
2: Exames de imagem do trato urinário
Este capítulo levará aproximadamente 23 minutos para ler.
Introdução
O diagnóstico por imagem é uma ferramenta poderosa para compreender a história natural de muitas condições que afetam o trato geniturinário (GU), tanto do ponto de vista anatômico quanto do funcional. Com uso otimizado, o diagnóstico por imagem melhora os desfechos dos pacientes ao mesmo tempo em que minimiza o risco para o paciente. Múltiplas modalidades estão disponíveis para obter imagens detalhadas do corpo humano, incluindo ultrassonografia (US), ressonância magnética (MRI), tomografia computadorizada (CT), cintilografia nuclear e fluoroscopia/ radiografia. Os avanços tecnológicos nessas modalidades são contínuos.
No contexto pediátrico, as indicações para exames de imagem diagnóstica dependem não apenas da apresentação clínica, mas também da idade (ou nível de desenvolvimento) do paciente. Pode ser necessária mais de uma técnica de imagem para avaliar plenamente a anatomia e a fisiologia do trato geniturinário (TGU). Embora a apresentação clínica seja primordial e muitas vezes permita uma abordagem algorítmica aos exames de imagem, a melhor abordagem em um adolescente pode diferir daquela em um bebê ou em uma criança pequena.
Considerações sobre Radiação
Nas últimas duas a três décadas, clínicos e leigos têm se preocupado mais com a exposição à radiação de imagem médica e seus potenciais perigos, especialmente em pacientes pediátricos. O risco de futuros cânceres pode ser maior em crianças devido a vários fatores. Primeiro, crianças pequenas são menores do que adultos, levando a mais energia cinética por unidade de massa para a mesma quantidade de exposição. As crianças também apresentam maiores taxas de proliferação celular, aumentando a radiossensibilidade. Por fim, as crianças têm maior expectativa de vida a partir do momento da exposição à radiação, permitindo que mutações cromossômicas induzidas pela radiação se tornem clinicamente relevantes.1
Em muitos casos, a questão clínica pode ser respondida sem o uso de radiação ionizante. No entanto, deve-se ponderar cuidadosamente os riscos e benefícios de um procedimento. Nos casos de trauma, o padrão-ouro continua a ser uma TC do abdómen e pelve com contraste.2 Deve tranquilizar o clínico solicitante saber que vinte anos de melhorias na tecnologia de TC permitiram doses entre dez e cem (ou mais) vezes mais baixas do que as do virar do milénio.3 Por outro lado, muitos clínicos não têm consciência de que uma única radiografia abdominal (KUB) não poupa muita radiação em comparação com uma TC moderna do abdómen.4
Embora a RM possa parecer preferível à TC do ponto de vista da exposição à radiação, a sedação para RM ainda é necessária na maioria das crianças com menos de aproximadamente 8 anos de idade. Os riscos da sedação (especialmente quando repetida) para crianças ainda não estão claros. Tempos de aquisição mais rápidos, interfaces de realidade virtual e programas robustos de child life têm potencial para minimizar a necessidade de sedação.5
Perguntas a serem feitas ao escolher uma investigação diagnóstica são:
- Este exame responderá à pergunta clínica?
- Há algum exame anterior que responda à pergunta clínica atual?
- Existe uma alternativa mais segura (considere a radiação ou a necessidade de sedação)?
- Qual é o nível de desenvolvimento do meu paciente?
Se houver alguma dúvida, é recomendável discutir com o seu radiologista.
Contraste em Exames de Imagem do Trato Urinário
Agentes de Contraste Iodados
Contraste iodado é utilizado para TC e VCUG. Ao solicitar um procedimento que envolva contraste, o clínico deve estar ciente de riscos potenciais. O primeiro é o risco de uma reação alérgica ou do tipo alérgico grave. Esses eventos adversos são altamente improváveis com os agentes de contraste modernos. Uma estimativa para a taxa de reações do tipo alérgico é de 0,6%, das quais a maioria é leve e autolimitada. Para reações graves, a estimativa é de 0,04%. Antecedente de reação prévia do tipo alérgico a contraste iodado é o fator de risco mais claro e importante para uma reação subsequente. O risco em pacientes com tal antecedente deve ser cuidadosamente ponderado em relação ao benefício de uma TC subsequente. As evidências permanecem inconclusivas quanto aos benefícios da premedicação.6
O segundo risco que o médico solicitante deve considerar é o risco de lesão renal aguda induzida por contraste (CI-AKI), definida como uma deterioração súbita da função renal causada pela administração intravascular de contraste iodado. Infelizmente, o risco real dessa entidade é desconhecido, mesmo em adultos. Como ocorre com as reações do tipo alérgico, há um fator de risco que é geralmente aceito, nas melhores práticas, como predisponente à CI-AKI; esse fator de risco é a insuficiência renal pré-existente. Nenhum limiar claro de eGFR foi estabelecido (acima do qual o risco possa ser ignorado). No entanto, o American College of Radiology (ACR) recomenda um ponto de corte de eGFR de 30 mL/min/1.73 m.26
O cálculo da TFGe em crianças requer o conhecimento da altura do paciente e da creatinina sérica. A TFGe aproximada é então dada pela equação de Schwartz à beira do leito:6
TFG (mL/min/1.73 m2) = 0.41 × altura / creatinina sérica
Existem fórmulas mais recentes que fornecem estimativas mais precisas da função renal com base na creatinina sérica ou na cistatina C, incluindo as equações CKiD-U25, que são ajustadas por idade, sexo e altura.7 Uma calculadora está disponível aqui. É importante observar que pacientes com doença renal crônica dependentes de diálise podem receber contraste iodado sem risco de LRA, pois têm rins não funcionantes.
Agentes de contraste para RM
Para a ressonância magnética com contraste, utiliza-se um quelato de gadolínio. As reações alérgicas a esses agentes são ainda menos prováveis do que ao contraste iodado, com uma taxa aproximada de 0,05%. O manejo das reações alérgicas ao gadolínio é o mesmo que para os agentes de contraste iodados, e isso será discutido abaixo. Um risco exclusivo dos agentes de gadolínio é a fibrose sistêmica nefrogênica (NSF), uma doença semelhante à esclerodermia que pode levar a contraturas articulares e falência de órgãos e, ocasionalmente, ser fatal.6 Essa entidade ainda é pouco compreendida, mas, felizmente, é bastante rara. Pacientes com lesão renal aguda, doença renal crônica em estágio 4 ou 5, ou aqueles em diálise podem ter até 7% de risco de desenvolver NSF com certos agentes de gadolínio (tipos I ou possivelmente III). O uso de gadolínio nesses pacientes ainda pode ser apropriado em casos raros em que o benefício potencial de uma ressonância magnética com contraste seja muito elevado. Entretanto, obter consentimento informado nessas circunstâncias é uma boa prática. Sempre que possível, deve-se utilizar um agente de gadolínio de menor risco (grupo II) nessa população.6
Agentes de contraste para ultrassonografia
Agentes de contraste por ultrassom consistem em microesferas de fosfolipídios ou proteínas que contêm um gás inerte ecogênico. Esses agentes melhoram temporariamente a resolução de contraste do ultrassom e são aprovados para uso intravenoso e endoluminal. É necessário software dedicado para ultrassom. Os agentes de contraste por ultrassom são muito seguros, com reações graves ocorrendo em aproximadamente 0,01% dos casos. Não há toxicidade renal conhecida nas doses aprovadas.6
Manejo de reações do tipo alérgico
As recomendações atuais do Manual sobre Meios de Contraste do Colégio Americano de Radiologia para o manejo de reações alérgicas recomendam a administração imediata de epinefrina na presença das seguintes situações:
- Broncoespasmo grave
- Eritema difuso com hipotensão profunda
- Edema laríngeo
- Hipotensão com taquicardia
O esquema posológico atual está resumido na tabela abaixo (Tabela 1).8
Tabela 1 Dosagem de epinefrina para reações ao meio de contraste.
| Via | Dose | Observações | Repetir | Dose máxima |
|---|---|---|---|---|
| intravenosa | 0.01 mg/kg | lentamente numa perfusão IV de fluidos em curso | A cada 5-15 minutos | 1 mg |
| intramuscular | 0.01 mg/kg | A cada 5-15 minutos | 1 mg | |
| Auto-injetor 15–30 kg | 0.15 mg | Use IV (acima) se menos de 15 kg | ||
| Auto-injetor > 30 kg | 0.3 mg |
Critérios de Adequação do ACR
Os critérios de adequação do Colégio Americano de Radiologia (ACR) são recomendações de consenso disponíveis gratuitamente online para o clínico em busca do exame de imagem apropriado em várias situações. As recomendações são elaboradas por painéis de especialistas e são atualizadas com frequência.
Tabela 2 Recomendações de ultrassonografia renal dos Critérios de Adequação do ACR.
| Indicação | Observações |
|---|---|
| Neonato com UTD pré-natal, ultrassonografia pós-natal inicial | Idealmente com pelo menos 72 horas de vida |
| Neonato com UTD pré-natal e ultrassonografia pós-natal normal | Acompanhamento em 1–6 meses a critério do clínico |
| Neonato com UTD pré-natal e grau SFU 1-2 ou APRPD menor que 15 mm na ultrassonografia pós-natal | Considerar estudo miccional como investigação complementar |
| Neonato com UTD pré-natal e grau SFU 3-4 ou APRPD maior que 15 mm na ultrassonografia pós-natal | Estudo miccional e cintilografia do sistema coletor também recomendados |
| Hematúria atraumática | Quando macroscópica ou associada à proteinúria |
| Suspeita de urolitíase | |
| ITU febril | Em criança com menos de 2 meses |
| ITU febril recorrente ou resposta inadequada aos antibióticos |
Modalidades de imagem
Ultrassonografia
Em crianças, a ultrassonografia (US) é uma modalidade muito utilizada. É quase sempre a primeira linha de investigação em suspeita de anomalias renais (trauma é a exceção notável). A US é barata, não envolve radiação ionizante e é prontamente disponível. A desvantagem é ser dependente do operador. Especialmente quando a interpretação é remota, o radiologista depende fortemente do ultrassonografista.
Para as indicações abaixo, a ultrassonografia é recomendada como modalidade de imagem inicial.8,9
Anatomia renal
Os tamanhos renais de acordo com a idade estão bem estabelecidos e o crescimento adequado pode ser prontamente demonstrado por ultrassonografia. Há uma margem de erro aproximada de ± 7 mm, dependendo dos planos de imagem ou do movimento do paciente (com a TC servindo como padrão-ouro), o que significa que a comparação ao longo de várias ultrassonografias prévias fornecerá uma indicação mais confiável do crescimento renal (ou da sua ausência). Os rins podem ser lobulados ou apresentar colunas de Bertin proeminentes como variantes normais.
A diferenciação corticomedular é normalmente muito evidente em recém-nascidos. À medida que os glomérulos corticais são fisiologicamente reduzidos com a maturação da criança, o córtex normalmente se torna mais hipoecoico. Assim, o rim normal em uma criança mais velha ou adolescente se assemelhará ao aspecto do adulto, com ecogenicidade do córtex e da medula quase isoecoica, contrastando claramente com o seio renal brilhante. A familiaridade com o aspecto normal do rim em diferentes idades é essencial para o radiologista pediátrico e permite o diagnóstico de anormalidades sutis.

