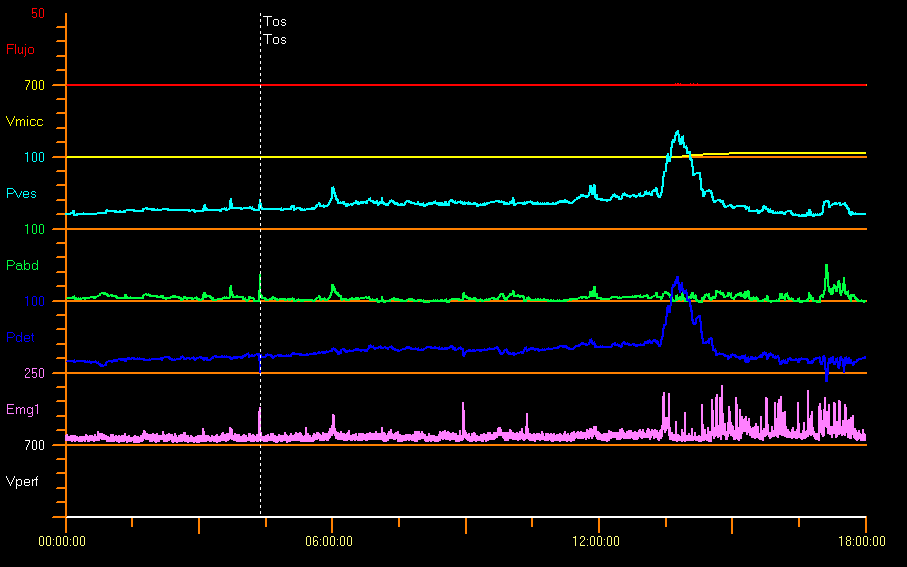
Figura 11 Obstrução infravesical
Quando há obstrução uretral anatômica (válvulas uretrais posteriores, estenose uretral, ureterocele ectópica), há uma curva de urofluxometria em platô, com Qmax baixo e constante, apesar da pressão do detrusor elevada e do relaxamento completo do esfíncter uretral externo. Ver seção Urofluxometria.
A obstrução funcional deve-se à contração do esfíncter uretral externo (constante ou intermitente) durante a micção, que cria um segmento uretral estreito. É possível documentar a atividade do assoalho pélvico com registros simultâneos de pressão/fluxo e EMG do assoalho pélvico, utilizando eletrodos de superfície.12,15
Vídeo-urodinâmica
Os estudos videourodinâmicos combinam os benefícios tanto da cistouretrografia fluoroscópica quanto da urodinâmica convencional em um único equipamento, o que torna possível realizar a avaliação anatômica e funcional simultânea do trato urinário. Figura 12 demonstra a videourodinâmica.
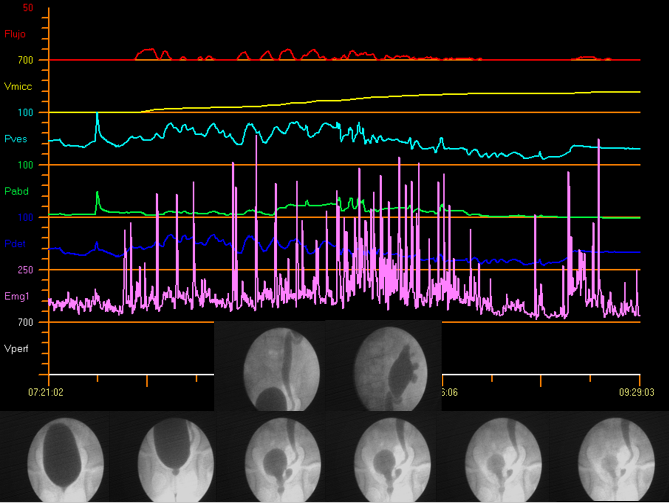
Figura 12 Videourodinâmica
A radiologia adjuvante tornou-se uma ferramenta útil no diagnóstico diferencial. Além disso, facilita a análise de imagens com tecnologia digital.32
Indicações para realizar estudos videourodinâmicos
Os estudos videourodinâmicos são indicados quando o diagnóstico permanece incerto após a realização de exames mais simples ou no caso de pacientes com condições complicadas, tais como:
- Infecções urinárias recorrentes: suspeita de refluxo vesicoureteral e sintomas urinários, como incontinência urinária.
