
33: Reoperación de hipospadias
Este capítulo durará aproximadamente 17 minutos para leer.
Introducción
El hipospadias secundario es un término reservado para individuos con complicaciones anatómicas y funcionales persistentes tras múltiples reparaciones correctivas del hipospadias. Estas incluyen la formación de estenosis, fístula uretrocutánea, dehiscencia del glande, dehiscencia uretral, chordee persistente y deformidad del glande. El hipospadias se define por tres características principales: un meato situado ventralmente, un grado variable de chordee y un aspecto 'en capucha’ del prepucio debido al exceso de piel prepucial dorsal, presentando cada componente un amplio espectro de gravedad. Por lo tanto, en los pacientes que se presentan para una reoperación tras una reparación primaria, es vital reconocer la combinación de componentes individuales que no ha logrado maximizar el resultado en una reoperación. También existe una mayor tasa de fistulización recurrente y de estenosis debido a la disminución de la vascularización tisular.
Otro aspecto crítico a tener en cuenta es que la población de pacientes que requieren una reparación secundaria tiende a ser de mayor edad, con estudios que destacan un grado significativo de comorbilidad psicológica y trastornos del neurodesarrollo.1,2 La mayoría de los ‘lisiados’ por hipospadias habrían tenido en promedio más de tres intentos fallidos de uretroplastia, y el fracaso tiende a aparecer muchos años después de haber logrado un resultado inicial satisfactorio.3 Anthony Mundy describió la magnitud de este desafío en el manejo de estas cohortes de pacientes en su revisión editorial. Hizo hincapié en que es casi imposible escribir un buen artículo de revista sobre la reparación fallida del hipospadias.4 Al reconocer las complicaciones posteriores a una reparación primaria de hipospadias, no se puede adoptar un ‘enfoque de talla única para todos’ sino que se requiere un enfoque individualizado. Este capítulo describe la incidencia y los factores predisponentes y propone un algoritmo general de manejo para los niños que necesitan una reoperación de hipospadias. Además, se describirá la técnica quirúrgica preferentemente utilizada en nuestra institución. Este capítulo también revisará estrategias alternativas para cada una de las complicaciones individuales frecuentes que posteriormente conducen a la necesidad de una reoperación.
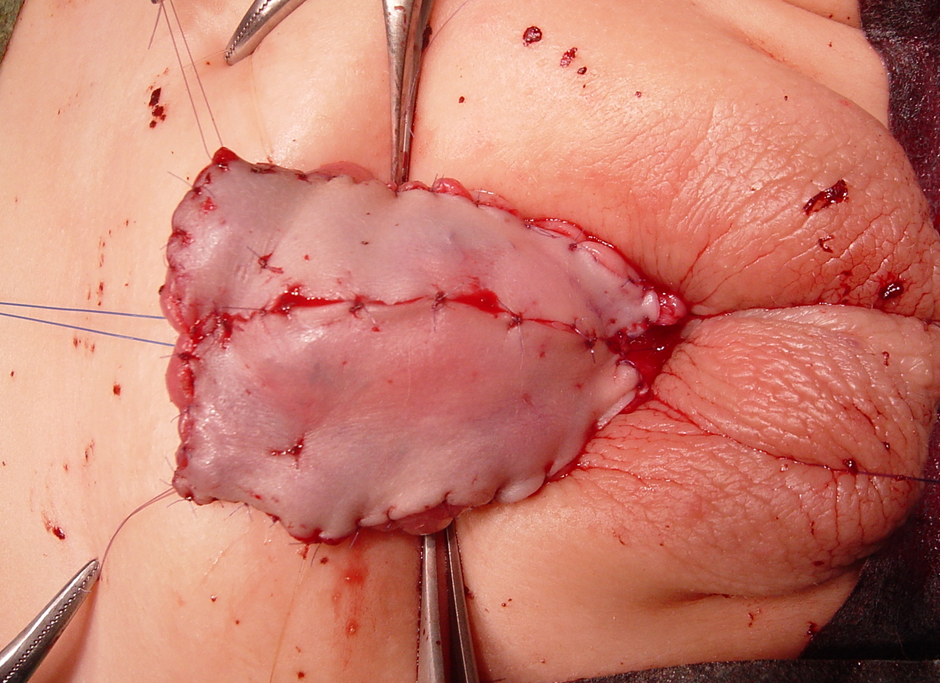
Figura 1 Injerto de piel prepucial con suturas de acolchado en una reparación de hipospadias en 1er tiempo. Obsérvese el glande del pene, que ha sido dividido y dejado ampliamente abierto.