Figura 1 Rim normal em um lactente de quatro meses.
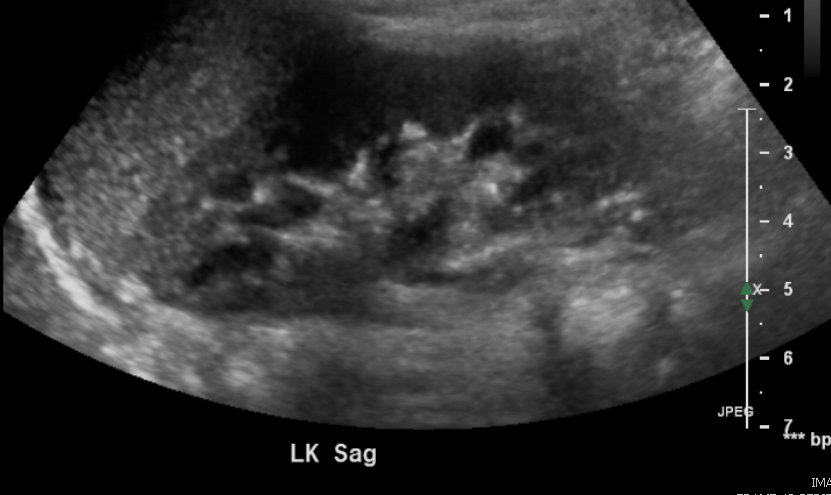
Figura 2 Rim normal em uma criança de 3 anos.
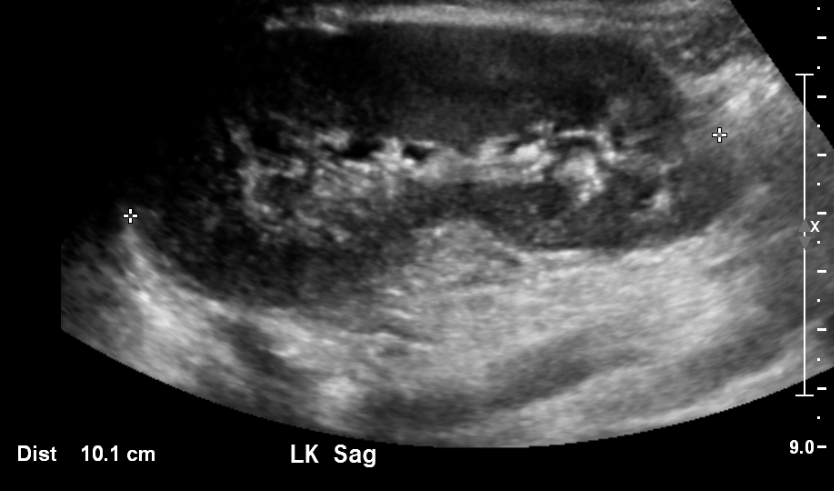
Figura 3 Rim normal em uma criança de 11 anos.
Acompanhamento da Dilatação do Trato Urinário Pré-natal
Esta é a indicação mais comum para uma ultrassonografia renal pediátrica em contexto ambulatorial. A arquitetura do sistema coletor dilatado geralmente é bem demonstrada pela ultrassonografia e pode fornecer pistas sobre a etiologia. Apesar de muitos esforços de padronização (iniciados em 1988 e ainda em curso), a terminologia descritiva tem sido lamentavelmente inconsistente. Essa inconsistência dificultou os esforços para correlacionar desfechos urológicos com o grau de dilatação do sistema coletor pré-natal. Embora os critérios de adequação do ACR se baseiem no sistema de classificação da SFU de 1988, a maioria dos hospitais pediátricos passou a adotar o sistema de classificação UTD. Este sistema de classificação foi desenvolvido em 2014. O UTD introduziu uma terminologia descritiva unificada tanto para a ultrassonografia pré- e pós-natal, a fim de facilitar uma avaliação perinatal padronizada. É aconselhável que o clínico se familiarize com a terminologia utilizada no serviço de radiologia ao qual está afiliado e incentive a padronização sempre que possível.
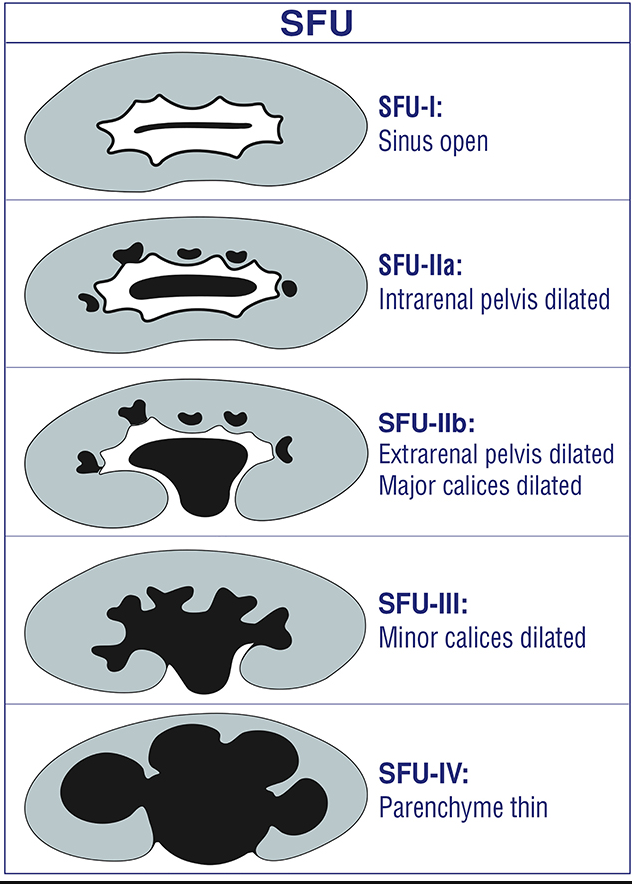
Figura 4 Classificação SFU da dilatação do sistema coletor
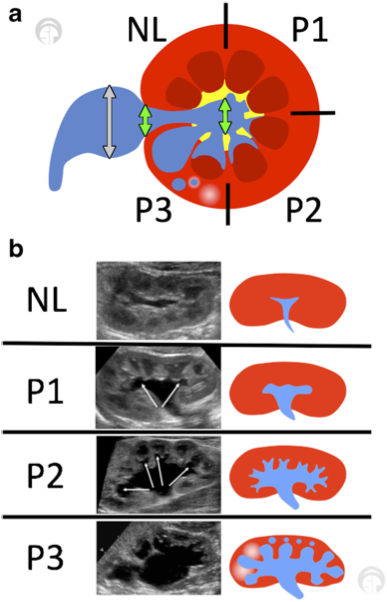
Figura 5 (a) A classificação de dilatação do trato urinário (UTD) mostra uma vista transversal da região renal média/interpolar. Setas verdes indicam o diâmetro anteroposterior (usar a maior medida). A pelve extrarrenal não deve ser incluída (setas cinzas). (b) Vistas longitudinais de vários graus dentro do sistema de classificação UTD. Adaptado de Chow et al 2017.10
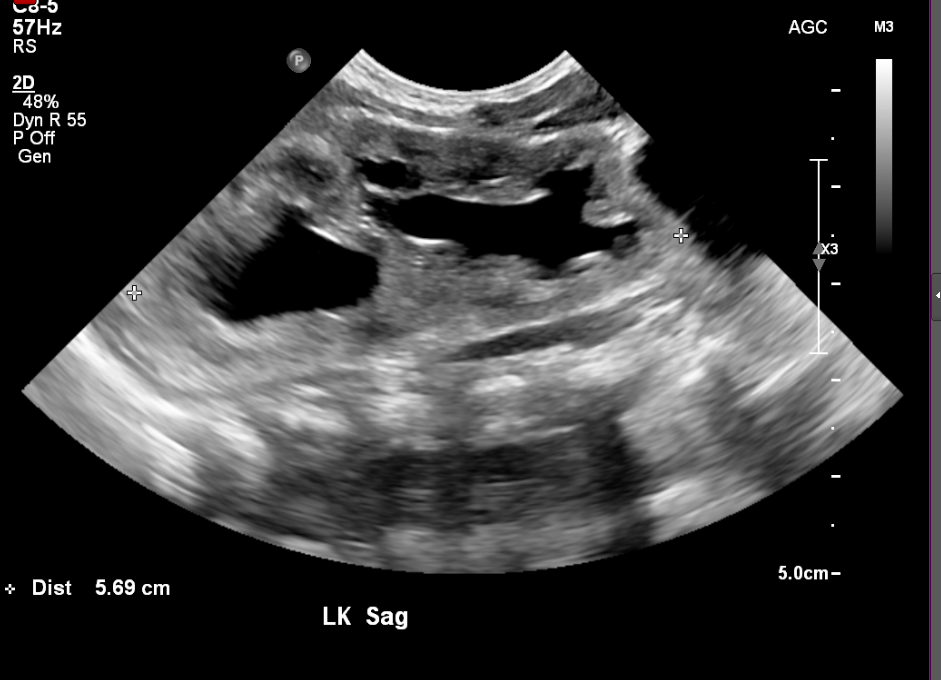
Figura 6 Sistema coletor duplicado em um recém-nascido

Figura 7 Mesmo paciente da (Figura 6) com duas semanas de idade, mostrando dilatação mais acentuada