- Malformações congênitas do trato urinário: válvula uretral posterior; Síndrome de Prune-Belly.
- Divertículos vesicais múltiplos; cirurgias prévias do trato urinário.
- Histórico de tratamento na região pélvica: ressecção de tumores, quimioterapia ou radioterapia.
- Suspeita ou histórico de obstrução vesical.
- Suspeita de dissinergia detrusor-esfincteriana (como no EMG).32
- Espinha bífida; disrafismo espinhal oculto.
- Paralisia cerebral; malformação anorretal e mielopatias.
- Malformações espinhais; escoliose grave; agenesia sacral.
- Outras entidades imunológicas e neurológicas.
- Avaliação renal pré-transplante e acompanhamento de anomalias congênitas do rim e do trato urinário (CAKUT).
Na nossa avaliação inicial dos pacientes com mielomeningocele (n:60), conseguimos realizar estudos urodinâmicos com vídeo em todos os pacientes, em média, dentro dos primeiros 8 meses de vida, e detectamos 20% das crianças com refluxo vesicoureteral, 55% com hiperatividade, 13% com hipertonia da parede vesical e 98% com PVR elevado.33
Há um custo em obter as informações adicionais fornecidas pela videourodinâmica: as crianças são expostas à radiação. O peso do paciente e a capacidade vesical são preditores independentes da exposição total à radiação. Estar ciente dessa exposição pode ajudar o médico a usar a fluoroscopia com cautela e a orientar melhor os pais quanto à exposição à radiação.34
Urodinâmica não convencional
Em 1996, De Gennaro demonstrou que é viável realizar monitorização urodinâmica contínua em crianças e que ela apresenta vantagens em relação à cistometria padrão na investigação de crianças com bexiga neuropática, mesmo quando realizada por curto período (6 horas).35
Quando não há correlação entre os volumes do diário miccional (em condições do trato urinário inferior [LUT]) ou do diário de cateterismo vesical (em bexiga neurogênica) e os resultados urodinâmicos convencionais, existe um método opcional: urodinâmica com enchimento espontâneo. Nessa modalidade não é necessário utilizar enchimento com líquido, mas o paciente deve permanecer por mais tempo no hospital, conectado ao equipamento de urodinâmica para ser monitorado. Embora, uma vez admitido, seja necessário iniciar hidratação, a duração do estudo é variável e, em geral, termina quando ocorre uma perda. Durante a micção vesical, as pressões continuam a ser medidas de forma alternada (verificação da pressão e esvaziamento) e, então, são correlacionadas com os volumes de maneira inversa à urodinâmica padrão, até o término da micção.
Urodinâmica Ambulatorial versus Convencional
A urodinâmica convencional consiste em uma avaliação altamente padronizada. No entanto, ao avaliar crianças, a confiabilidade das medições pode ser influenciada pelos efeitos do desenvolvimento e pela variabilidade dos dados, bem como pelo ambiente clínico pouco familiar. A urodinâmica ambulatorial oferece uma alternativa a essas limitações: requer enchimento natural, é medida ao longo de um período prolongado de tempo e é realizada em um ambiente amigável para crianças.
Lu et al identificaram diferentes padrões miccionais na urodinâmica ambulatorial em comparação com a urodinâmica convencional, com falta de consistência no padrão miccional identificado por cada método.36 Talvez considerar também a última evacuação intestinal, a quantidade de líquido ingerida previamente e o horário do dia em que o estudo é realizado possa explicar por que padrões miccionais menos consistentes foram observados nos estudos de urodinâmica ambulatorial.