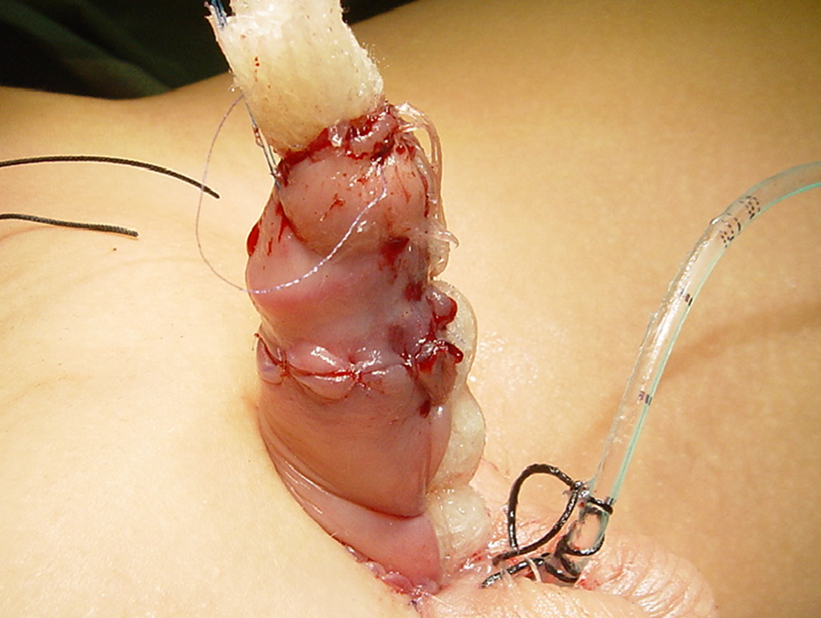
Figura 2 jelonet enrollado fijado para proporcionar humedad e inmovilizar el injerto cutáneo.
Incidencia
Las reintervenciones quirúrgicas dependen principalmente de dos factores críticos: el volumen de casos de la institución y la experiencia técnica del cirujano actuante. Por lo tanto, esta incidencia varía ampliamente entre centros. Barbagli et al informaron en su análisis retrospectivo de una única cohorte de adolescentes que el 50% de los pacientes con estenosis uretral peneana tenía antecedentes de una reparación de hipospadias fallida. De la cohorte, el 16.4% se había sometido a cirugía por hipospadias distal primario, y la mayoría había tenido más de una operación para reparar el defecto primario. Desde el punto de vista demográfico, el 21.2% de los pacientes tenía entre 1 y 16 años, y el 38.4% entre 17 y 20 años.5 Estos hallazgos pusieron de relieve la necesidad de un seguimiento a largo plazo y subrayaron la necesidad de una transición asistencial efectiva.