Figura 8 Obstrução da junção pieloureteral

Figura 9 Caliectasia grave e adelgaçamento cortical em um paciente com válvulas uretrais posteriores
Rastreamento de Tumor em Condições Genéticas Predisponentes, como Beckwith-Wiedemann ou WAGR
A ultrassonografia pode detectar massas sólidas sutis em crianças pequenas, como ilustrado pelo exemplo abaixo. A frequência do rastreamento e a faixa etária variam de acordo com a condição predisponente específica.11
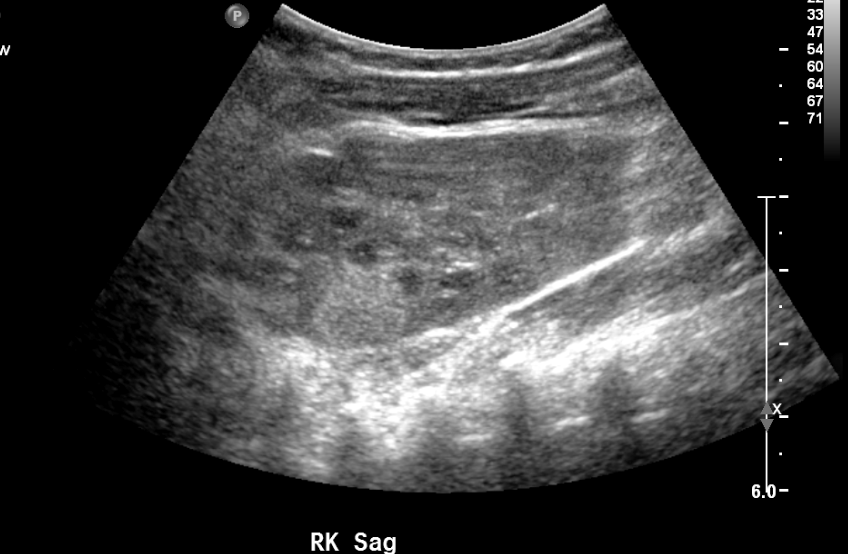
Figura 10 Massa renal ecogênica na ultrassonografia de rastreio em paciente com síndrome de WAGR.
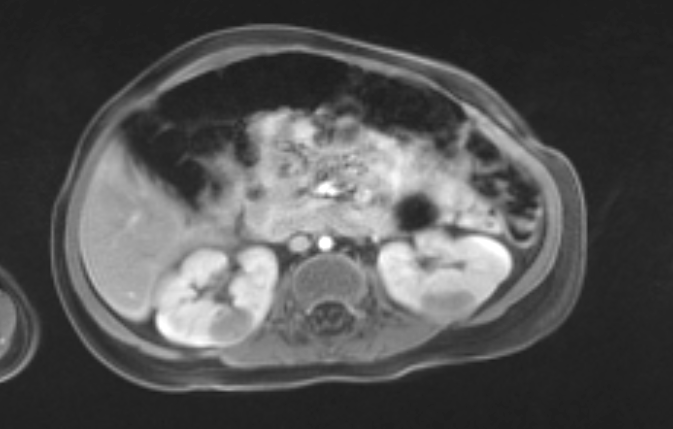
Figura 11 A RM confirmou múltiplas massas (mesmo paciente da Figura 10).
Fluxo Sanguíneo Renal
A ultrassonografia fornece informações valiosas em casos de suspeita de estenose da artéria renal.
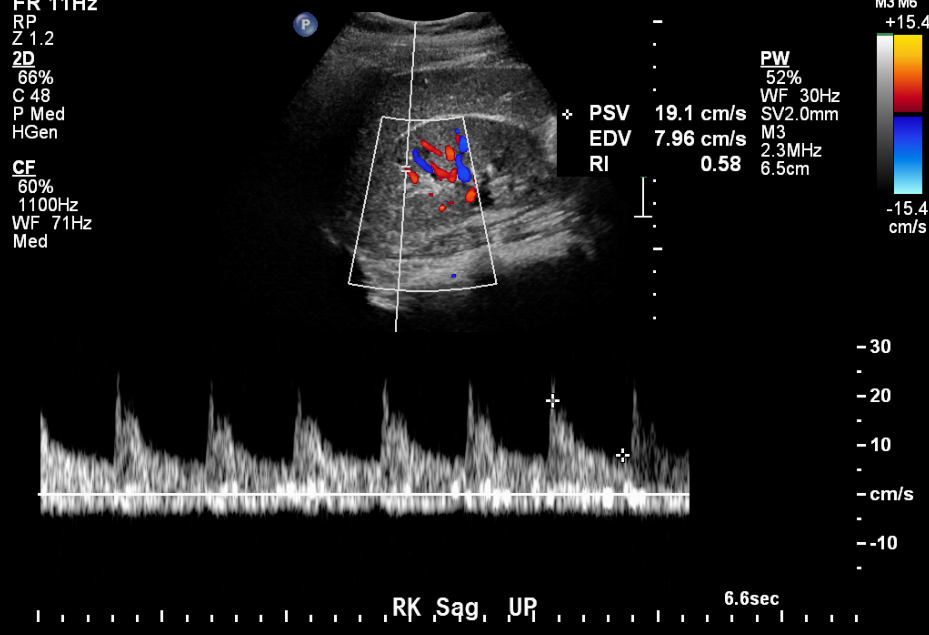
Figura 12 Traçado arterial normal em uma criança de 11 anos com hipertensão.
Cálculos renais
Cálculos obstrutivos podem ser visualizados diretamente por ultrassonografia ou podem ser inferidos pela presença de um sistema coletor dilatado no lado sintomático. O artefato de cintilação pode ser utilizado para detectar cálculos.

Figura 13 Cálculo no polo inferior do rim direito.
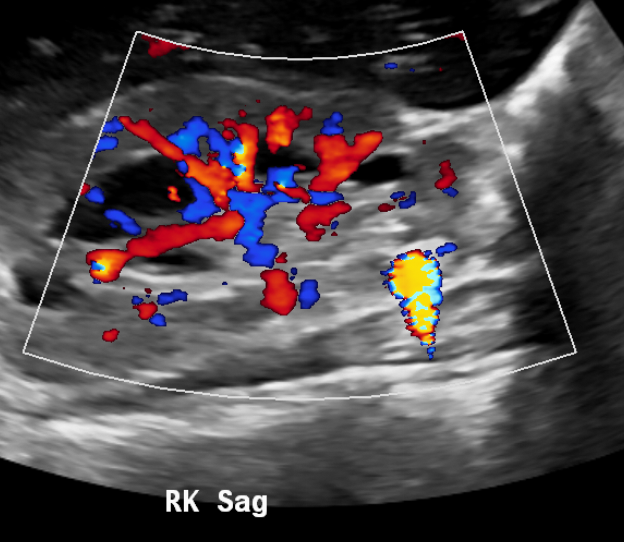
Figura 14 O artefato twinkling melhora a conspicuidade dos cálculos.
Anomalias da Bexiga
Uma bexiga adequadamente distendida pode ser avaliada quanto a espessamento da parede, trabeculação, detritos ou cálculos. Massas vesicais podem ser encontradas incidentalmente. Imagens pós-miccionais são úteis em pacientes com suspeita de disfunção miccional.
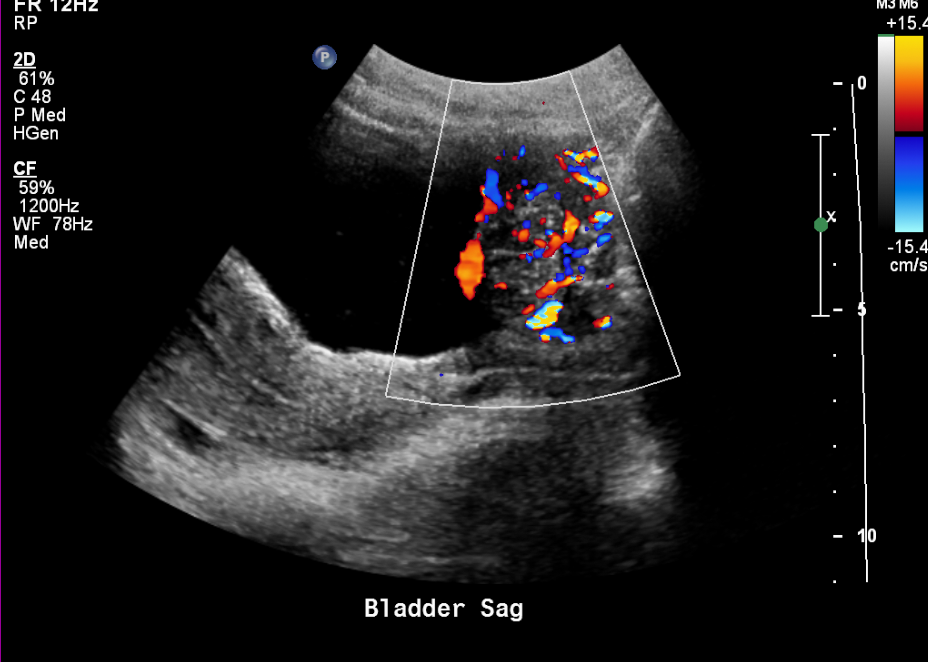
Figura 15 Massa vesical altamente vascularizada em um adolescente.
Técnica:
- Bexiga cheia (em criança treinada para o toalete).
- Bexiga examinada primeiro, antes do restante do abdome, para evitar esvaziamento precoce da bexiga.
- Cortes sagitais dos rins; melhores para medida do comprimento. Idealmente, o ultrassonografista deve revisar ultrassonografias prévias para ter uma noção do comprimento renal esperado.
- Corte transversal nos polos superior, interpolar e inferior; melhor para dilatação do sistema coletor intrarrenal. Uma pelve extrarrenal visualizada no plano sagital pode mimetizar leve dilatação do sistema coletor intrarrenal.
Ultrassonografia escrotal
A ultrassonografia é a modalidade de escolha para avaliar o escroto no contexto de dor ou anormalidade palpável.12
Técnica:
- Imagens dos testículos na maior dimensão em dois planos, com medidas
- Imagens da cabeça do epidídimo (meninos mais velhos), com medidas
- Doppler colorido mostrando ambos os testículos
- Doppler espectral mostrando fluxo arterial em ambos os testículos
- Vistas dos cordões espermáticos (idealmente clipes com movimento)
- Documentar hidrocele ou varicocele, caso presentes