Considerações Finais
A maioria das entidades do trato urinário inferior pode ser avaliada com métodos urodinâmicos não invasivos e pode ser manejada com tratamento e seguimento adequados.
Para algumas crianças, os estudos urodinâmicos invasivos são vivenciados como uma situação estressante em um ambiente pouco acolhedor. Para contrabalançar esse cenário e usufruir de todos os benefícios de uma prática invasiva, é essencial contar com uma equipe profissional treinada, com paciência suficiente para apoiar as crianças e suas famílias.
É fundamental que a equipe urodinâmica e todos os demais profissionais envolvidos estejam cientes das padronizações e nomenclaturas atualizadas das entidades e das boas práticas urodinâmicas, para que comuniquem e relatem os resultados em uma linguagem comum. Dessa forma, a pesquisa fornecerá achados mais sólidos.
Referências
- Linde JM, Nijman RJM, Trzpis M, Broens PMA. Prevalence of urinary incontinence and other lower urinary tract symptoms in children in the Netherlands. J Pediatr Urol 2019; 15 (2): 164.e1–164.e7. DOI: 10.1016/j.jpurol.2018.10.027.
- Lopes I, Veiga ML, Braga AANM, Brasil CA, Hoffmann A, Barroso U. A two-day bladder diary for children: Is it enough? J Pediatr Urol 2015; 11 (6): 348.e1–348.e4. DOI: 10.1016/j.jpurol.2015.04.032.
- Burgers RE, Mugie SM, Chase J, Cooper CS, Gontard A von, Rittig CS, et al.. Management of Functional Constipation in Children with Lower Urinary Tract Symptoms: Report from the Standardization Committee of the International Children’s Continence Society. J Urol 2013; 190 (1): 29–36. DOI: 10.1016/j.juro.2013.01.001.
- Robin SG, Keller C, Zwiener R, Hyman PE, Nurko S, Saps M, et al.. Prevalence of Pediatric Functional Gastrointestinal Disorders Utilizing the Rome IV Criteria. J Pediatr 2018; 195: 134–139. DOI: 10.1016/j.jpeds.2017.12.012.
- Chase J, Bower W, Gibb S, Schaeffer A, Gontard A von. Diagnostic scores, questionnaires, quality of life, and outcome measures in pediatric continence: A review of available tools from the International Children’s Continence Society. J Pediatr Urol 2018; 14 (2): 98–107. DOI: 10.1016/j.jpurol.2017.12.003.
- Lee LC, Koyle MA. The Role of Bladder and Bowel Dysfunction (BBD) in Pediatric Urinary Tract Infections. Curr Bladder Dysfunct Rep 2014; 9 (3): 188–196. DOI: 10.1007/s11884-014-0240-0.
- Austin PF, Bauer SB, Bower W, Chase J, Franco I, Hoebeke P, et al.. Faculty Opinions recommendation of The standardization of terminology of lower urinary tract function in children and adolescents: update report from the Standardization Committee of the International Children’s Continence Society. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2016; 35: 471–481. DOI: 10.3410/f.718270635.793500042.
- Schewe J, Brands FH, Pannek J. Voiding Dysfunction in Children: Role of Urodynamic Studies. Urol Int 2002; 69 (4): 297–301. DOI: 10.1159/000066129.
- Bauer SB, Nijman RJ, Drzewiecki BA, Sillen U. Faculty Opinions recommendation of International Children’s Continence Society standardization report on urodynamic studies of the lower urinary tract in children. Neurourol Urodyn 2015; 34 (7): 640–647. DOI: 10.3410/f.725510393.793507237.
- Tekgul S, Stein R, Bogaert G, Undre S, Nijman RJM, Quaedackers J, et al.. EAU-ESPU guidelines recommendations for daytime lower urinary tract conditions in children. Eur J Pediatr 2020; 179 (7): 1069–1077. DOI: 10.1007/s00431-020-03681-w.