Factores de riesgo
Las complicaciones de la uretroplastia se duplican en las personas sometidas a una segunda uretroplastia por hipospadias en comparación con aquellas reparadas de forma primaria. Estos riesgos aumentan hasta el 40% con tres o más reoperaciones adicionales.6 La etiopatogenia de la reparación fallida del hipospadias es multifactorial. La infección posoperatoria, la extravasación de orina, los tejidos cicatriciales residuales, el hematoma y las técnicas quirúrgicas deficientes contribuyen a la alteración de la cicatrización tisular del injerto y a la isquemia. Los tejidos ventrales cicatrizados, combinados con la falta de tejido circundante en los hipospadias reparados de forma secundaria, predisponen a los pacientes a un resultado desfavorable.7 Teóricamente, la desproporción entre el crecimiento de la neouretra reconstruida y el estirón puberal del tejido cavernoso circundante al inicio de la pubertad puede resultar en un conducto corto y estrecho y manifestarse como una estenosis. En la población pediátrica, se reconoce que una mayor edad al momento de la reparación se asocia con un mayor riesgo de complicaciones.8 En nuestra opinión, un cirujano con experiencia en hipospadias debería realizar la reparación secundaria en un centro de alto volumen. Existe evidencia de que el volumen quirúrgico se correlaciona positivamente con los resultados de los pacientes, especialmente en este grupo de pacientes.9
Diagnóstico
La evaluación clínica de los pacientes no difiere mucho de la de quienes se presentan inicialmente con hipospadias. Los detalles operatorios de cirugías previas son imprescindibles si los pacientes proceden de otro centro. Al contemplar la reparación, se debe documentar la localización del meato, el volumen del glande, la longitud peneana, la curvatura peneana recurrente (si la hubiera), y la profundidad y la anchura de la placa uretral. Otras consideraciones igualmente críticas son la extensión del tejido cicatricial y la disponibilidad de sitios donantes para injerto, en caso de emprender un abordaje en dos tiempos. Un examen físico exhaustivo es obligatorio y debe documentarse con todo detalle; rara vez es necesaria una valoración radiológica adicional. Las características del paciente y las preferencias técnicas y la experiencia del cirujano influirán en el tipo de reparación. Por último, los posibles riesgos y beneficios de la reparación secundaria deben discutirse junto con los padres como parte de un proceso de toma de decisiones compartida.
Planificación perioperatoria
Emprender una reintervención por hipospadias es técnicamente exigente y se asocia con tasas más altas de complicaciones. El resultado funcional siempre tendrá prioridad sobre la estética, lo cual debe comunicarse claramente. La ubicación “normal” del meato se considera ampliamente la punta distal del glande. Sin embargo, se ha comunicado que variaciones significativas en la ubicación del meato preservan la función sexual y miccional a lo largo de la adultez en hombres con hipospadias no tratado.10 Además del sitio meatal, una encuesta encontró que los hombres con hipospadias “más leve” o distal no tratados reportan dificultades con el coito, en su mayoría asociadas con la curvatura peneana, pero sin problemas urinarios significativos en comparación con hombres normales.10 Considerando el resultado de la encuesta y aplicado al contexto de reparaciones secundarias, la corrección de la curvatura peneana