Figura 16 Hidroceles bilaterais em um recém-nascido

Figura 17 Hidrocele não comunicante em recém-nascido

Figura 18 Hérnia inguinal em um neonato
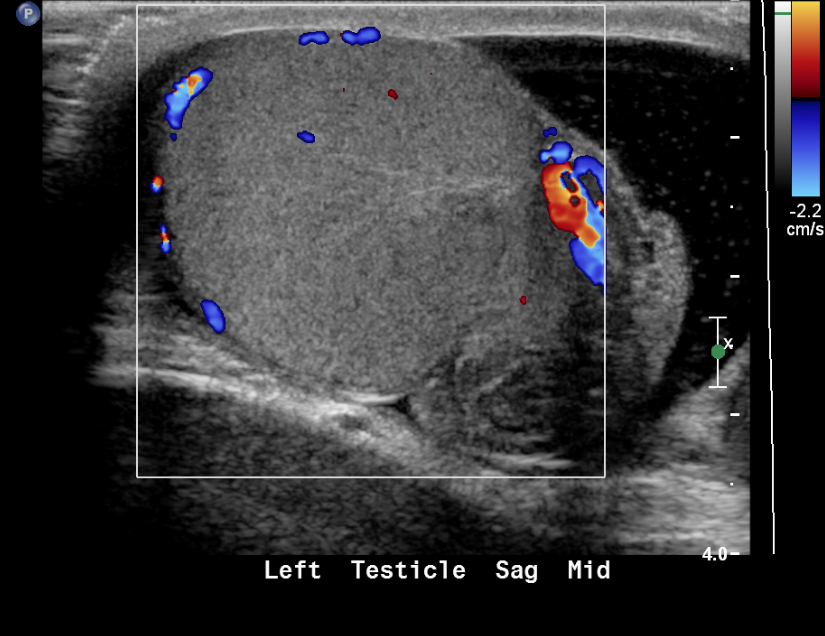
Figura 19 Testículo torcido com ausência de fluxo colorido
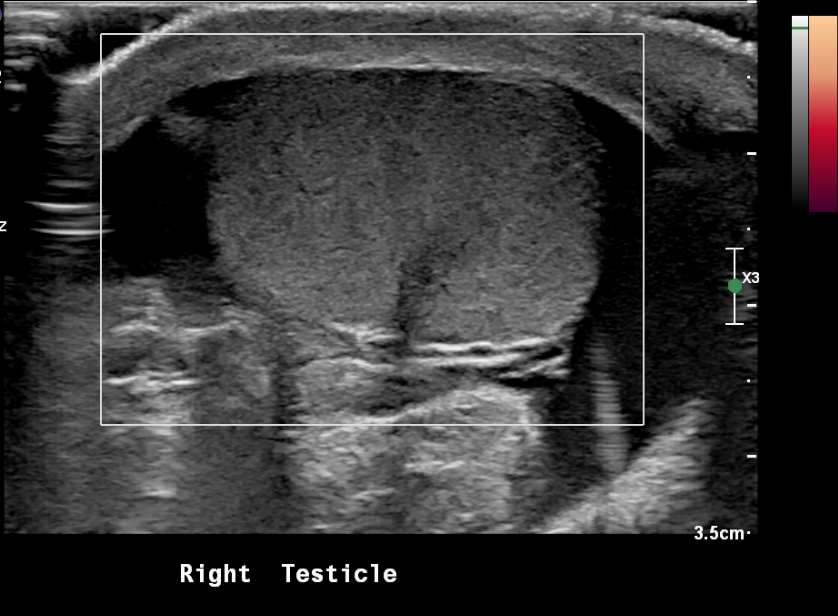
Figura 20 Testículo torcido com ausência de fluxo sanguíneo no power Doppler
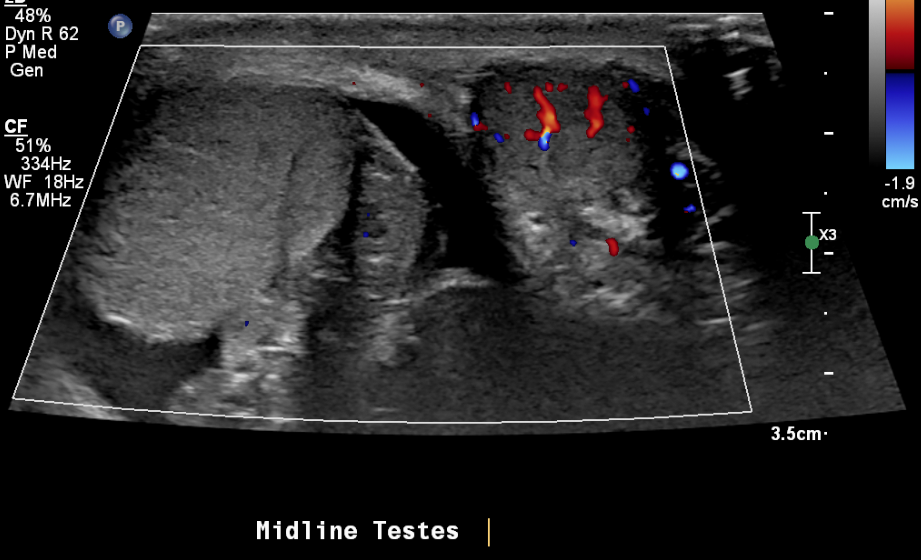
Figura 21 Testículo direito torcido e fluxo sanguíneo normal no testículo esquerdo

Figura 22 Rabdomiossarcoma paratesticular em um adolescente com massa palpável indolor
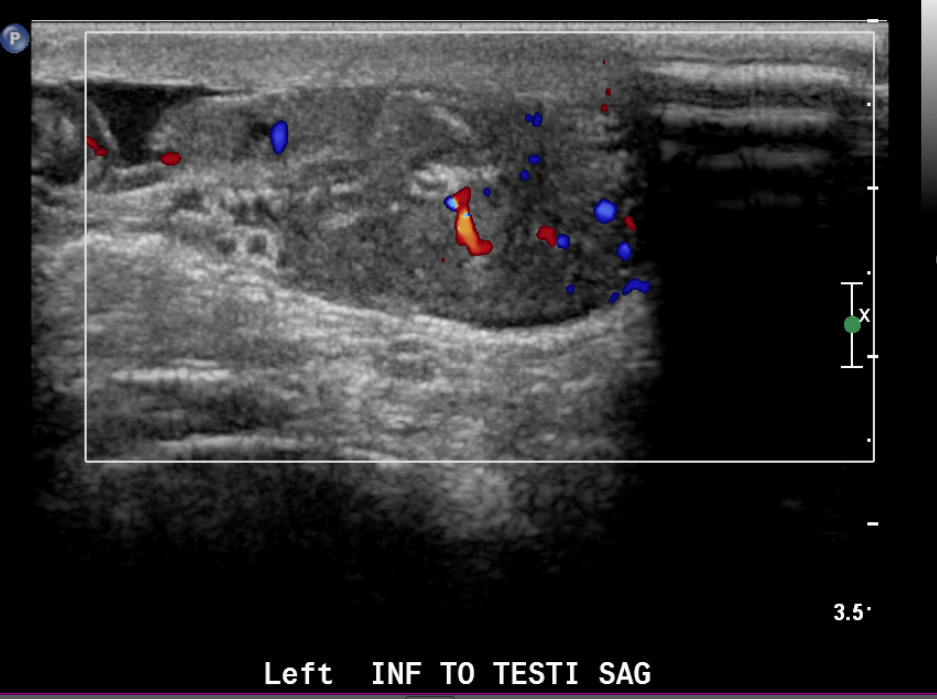
Figura 23 Imagem colorida de rabdomiossarcoma paratesticular
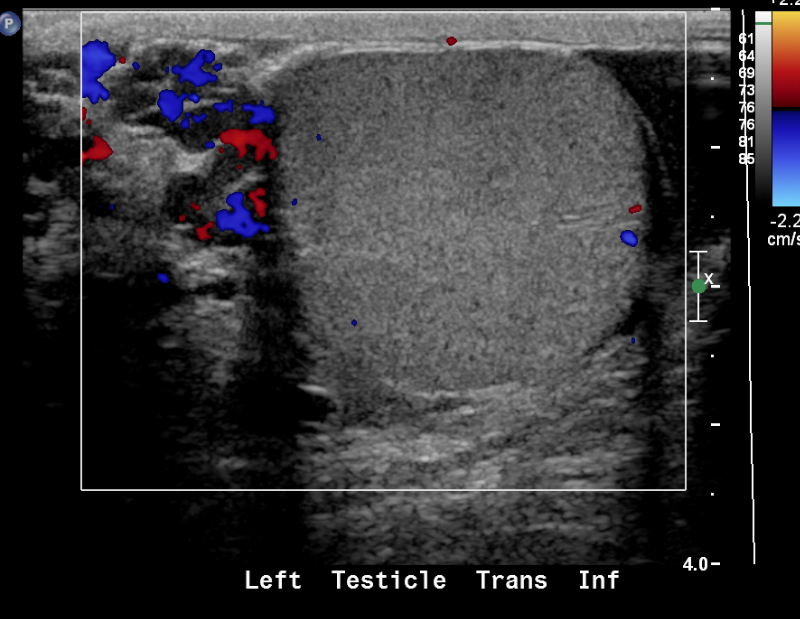
Figura 24 Varicocele
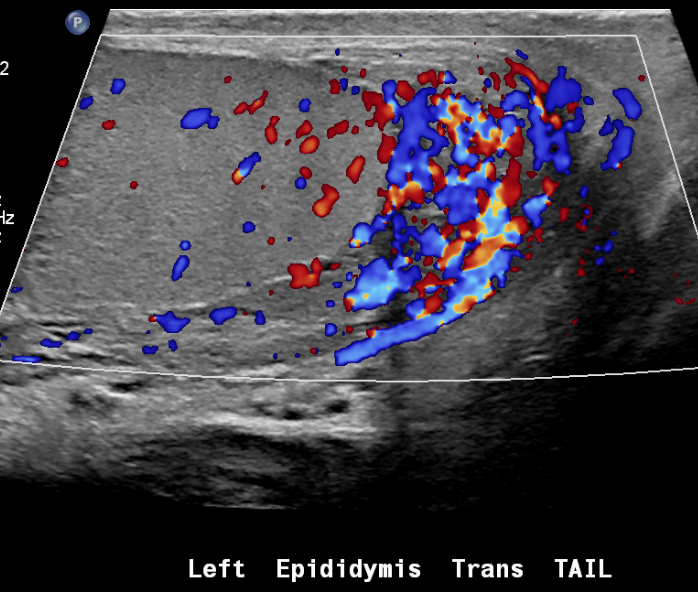
Figura 25 Epididimite
Radiografia
Radiografias utilizam a diferença de densidade radiográfica das várias partes do corpo para criar uma imagem (ar, gordura, líquido, osso e metal). Radiografias modernas são armazenadas usando um sistema de arquivamento e comunicação de imagens (PACS), que é um sistema de imagens digitais. As vantagens do PACS incluem melhor resolução das imagens e a capacidade de compartilhar o acesso de forma instantânea e remota.
As radiografias abdominais são frequentemente obtidas no contexto agudo (dor abdominal aguda) para avaliar o padrão de gás intestinal e excluir ar livre (geralmente são necessárias duas incidências para este último).
Outros achados potenciais:
- Calcificações de partes moles
- Massas abdominais volumosas
- Organomegalia
- Anomalias ósseas
- Posicionamento de dispositivos de suporte (p. ex., stents ureterais)
Uma única radiografia abdominal em decúbito dorsal também é comumente solicitada por urologistas pediátricos no contexto ambulatorial para constipação intestinal conhecida ou suspeita. Por consenso de especialistas, isso não está indicado em crianças com grande quantidade de fezes ao exame retal.13 Pode haver indicação para essa prática em casos em que o exame retal não é possível (como em um histórico de trauma). O profissional deve lembrar que radiografias abdominais podem resultar em uma carga de radiação não desprezível ao longo do tempo.
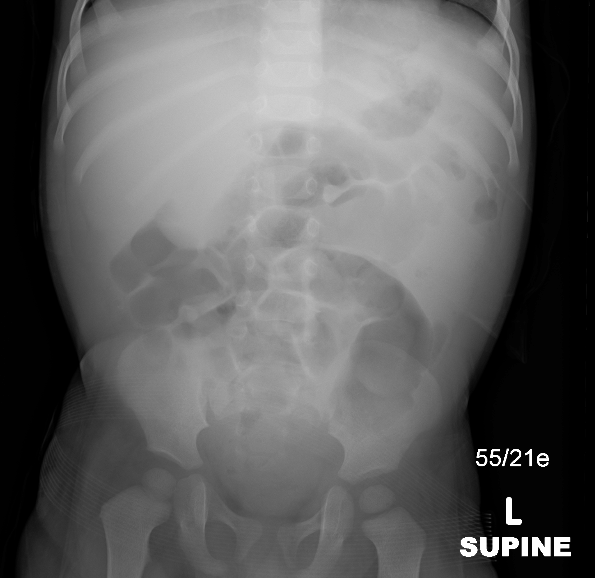
Figura 26 Radiografia abdominal mostrando efeito de massa no quadrante superior direito
Cistouretrografia Miccional e Urosonografia Miccional
VCUG é um procedimento de radiologia especializado usado principalmente para avaliar a presença de refluxo vesicoureteral (RVU) e para avaliar a morfologia uretral. A justificativa tem sido a suposta ligação entre o refluxo e as cicatrizes pós-infecciosas. Apesar de trinta anos de estudo desde o início da profilaxia antibiótica rotineira para o refluxo, permanecem dúvidas. Cistografias são realizadas com menos frequência do que no passado, e a conduta expectante é frequentemente preferida à profilaxia antibiótica.14 Estudos miccionais tradicionalmente têm sido realizados com fluoroscopia. Está em curso, nos Estados Unidos, uma transição para o uso de ultrassonografia com contraste (ceUS). Na Europa, a ultrassonografia com contraste é realizada desde a década de 1990 e está amplamente disponível desde o início dos anos 2000. No entanto, os agentes de contraste para ultrassonografia não foram aprovados para uso nos EUA até 2016. Permanece debate quanto à sensibilidade da ceVUS para anomalias uretrais no lactente do sexo masculino. À época desta redação, os critérios de adequação do ACR ainda recomendam VCUG em vez de ceVUS nesse contexto, apesar da existência de artigos de revisão mostrando excelente representação da anatomia uretral pela ceVUS.8,15,16
Fluoroscopia ainda é frequentemente utilizada, inclusive na instituição deste autor, apesar de expor o paciente à radiação ionizante. Outra desvantagem da fluoroscopia tradicional é que exige que o paciente permaneça deitado em posição supina para urinar; isso frequentemente é difícil para pacientes treinados para o toalete.