- Franco I, Shei-Dei Yang S, Chang S-J, Nussenblatt B, Franco JA. A quantitative approach to the interpretation of uroflowmetry in children. Neurourol Urodyn 2016; 35 (7): 836–846. DOI: 10.1002/nau.22813.
- Wenske S, Van Batavia JP, Combs AJ, Glassberg KI. Analysis of uroflow patterns in children with dysfunctional voiding. J Pediatr Urol 2014; 10 (2): 250–254. DOI: 10.1016/j.jpurol.2013.10.010.
- Van Batavia JP, Combs AJ, Fast AM, Glassberg KI. Use of non-invasive uroflowmetry with simultaneous electromyography to monitor patient response to treatment for lower urinary tract conditions. J Pediatr Urol 2014; 10 (3): 532–537. DOI: 10.1016/j.jpurol.2013.11.015.
- Combs AJ, Grafstein N, Horowitz M, Glassberg KI. Primary Bladder Neck Dysfunction In Children And Adolescents I: Pelvic Floor Electromyography Lag Time–a New Noninvasive Method To Screen For And Monitor Therapeutic Response. J Urol 2005; 173 (1): 207–211. DOI: 10.1097/01.ju.0000147269.93699.5a.
- Ha JS, Lee YS, Han SW, Kim SW. The relationship among flow index, uroflowmetry curve shape, and EMG lag time in children. Neurourol Urodyn 2020; 39 (5): 1387–1393. DOI: 10.1002/nau.24349.
- Chang S-J, Chiang I-N, Hsieh C-H, Lin C-D, Yang SS-D. Age- and gender-specific nomograms for single and dual post-void residual urine in healthy children. Neurourol Urodyn 2013; 32 (7): 1014–1018. DOI: 10.1002/nau.22342.
- Bauer SB, Austin PF, Rawashdeh YF, Jong TP de, Franco I, Siggard C, et al.. International children’s continence society’s recommendations for initial diagnostic evaluation and follow-up in congenital neuropathic bladder and bowel dysfunction in children. Neurourol Urodyn 2012; 31 (5): 610–614. DOI: 10.1002/nau.22247.
- Tanaka ST, Yerkes EB, Routh JC, Tu DD, Austin JC, Wiener JS, et al.. Urodynamic characteristics of neurogenic bladder in newborns with myelomeningocele and refinement of the definition of bladder hostility: Findings from the UMPIRE multi-center study. J Pediatr Urol 2021; 17 (5): 726–732. DOI: 10.1016/j.jpurol.2021.04.019.
- Lopez Imizcoz F, Burek CM, Sager C, Vasquez Patiño M, Gomez YR, Szklarz MT, et al.. Pediatric Urodynamic Study Without a Preprocedural Urine Culture, Is It Safe in Clinical Practice? Urology 2020; 145: 224–228. DOI: 10.1016/j.urology.2020.07.054.
- Özmert S, Sever F, Tiryaki HT. Evaluation of the effects of sedation administered via three different routes on the procedure, child and parent satisfaction during cystometry. Springerplus 2016; 5 (1): 10 1186 40064–40016–3164–3167. DOI: 10.1186/s40064-016-3164-7.
- Chen Z, Lin M, Huang Z, Zeng L, Huang L, Yu D, et al.. Efficacy of Chloral Hydrate Oral Solution for Sedation in Pediatrics: a Systematic Review and Meta-Analysis [Corrigendum]. Drug Des Devel Ther 2022; Volume 16 (13): 3491–3492. DOI: 10.2147/dddt.s392339.
- Wagner AA, Godley ML, Duffy PG, Ransley PG. A Novel, Inexpensive, Double Lumen Suprapubic Catheter for Urodynamics. J Urol 2004; 171 (3): 1277–1279. DOI: 10.1097/01.ju.0000110761.60356.44.
- Wen JG, Djurhuus JC, Rosier PFWM, Bauer SB. ICS educational module: Cystometry in children. Neurourol Urodyn 2018; 37 (8): 2306–2310. DOI: 10.1002/nau.23729.