sería la principal consideración. Si se contempla un abordaje quirúrgico en dos etapas, se recomienda un intervalo mínimo de 6 meses entre procedimientos para permitir una cicatrización adecuada de la herida. En la literatura se han reportado coadyuvantes para favorecer la cicatrización tisular en las reintervenciones por hipospadias, especialmente inyecciones de nitroglicerina y terapia con oxígeno hiperbárico para aumentar la vascularidad tisular y promover la cicatrización de la herida.11 Sin embargo, estas terapias de apoyo aún no han logrado una amplia aceptación. En niños con un glande peneano pequeño y un falo corto, existe un debate continuo entre los especialistas sobre el uso de la estimulación androgénica preoperatoria. Algunos sectores abogan por su uso en hipospadias severo para aumentar la longitud del falo, la circunferencia del glande, la vascularidad peneana y la robustez tisular, elementos esenciales en cualquier reintervención. Sin embargo, evidencia contradictoria sugiere que la estimulación hormonal preoperatoria se asocia con mayores tasas de complicaciones en el hipospadias proximal, aunque sin significación estadística.12
Antibióticos
Recomendaríamos cobertura antibiótica en una reoperación de hipospadias para minimizar el riesgo de infecciones del sitio quirúrgico y del tracto urinario. Debe realizarse un urocultivo preoperatorio, y la presencia de bacteriuria debe tratarse según el cultivo y el antibiograma. A pesar de que estudios no han encontrado diferencias significativas en las infecciones del sitio quirúrgico y del tracto urinario con o sin profilaxis antibiótica preoperatoria,13,14 utilizamos co-amoxiclav (amoxicilina/ácido clavulánico 30 mg/kg) por vía intravenosa como antibiótico de primera elección. Luego se continúa por vía oral en el período posoperatorio durante una semana, hasta que se retiren el catéter y el apósito. Nuestra práctica se alinea en general con el estudio que informó que el 91% de los urólogos pediátricos prescribe antibióticos posoperatorios cuando se deja un catéter uretral en su lugar.15 Aunque debatible, un metanálisis reciente que evaluó los efectos de la profilaxis antibiótica posoperatoria tras la reparación del hipospadias encontró una utilidad limitada para prevenir infecciones y complicaciones de la cicatrización, aunque el riesgo de sesgo fue alto en muchos de los estudios.16,17 Brindar apoyo a la recuperación de los pacientes con una analgesia adecuada es esencial, ya que por lo general requerirán una disección tisular más extensa con una reconstrucción más compleja. El bloqueo caudal sería la opción más común para el control del dolor perioperatorio. De forma alternativa, también pueden utilizarse bloqueos de nervios periféricos (bloqueo del nervio dorsal del pene y bloqueo del nervio pudendo). La evidencia sigue siendo inconcluyente en cuanto a la elección de la analgesia y su relación con los resultados posoperatorios en las reparaciones de hipospadias.18,19
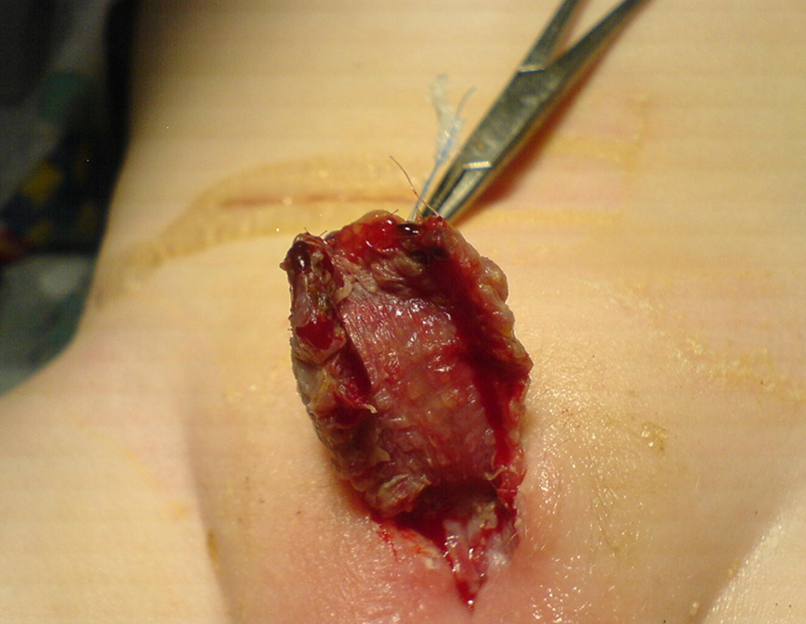
Figura 3 Apariencia del injerto cutáneo una semana después de la cirugía. El cuidador familiar debe continuar masajeando el injerto con vaselina o ungüento de manteca de cacao para optimizar la cicatrización y prevenir la contractura del injerto.

Figura 4 Aspecto del injerto cutáneo 6 meses después de la reparación de la 1ª etapa. Buena cicatrización sin evidencia de contractura del injerto. Está listo para la 2.ª etapa de la reparación.