A cateterização vesical asséptica é necessária para ambos os tipos de exame e é frequentemente a parte mais difícil do exame para o paciente. Uma pequena sonda de alimentação (5 Fr a 10 Fr, dependendo do tamanho e da idade do paciente) é introduzida pela uretra até a bexiga. O uso de sedação em crianças entre aproximadamente dois e seis anos de idade é controverso. Os riscos potenciais da sedação devem ser ponderados em relação ao dano causado pelo estresse psicológico. O uso de uma prancha octogonal ou similar para imobilizar o paciente também é controverso. Alguns radiologistas pediátricos preferem usar a prancha em lactentes mais velhos ou crianças pequenas. Um profissional de Child Life é um recurso valioso durante esses exames e pode ser uma presença reconfortante tanto para o paciente quanto para o pai ou a mãe que o acompanha.
Uma vez que o cateter esteja posicionado e a bexiga esvaziada, o material de contraste é instilado sob observação fluoroscópica (ou ultrassonográfica). O exame ultrassonográfico pode usar um manguito de pressão arterial para infundir o contraste com pressão leve. Para a VCUG, o contraste é instilado por gravidade. As imagens padrão obtidas tanto na VCUG quanto na ceVUS são essencialmente as mesmas.
Técnica de VCUG:
- Imagem spot fluoroscópica do abdômen (lactente) ou ao nível dos rins e ao nível da bexiga (criança maior)
- Imagem spot ou retenção da última imagem da bexiga no enchimento inicial (avaliação de ureterocele)
- Verificações intermitentes para avaliar refluxo
- Próximo da capacidade vesical prevista, obter imagens oblíquas bilaterais com retenção da última imagem ou spots
- Na primeira micção, verificar presença de refluxo
- Segundo ciclo (pelo menos) em lactente ou em paciente com infecção do trato urinário febril
- Projeção lateral da uretra durante a micção em paciente do sexo masculino (idealmente com o cateter retirado)
As imagens padrão da urosonografia miccional serão, em sua maioria, semelhantes, com exceção da vista de reconhecimento inicial. Vistas panorâmicas podem auxiliar na ampliação do campo de visão na ultrassonografia. No entanto, o campo de visão reduzido permanece uma limitação da ultrassonografia.
Deve-se tomar cuidado para encher a bexiga adequadamente e não a superencher. Uma fórmula útil para a capacidade vesical (para crianças com mais de 12 meses) é idade mais 2 multiplicado por 30 para a capacidade vesical prevista (em mL). Espera-se que um recém-nascido retenha cerca de 50 mL. Devem ser obtidas imagens pontuais fluoroscópicas oblíquas ou, pelo menos, retenções da última imagem com distensão vesical máxima para avaliar refluxo de baixo grau (que pode ser obscurecido na projeção AP). Dar leves toques sobre a bexiga, massagem suave sobre o abdome ou água morna borrifada na pele pode ajudar a induzir crianças pequenas a urinar. A sedação pode, ocasionalmente, dificultar a micção para os pacientes. O superenchimento (superior ao dobro da capacidade prevista) deve ser evitado, pois pode tornar esse problema mais provável.
- Indicações
- Refluxo vesicoureteral
- Estudo da uretra durante a micção
- Anomalias vesicais
- Contraindicações
- Infecção do trato urinário aguda
- Reação prévia grave ao contraste
- Preparação do paciente
- O paciente deve urinar antes do exame (crianças pequenas podem ter a bexiga drenada antes do enchimento).
- Cobertura antibiótica com Trimetoprima 2 mg/kg/dose uma vez ao dia por 3 dias antes do exame (em crianças que não estejam em antibiótico profilático)
- Nota do editor: A evidência para isto é limitada e a prática não é universal.
- Complicações
- Reações relacionadas ao contraste
- Infecção do trato urinário
- Sobredistensão e ruptura da bexiga
- Lesão por cateter
- Achados
- Grau I – refluxo para ureter não dilatado
- Grau II – refluxo para a pelve renal e cálices sem dilatação
- Grau III – dilatação leve/moderada do ureter, pelve renal e cálices com mínimo apagamento dos fórnices
- Grau IV – dilatação da pelve renal e dos cálices com tortuosidade ureteral moderada
- Grau V – dilatação acentuada do ureter, pelve e cálices; tortuosidade ureteral; perda das impressões papilares
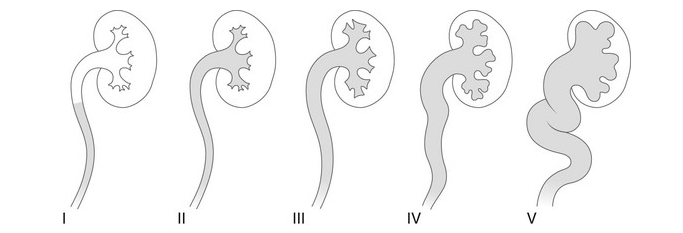
Figura 27 Classificação radiológica do refluxo vesicoureteral