- Gilmour RF, Churchill BM, Steckler RE, Houle A-M, Khoury AE, McLorie GA. A New Technique for Dynamic Analysis of Bladder Compliance. J Urol 1993; 150 (4): 1200–1203. DOI: 10.1016/s0022-5347(17)35727-0.
- Chin-Peuckert L, Komlos M, Rennick JE, Jednak R, Capolicchio J-P, Salle JLP. What is the Variability Between 2 Consecutive Cystometries in the Same Child? J Urol 2003; 170 (4 Part 2): 1614–1617. DOI: 10.1097/01.ju.0000084298.49645.27.
- Landau EH, Churchill BM, Jayanthi VR. The sensitivity of pressure specific bladder volume versus total bladder capacity as a measure of bladder storage dysfunction. J Pediatr Surg 1994; 30 (5): 761. DOI: 10.1016/0022-3468(95)90736-x.
- Tarcan T, Sekerci CA, Akbal C, Tinay I, Tanidir Y, Sahan A, et al.. Is 40 cm H2O detrusor leak point pressure cut-off reliable for upper urinary tract protection in children with myelodysplasia? Neurourol Urodyn 2017; 36 (3): 759–763. DOI: 10.1002/nau.23017.
- Rosier PFWM, Schaefer W, Lose G, Goldman HB, Guralnick M, Eustice S, et al.. International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow study. Neurourol Urodyn 2017; 36 (5): 1243–1260. DOI: 10.1002/nau.23124.
- Abrams P. Describing bladder storage function: overactive bladder syndrome and detrusor overactivity. Urology 2003; 62 (5): 28–37. DOI: 10.1016/j.urology.2003.09.050.
- Bauer SB, Vasquez E, Cendron M, Wakamatsu MM, Chow JS. Pelvic floor laxity: A not so rare but unrecognized form of daytime urinary incontinence in peripubertal and adolescent girls. J Pediatr Urol 2018; 14 (6): 544.e1–544.e7. DOI: 10.1016/j.jpurol.2018.04.030.
- Bachelard M, Sillén U, Hansson S, Hermansson G, Jodal U, Jacobsson B. Urodynamic Pattern In Asymptomatic Infants: Siblings Of Children With Vesicoureteral Reflux. J Urol 1999; 162 (5): 1733–1738. DOI: 10.1016/s0022-5347(05)68226-2.
- Marks BK, Goldman HB. Videourodynamics. Urol Clin North Am 2014; 41 (3): 383–391. DOI: 10.1016/j.ucl.2014.04.008.
- Sager C, Burek C, Corbetta JP, Weller S, Ruiz J, Perea R, et al.. Initial urological evaluation and management of children with neurogenic bladder due to myelomeningocele. J Pediatr Urol 2017; 13 (3): 271.e1–271.e5. DOI: 10.1016/j.jpurol.2016.12.024.
- Ngo TC, Clark CJ, Wynne C, Kennedy WA. Radiation Exposure During Pediatric Videourodynamics. J Urol 2011; 186 (4s): 1672–1677. DOI: 10.1016/j.juro.2011.04.014.
- De Gennaro M, Capitanucci M, Silveri M, Mosiello G, Broggi M, Pesce F. Continuous (6 Hour) Urodynamic Monitoring in Children with Neuropathic Bladder. Eur J Pediatr Surg 1996; 6 (S 1): 21–24. DOI: 10.1055/s-2008-1071032.
- Lu YT, Jakobsen LK, Djurhuus JC, Bjerrum SN, Wen JG, Olsen LH. What is a representative voiding pattern in children with lower urinary tract symptoms? Lack of consistent findings in ambulatory and conventional urodynamic tests. J Pediatr Urol 2016; 12 (3): 154.e1–154.e7. DOI: 10.1016/j.jpurol.2016.02.006.
Ultima atualização: 2025-09-21 13:35