Figura 28 Ureterocele na retenção da última imagem fluoroscópica

Figura 29 Refluxo de grau 3 para ambos os rins
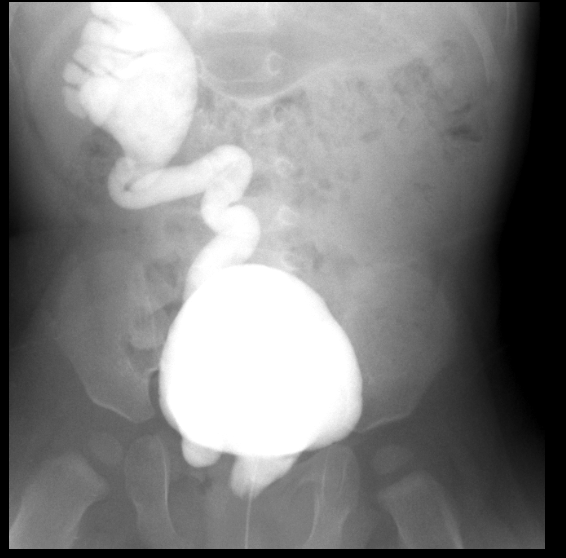
Figura 30 Refluxo grau 5 à direita com inserção ectópica na uretra
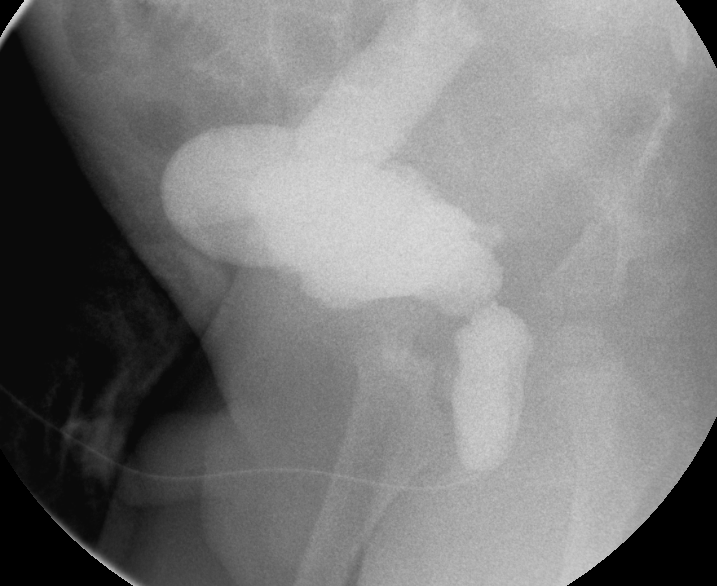
Figura 31 Uretra posterior dilatada e ureter direito marcadamente dilatado no contexto de válvulas uretrais posteriores
Estudos com radionuclídeos
DMSA / Cintilografia Renal Estática
O ácido dimercaptossuccínico (DMSA) liga-se às proteínas plasmáticas e é retido pelo córtex renal durante a depuração renal, permitindo a avaliação funcional. Dados quantitativos sobre a função renal são informações cruciais que não podem ser obtidas por ultrassonografia. A cintilografia com ácido dimercaptossuccínico (DMSA) com Tc99m tem sido considerada o exame de escolha na avaliação de dano parenquimatoso devido à pielonefrite aguda ou crônica e fornece dados sobre a função renal diferencial. Não é necessário cateter vesical para a cintilografia com DMSA, pois o radiofármaco não é excretado na urina. O SPECT com DMSA aumenta a sensibilidade, mas é necessária sedação em crianças pequenas para obter imagens de alta qualidade.17 O DMSA não fornece informações sobre o sistema coletor ou urodinâmica.
- Indicações
- Avaliar a função renal
- Investigação de infecção renal
- Anomalias renais congênitas (por exemplo, rins em ferradura)
- Cicatrizes renais e lesões renais
- Contraindicações
- Nenhuma
- Técnica
- DMSA injetado por via intravenosa e imagens obtidas por uma câmara gama 1–6 horas depois.
- Informações obtidas
- Função renal relativa
- Captação absoluta
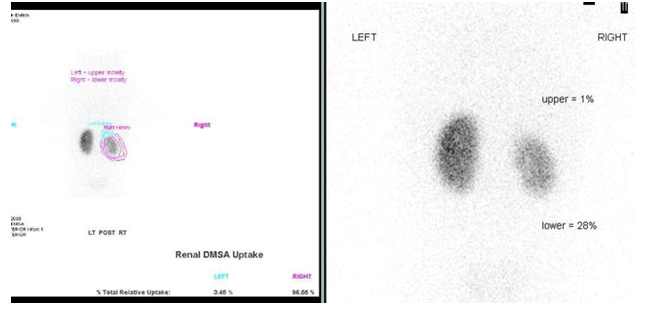
Figura 32 Cintilografia renal com DMSA mostrando cicatrizes e função reduzida do hemi-rim inferior direito de um rim duplicado e do hemi-rim superior não funcionante
Exame MAG-3 / Cintilografia Renal Dinâmica
Mercaptoacetiltriglicina (MAG-3) é fortemente ligada a proteínas plasmáticas, portanto é depurada por secreção tubular. A cintilografia dinâmica com MAG-3 fornece informações sobre a função e a morfologia renais. É necessária sedação para crianças pequenas (com menos de cerca de 5 anos de idade). A parte inicial do estudo demonstra a perfusão e a função cortical renal, permitindo distinguir entre lesões reversíveis e irreversíveis. O sistema coletor e a urodinâmica são então caracterizados com o auxílio de furosemida. Uma cintilografia com MAG-3 tranquilizadora permite ao urologista pediátrico observar com segurança um paciente com hidronefrose na maioria dos casos.18
- Indicações
- Sistema obstruído vs não obstruído
- Estenose da artéria renal
- Doença do refluxo
- Trauma renal
- Contraindicações
- Nenhuma
- Técnica
- Hidratar o paciente e esvaziar a bexiga
- Colocação de cateter vesical
- Injeção de MAG-3
- Imagem aos 2–3 minutos com uma câmara gama para a fase parenquimatosa
- Imagem a partir de 18–20 minutos
- Furosemida 1 mg/kg, máximo 40 mg, injeção quando a pelve renal dilatada estiver cheia
- Imagem sequencial por aproximadamente 20 minutos adicionais
- Regiões de interesse desenhadas ao redor dos rins
- Curvas de washout geradas e t½ (tempo para metade do radiofármaco ser eliminado) calculado
- Informações obtidas
- Perfusão renal
- Perfusão cortical (função renal diferencial)
- Tempos de trânsito do parênquima e do rim como um todo
- T½ menor que 10 minutos é normal
- T½ entre 10 e 20 minutos é indeterminado
- T½ maior que 20 minutos sugere obstrução
- Armadilhas
- Desidratação causando resposta diurética inadequada
- Função renal subjacente reduzida causando resposta diurética inadequada
- Bexiga distendida ou não complacente (colocar cateter)
- Refluxo de alto grau precoce (VCUG/ VUS prévios)
- Sistema coletor patuloso atrasando o washout
- Regiões de interesse incluindo baço ou fígado
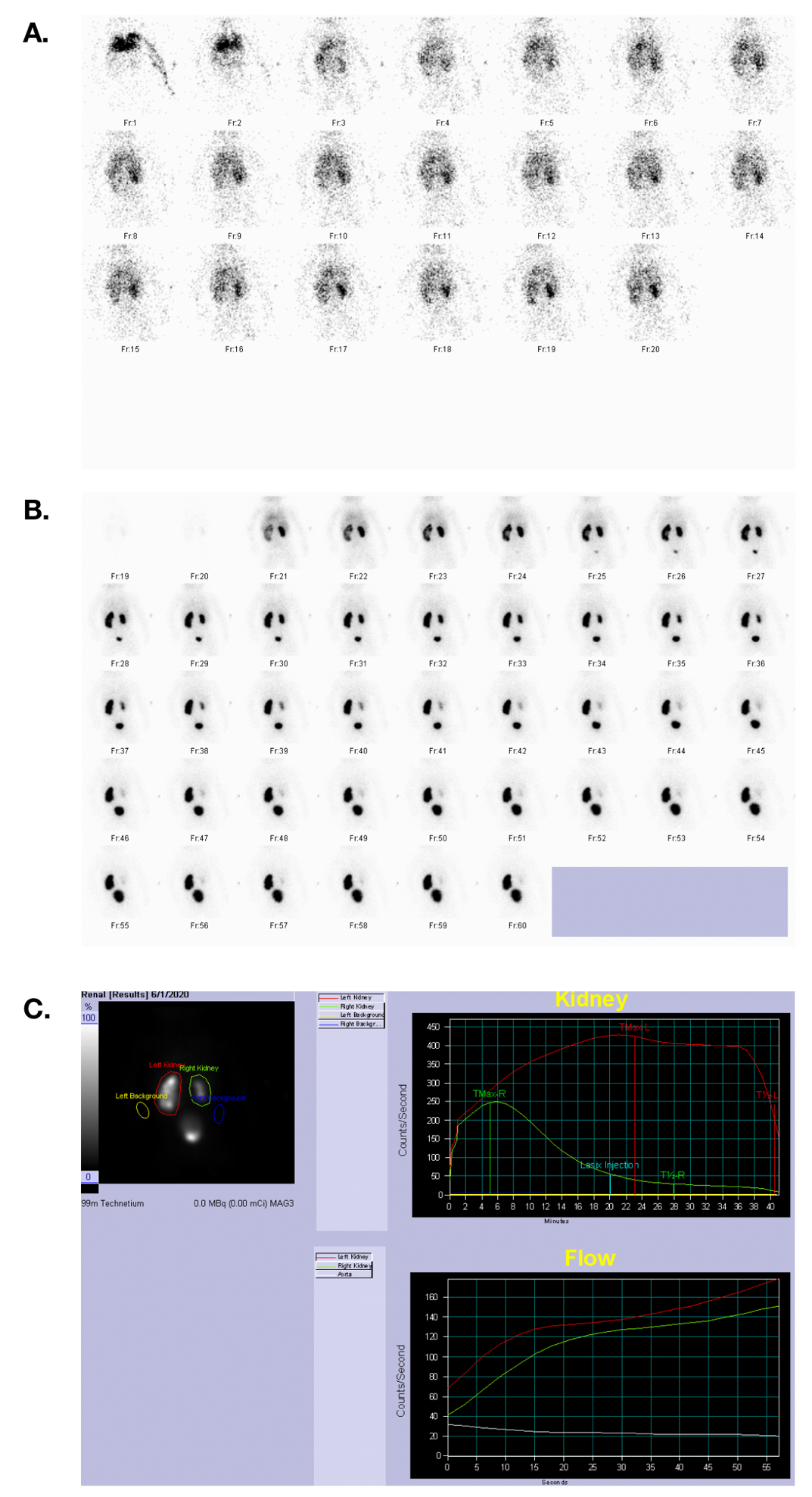
Figura 33 Cintilografia com MAG 3 mostrando fluxo sanguíneo, fase excretora e curvas tempo-atividade em um paciente com função renal simétrica e obstrução da JUP à esquerda.
Tomografia Computadorizada
A TC com contraste IV é o padrão de cuidado em crianças para avaliação de trauma abdominal contuso. É rápida, amplamente disponível e permite monitorização pelo radiologista em tempo real. Idealmente, se for identificada uma lesão do sistema coletor renal, podem ser obtidas imagens tardias adicionais direcionadas aos rins ou à bexiga (dependendo do nível anatômico da lesão suspeita). Com raras exceções, este é o único uso apropriado de TC multifásica na população pediátrica. Nos Estados Unidos, a RM substituiu em grande parte a TC para o estadiamento tumoral do abdome e da pelve pediátricos.
TC sem contraste pode ocasionalmente ser útil no contexto pediátrico para o acompanhamento de cálculos renais e ureterais, ou para o diagnóstico quando a ultrassonografia não é elucidativa.2 A ultrassonografia pode não revelar o cálculo obstrutivo, especialmente se ele estiver no terço médio do ureter (onde o gás intestinal que causa sombra acústica frequentemente bloqueia o feixe ultrassônico). No entanto, a presença de um sistema coletor dilatado no lado sintomático pode permitir ao clínico inferir que há um cálculo. Em crianças com cálculos conhecidos ou condições que predispõem à formação de cálculos, pode ser desejável a realização de TC. Podem ser empregadas doses muito baixas de radiação para avaliar a carga litiásica ou para o acompanhamento após intervenção para cálculos.19 Protocolos para hematúria (TC trifásica com fases sem contraste, com contraste e tardia) não são apropriados para crianças devido à elevada carga de radiação.2
Nos Estados Unidos, a RM substituiu em grande parte a TC para o estadiamento tumoral do abdome e da pelve pediátricos.20 No entanto, a angiografia por TC é ocasionalmente solicitada por nossos cirurgiões pediátricos para fins de planejamento. A CTA mostra as relações entre órgãos e a anatomia vascular com menos artefatos e maior resolução do que a RM, permitindo ao cirurgião planejar uma abordagem mais precisa em casos de tumor de Wilms, neuroblastoma ou outras neoplasias malignas. Como a angiografia por TC requer uma injeção de contraste mais rápida e acarreta uma carga de radiação mais elevada, esses exames devem ser monitorados ativamente por um radiologista pediátrico.
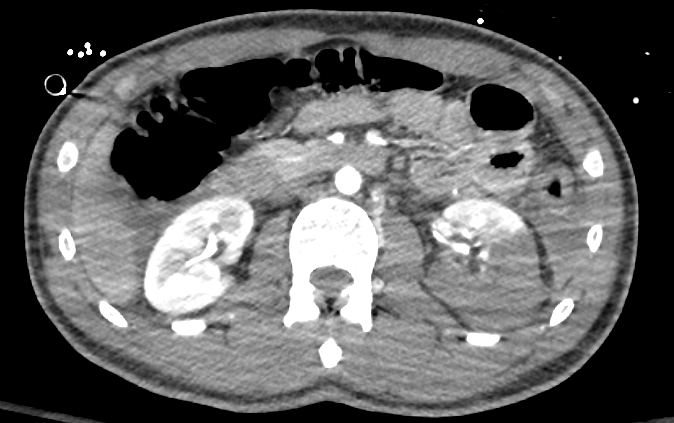
Figura 34 TC com contraste mostrando laceração renal de alto grau do rim esquerdo.

Figura 35 A imagem tardia através do rim descarta ruptura do sistema coletor.

Figura 36 Estudo de cálculos por TC em paciente com cistinúria; note-se stents bilaterais parcialmente visíveis.

Figura 37 Angiotomografia computadorizada com reconstrução 3D em paciente oncológico com anatomia arterial complexa; três artérias renais são mapeadas para cada hemirrim
RM
A RM explora as propriedades magnéticas do núcleo do hidrogênio para produzir informações matemáticas sobre os tecidos moles do corpo humano, que podem então ser transformadas em uma imagem detalhada. Ela é superior a qualquer outra modalidade para contraste de tecidos moles e não utiliza radiação ionizante. Essas vantagens a tornaram a modalidade de escolha para a maior parte do estadiamento do câncer no abdome e na pelve. Numerosas sequências de pulso de RM estão comercialmente disponíveis. Assim, a RM é adaptada à questão clínica (mais do que a TC), exigindo protocolos específicos.
A resolução da RM permanece inferior à da TC (sendo cerca de uma ordem de magnitude inferior à da TC nesse aspecto), e a avaliação do tecido pulmonar ainda é limitada no contexto clínico. Além disso, a RM é demorada e ruidosa, exigindo alguma forma de sedação na maioria das crianças com menos de cerca de oito anos de idade. Enquanto os pacientes adultos (geralmente) conseguem seguir instruções de apneia (prender a respiração), isso é difícil ou impossível para crianças pequenas. Software que permita aquisição durante respiração livre é essencial para a RM do corpo em crianças.21 Essas sequências tipicamente demoram mais do que uma sequência com apneia, mas ainda assim podem ser adquiridas de forma relativamente rápida (em aproximadamente três minutos). A duração de um exame de RM pode variar de trinta minutos a mais de uma hora, dependendo do protocolo específico.
A avaliação do trato urinário é chamada de urografia por ressonância magnética (MRU). A MRU é capaz de fornecer informações anatômicas e funcionais com um único exame.8 A MRU correlaciona-se bem com a cintilografia renal com Lasix na avaliação da função renal. Os pacientes são hidratados com soro fisiológico (aproximadamente 10 mL/kg) e o Lasix é administrado no início do exame, na dose de 1 mg/kg até um máximo de 20 mg. Nos casos de suspeita de obstrução da junção ureteropélvica, pode ser útil obter imagens do paciente em decúbito ventral ou sobre o lado contralateral à obstrução suspeita. Em pacientes sedados, pode-se colocar um cateter de Foley.8 A MRU para pacientes sedados é um empreendimento cooperativo que exige boa comunicação entre o urologista, a equipe de radiologia e a equipe de sedação ou anestesia.
A angiografia por RM evita expor o paciente à radiação, mas tem menor resolução e é mais suscetível a artefatos do que a CTA.
No diagnóstico fetal, a RM é uma modalidade complementar à ultrassonografia. Sequências rápidas de pulso são essenciais para a obtenção de imagens fetais. Embora a RM fetal seja solicitada com mais frequência para avaliação adicional de uma anomalia cerebral, ela também pode fornecer informações adicionais sobre o trato urinário fetal. Pode ser especialmente útil no contexto do planejamento cirúrgico de anomalias urogenitais complexas.22 Em geral, a qualidade da imagem na RM fetal melhora nas fases mais avançadas da gestação.
- Indicações de RM em pediatria
- Estadiamento de cânceres
- Suspeita de massa renal
- Rastreamento de pacientes com risco de tumor (por exemplo, TS, VHL)
- Pode ser apropriada para pielonefrite complicada
- Urografia por RM
- Método
- Urografia sensível a fluidos usando técnicas de RM fortemente ponderadas em T2
- Urografia excretora por RM usando imagens ponderadas em T1 com contraste e furosemida
- Indicações
- Anatomia do sistema coletor
- Determinar o nível de obstrução nas vias renais (intrínseca e extrínseca)
- Anomalias congênitas
- Método

Figura 38 Imagem de RM sensível a líquido com supressão de gordura mostrando polo superior esquerdo dilatado em um rim duplicado.
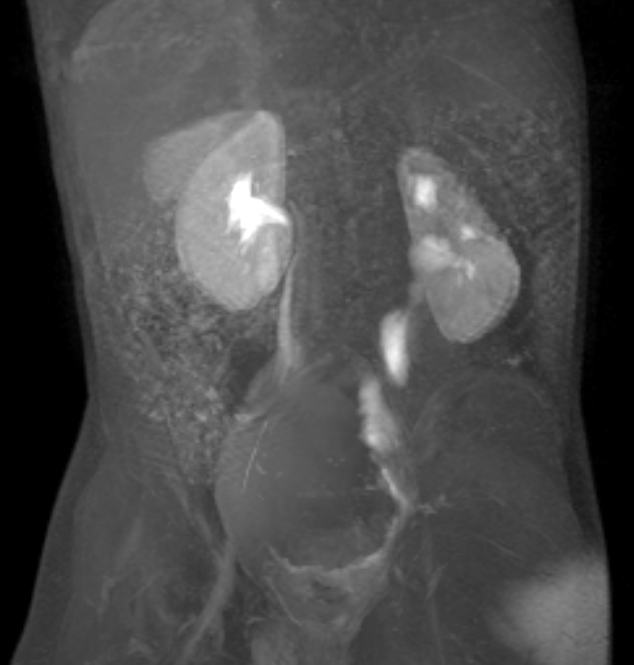
Figura 39 Imagem de RM dinâmica pós-contraste mostra um megauréter esquerdo dilatado, porém não obstruído.
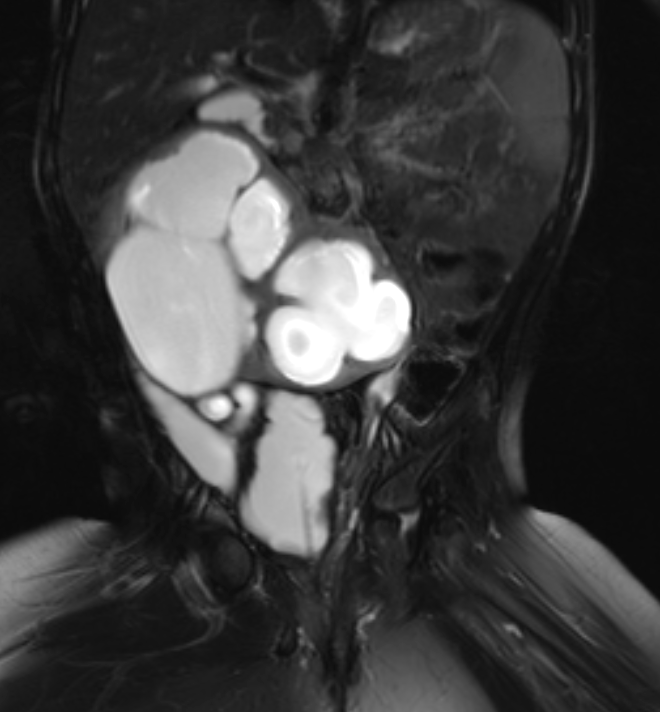
Figura 40 Imagem de RM sensível ao líquido com supressão de gordura mostra um rim em ferradura hidronefrótico e uma morfologia de bexiga neurogênica.

Figura 41 Série dinâmica de RM pós-contraste confirma obstrução do rim em ferradura.

Figura 42 Imagem de RM sensível a fluidos com supressão de gordura mostra um rim esquerdo pequeno e displásico.
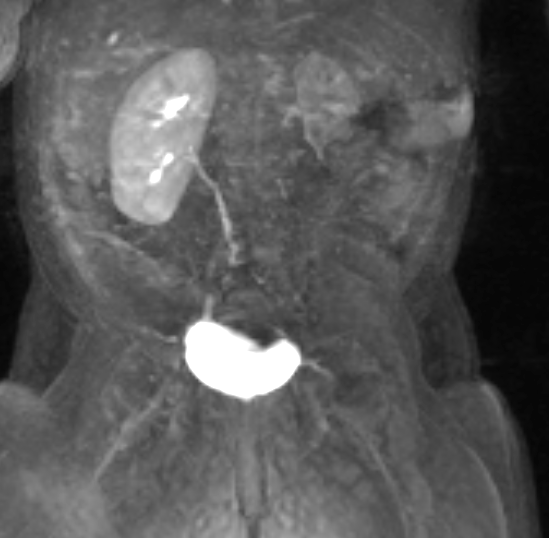
Figura 43 Série dinâmica de RM pós-contraste mostra realce tardio e mínimo do rim displásico, indicando função limitada.

Figura 44 Série dinâmica de RM pós-contraste mostra rim direito pequeno em um paciente com síndrome de prune-belly e refluxo vesicoureteral bilateral.
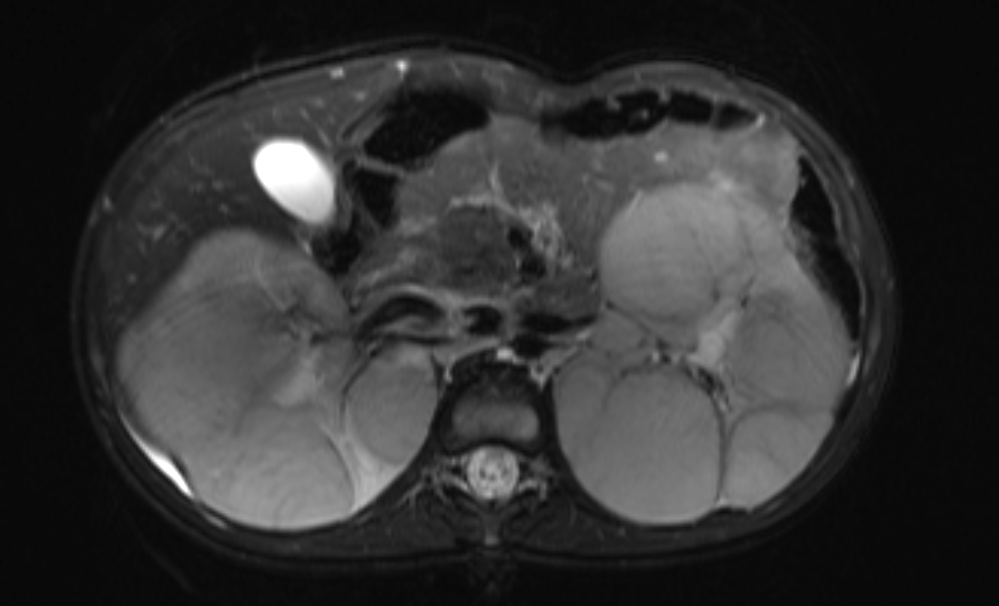
Figura 45 Imagem de RM sensível a líquido com supressão de gordura mostrando substituição do parênquima renal por múltiplas massas em um paciente com nefroblastomatose.
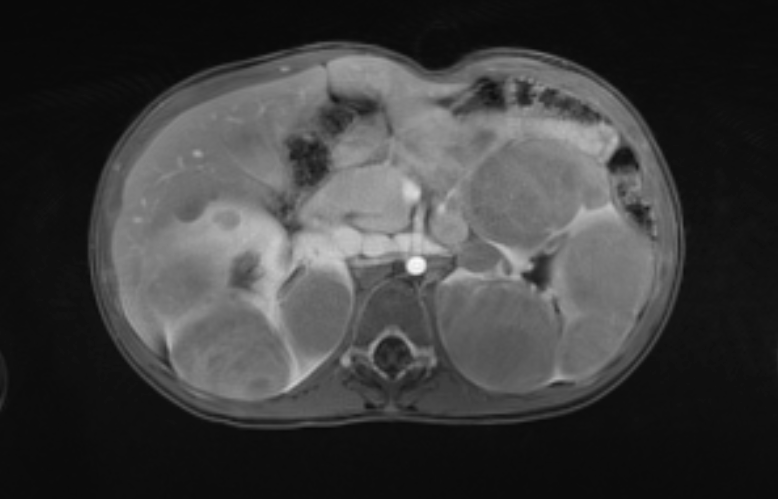
Figura 46 As imagens de RM pós-contraste mostram as características de realce das massas.
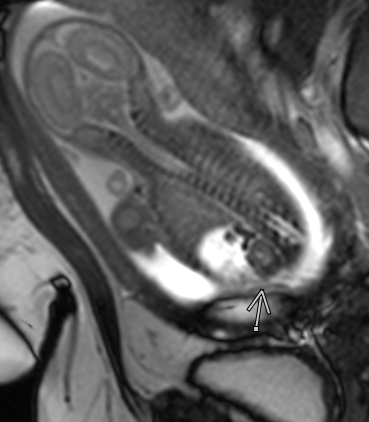
Figura 47 Vista de um rim e de uma glândula suprarrenal normais em um feto com ascite
Intervenção em Urologia Pediátrica
Procedimentos intervencionistas são parte integrante do manejo de condições urológicas pediátricas.23,24 A subespecialidade de radiologia pediátrica é distinta tanto da radiologia pediátrica quanto da radiologia intervencionista do adulto, e os profissionais de RI pediátrica permanecem em número reduzido, apesar do crescimento ao longo dos últimos quinze anos.25
Drenagem das vias urinárias secundária à obstrução/nefrostomias
- Deve ser reservado para pacientes em que a abordagem de drenagem retrógrada não é possível
- A preparação pré-procedimento incluiria a avaliação do risco de sangramento e infecção
- Profilaxia antibiótica
- Acesso ao sistema coletor renal sob orientação de ultrassom, fluoroscopia ou tomografia computadorizada.
- Complicações
- Hemorragia
- Sepse
- Lesão de órgãos
- Lesão torácica (isto é, pneumotórax)
Nefrolitotomia percutânea
- Reservado para pacientes que não são candidatos à ureteroscopia ou à litotripsia por ondas de choque
- Procedimento em duas etapas
- Acesso ao sistema coletor pelo radiologista usando ultrassonografia/fluoroscopia
- Remoção do cálculo pelo urologista
Outras Intervenções
- Colocação de stent ureteral
- Dilatação ureteral secundária a estenose
- Biópsia de tumores renais
- Embolização de tumores renais ou hemorragia renal
Leituras recomendadas
- Brown BP, Simoneaux SF, Dillman JR, Rigsby CK, Iyer RS, Alazraki AL, et al.. ACR Appropriateness Criteria® Antenatal Hydronephrosis–Infant. J Am Coll Radiol 2020; 17 (11): S367–s379. DOI: 10.1016/j.jacr.2020.09.017.
- Chung EM, Soderlund KA, Fagen KE. Imaging of the Pediatric Urinary System. Radiol Clin North Am 2017; 55 (2): 337–357. DOI: 10.1016/j.rcl.2016.10.010.
- Dillman JR, Rigsby CK, Iyer RS, Alazraki AL, Anupindi SA, Brown BP, et al.. ACR Appropriateness Criteria® Hematuria-Child. J Am Coll Radiol 2018; 15 (5): S91–s103. DOI: 10.1016/j.jacr.2018.03.022.
- Dillman JR, Trout AT, Smith EA. MR urography in children and adolescents: techniques and clinical applications. Abdom Radiol (NY) 2016; 41 (6): 1007–1019. DOI: 10.1007/s00261-016-0669-z.
- Duran C, Beltrán VP, González A, Gómez C, Riego Jdel. Contrast-enhanced Voiding Urosonography for Vesicoureteral Reflux Diagnosis in Children. Radiographics 2017; 37 (6): 1854–1869. DOI: 10.1148/rg.2017170024.
- Chow JS, Koning JL, Back SJ, Nguyen HT, Phelps A, Darge K. Classification of pediatric urinary tract dilation: the new language. Pediatric Radiology 2017; 47: 1109–1115.
Referências
- Strauss KJ, Goske MJ, Kaste SC, Bulas D, Frush DP, Butler P, et al.. Image Gently: Ten Steps You Can Take to Optimize Image Quality and Lower CT Dose for Pediatric Patients. AJR Am J Roentgenol 1976; 194 (4): 868–873. DOI: 10.2214/ajr.09.4091.
- Dillman JR, Rigsby CK, Iyer RS, Alazraki AL, Anupindi SA, Brown BP, et al.. ACR Appropriateness Criteria® Hematuria-Child. J Am Coll Radiol 2018; 15 (5): S91–s103. DOI: 10.1016/j.jacr.2018.03.022.
- Goodman TR, Mustafa A, Rowe E. Pediatric CT radiation exposure: where we were, and where we are now. Pediatr Radiol 2019; 49 (4): 469–478. DOI: 10.1007/s00247-018-4281-y.
- Kuebker J, Shuman J, Hsi RS, Herrell SD, Miller NL. Radiation From Kidney-Ureter-Bladder Radiographs Is Not Trivial. Urology 2019; 125: 46–49. DOI: 10.1016/j.urology.2018.11.035.
- Dong S-Z, Zhu M, Bulas D. Techniques for minimizing sedation in pediatric MRI. J Magn Reson Imaging 2019; 50 (4): 1047–1054. DOI: 10.1002/jmri.26703.
- Drugs ACRC on, Media C. ACR Manual On Contrast Media. American College of Radiology; 2022.
- Brown BP, Simoneaux SF, Dillman JR, Rigsby CK, Iyer RS, Alazraki AL, et al.. ACR Appropriateness Criteria® Antenatal Hydronephrosis–Infant. J Am Coll Radiol 2020; 17 (11): S367–s379. DOI: 10.1016/j.jacr.2020.09.017.
- Karmazyn BK, Alazraki AL, Anupindi SA, Dempsey ME, Dillman JR, Dorfman SR, et al.. ACR Appropriateness Criteria® Urinary Tract Infection–Child. J Am Coll Radiol 2018; 14 (5): S362–s371. DOI: 10.1016/j.jacr.2017.02.028.
- Kalish JM, Doros L, Helman LJ, Hennekam RC, Kuiper RP, Maas SM, et al.. Surveillance Recommendations for Children with Overgrowth Syndromes and Predisposition to Wilms Tumors and Hepatoblastoma. Clin Cancer Res 2017; 23 (13): e115–e122. DOI: 10.1158/1078-0432.ccr-17-0710.
- Wang CL, Aryal B, Oto A, Allen BC, Akin O, Alexander LF, et al.. ACR Appropriateness Criteria® Acute Onset of Scrotal Pain-Without Trauma, Without Antecedent Mass. J Am Coll Radiol 2019; 16 (5): S38–s43. DOI: 10.1016/j.jacr.2019.02.016.
- Rerksuppaphol S, Barnes G. Guidelines for Evaluation and Treatment of Gastroesophageal Reflux In Infants and Children: Recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr 2006; 35 (4): 583. DOI: 10.1097/00005176-200210000-00024.
- Chung EM, Soderlund KA, Fagen KE. Imaging of the Pediatric Urinary System. Radiol Clin North Am 2017; 55 (2): 337–357. DOI: 10.1016/j.rcl.2016.10.010.
- Barnewolt CE, Acharya PT, Aguirre Pascual E, Back SJ, Beltrán Salazar VP, Chan PKJ, et al.. Contrast-enhanced voiding urosonography part 2: urethral imaging. Pediatr Radiol 2021; 51 (12): 2368–2386. DOI: 10.1007/s00247-021-05116-6.
- Duran C, Beltrán VP, González A, Gómez C, Riego Jdel. Contrast-enhanced Voiding Urosonography for Vesicoureteral Reflux Diagnosis in Children. Radiographics 2017; 37 (6): 1854–1869. DOI: 10.1148/rg.2017170024.
- Sheehy N, Tetrault TA, Zurakowski D, Vija AH, Fahey FH, Treves ST. Pediatric 99mTc-DMSA SPECT Performed by Using Iterative Reconstruction with Isotropic Resolution Recovery: Improved Image Quality and Reduced Radiopharmaceutical Activity. Radiology 2009; 251 (2): 511–516. DOI: 10.1148/radiol.2512081440.
- Wood LN, Souders CE, Freedman AL. Is a Reassuring MAG-3 Diuretic Renal Scan Really Reassuring? Curr Urol 2014; 8 (4): 178–182. DOI: 10.1159/000365713.
- Rodger F, Roditi G, Aboumarzouk OM. Diagnostic Accuracy of Low and Ultra-Low Dose CT for Identification of Urinary Tract Stones: A Systematic Review. Urol Int 2018; 100 (4): 375–385. DOI: 10.1159/000488062.
- Voss SD. Staging and following common pediatric malignancies: MRI versus CT versus functional imaging. Pediatr Radiol 2018; 48 (9): 1324–1336. DOI: 10.1007/s00247-018-4162-4.
- Darge K, Anupindi SA, Jaramillo D. MR Imaging of the Abdomen and Pelvis in Infants, Children, and Adolescents. Radiology 2011; 261 (1): 12–29. DOI: 10.1148/radiol.11101922.
- Calvo-Garcia MA, Kline-Fath BM, Levitt MA, Lim F-Y, Linam LE, Patel MN, et al.. Fetal MRI clues to diagnose cloacal malformations. Pediatr Radiol 2011; 41 (9): 1117–1128. DOI: 10.1007/s00247-011-2020-8.
- Hwang JY, Shin JH, Lee YJ, Yoon HM, Cho YA, Kim KS. Percutaneous nephrostomy placement in infants and young children. Diagn Interv Imaging 2018; 99 (3): 157–162. DOI: 10.1016/j.diii.2017.07.002.
- Sweed Y, Singer-Jordan J, Papura S, Loberant N, Yulevich A. Use of angiographic embolization in pediatric abdominal trauma-induced solid organ injuries. Ulus Travma Acil Cerrahi Derg 2016; 8 (11): 65–68. DOI: 10.5505/tjtes.2018.00056.
- Kaufman CS, James CA, Harned RK, Connolly BL, Roebuck DJ, Cahill AM, et al.. Pediatric interventional radiology workforce survey: 10-year follow-up. Pediatr Radiol 2017; 47 (6): 651–656. DOI: 10.1007/s00247-017-3796-y.
- Pierce CB, Muñoz A, Ng DK, Warady BA, Furth SL, Schwartz GJ. Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int 2021; 99 (4): 948–956. DOI: 10.1016/j.kint.2020.10.047.
- Dillman JR, Trout AT, Smith EA. MR urography in children and adolescents: techniques and clinical applications. Abdom Radiol (NY) 2016; 41 (6): 1007–1019. DOI: 10.1007/s00261-016-0669-z.
- Chow JS, Koning JL, Back SJ, Nguyen HT, Phelps A, Darge K. Classification of pediatric urinary tract dilation: the new language. Pediatric Radiology 2017; 47: 1109–1115.
Ultima atualização: 2025-09-21 13:35