Técnicas quirúrgicas
Se han descrito diferentes enfoques para técnicas de rescate en la reoperación de hipospadias, incluyendo la uretroplastia con placa incisa tubularizada (TIP), la reparación de Mathieu, colgajos en isla tubularizados tipo onlay (OIF) e injertos libres, realizados ya sea en una sola etapa o en dos etapas. Independientemente de las diferentes técnicas, siempre se deben aplicar los principios generales de la cirugía y la reparación. El uso mínimo de electrocauterio, suturas sin tensión, injertos o tejidos circundantes bien vascularizados y múltiples planos con cierre hermético minimizarán las complicaciones potenciales habituales. Una uretroplastia TIP puede ser una opción en una reparación en una sola etapa si la placa uretral está presente y es lo suficientemente ancha. Snodgrass y Lorenzo comunicaron su experiencia inicial con el uso de la uretroplastia TIP en la reoperación de hipospadias. Incluyeron 15 pacientes, con un seguimiento medio de 5 meses. Lograron un meato con aspecto cosméticamente normal en 13 de 15 pacientes, y las complicaciones consistieron en dos fístulas y una dehiscencia del glande.6 Shanberg y colegas comunicaron la uretroplastia TIP en 13 casos reoperados, con un seguimiento medio de 22 meses. Los resultados cosméticos fueron excelentes, con dos complicaciones: un paciente con dehiscencia del glande y una fístula uretrocutánea, y un segundo paciente que desarrolló estenosis meatal.20 Una placa uretral marcadamente cicatrizada que contribuya a la curvatura peneana (chordee) debe ser escindida y reemplazada por un injerto de mucosa bucal para una reparación en dos etapas, como lo propuso Bracka.21
Bracka popularizó la reparación en dos tiempos en la cirugía de hipospadias como una posible solución a las altas tasas de complicaciones observadas tras un abordaje en un solo tiempo. Informó la serie más extensa en la literatura con seiscientos casos (457 niños y 143 adultos), de los cuales el 34.8% fueron reparaciones secundarias. En total, el 3.7% requirió revisión del primer tiempo. La tasa de fístula uretrocutánea fue del 10.5% para la cirugía de rescate, mientras que la tasa de formación de estenosis fue del 7%.22 Hayes et al informaron el uso de injertos de mucosa bucal en reparaciones en múltiples tiempos en 25 pacientes (tanto adultos como niños) con reparación de hipospadias previamente fallida. El 22% requirió revisión del primer tiempo, mientras que solo un paciente (4%) desarrolló una fístula uretrocutánea.23 Barbagli et al estudiaron a 60 adultos con hipospadias secundario, de los cuales 31 casos se sometieron a reparaciones en múltiples tiempos. Los injertos de mucosa bucal resultaron en un 82% de éxito en procedimientos en un tiempo y en un 82% en procedimientos en múltiples tiempos. La tasa de fístula para operaciones en un tiempo y en dos tiempos fue del 10.3% y del 6.5%, respectivamente.5 Kulkarni et al destacaron la mayor incidencia de contractura del injerto de mucosa bucal en su serie de pacientes sometidos a una reparación en 2 tiempos con BMGs (injerto de mucosa bucal), lo que motivó su cambio de técnica hacia un abordaje híbrido.24
En el Hospital para Niños Great Ormond Street (GOSH), nuestra reparación en dos tiempos combina técnicas descritas históricamente por Turner-Warwick, Duplay y Cloutier.25 En el primer tiempo de la reparación, la uretra cicatrizada se abre ventralmente en la línea media hasta llegar a tejido sano sangrante. Se completa una incisión de circuncisión alrededor de la corona del pene, a menudo coincidiendo con la incisión previa y dejando un manguito de mucosa proximal al glande. Luego se reseca el área cicatrizada dentro del glande, y el glande se abre ampliamente mediante una incisión profunda en la línea media, despegando después el tejido glandular del ápice. La uretra se extiende hasta una zona sana con tejido de buen calibre antes de la escisión de la neouretra distal y del tejido cicatricial. La neouretra fracasada se reseca parcial o totalmente hasta el tejido sano. La incurvación peneana (chordee) se identifica mediante una erección artificial, usando un torniquete e inyección de solución salina, y se corrige mediante una combinación de liberación ventral de la neouretra cicatrizada y plicaturas adicionales de la túnica albugínea dorsal cuando está indicado. Es necesario confeccionar una amplia abertura uretral proximal y recolocar la piel del tronco en el dorso del pene. Esto deja una zona cruenta variable en la superficie ventral desde la abertura uretral hasta la punta del glande distalmente y entre los bordes cutáneos. Si hay un exceso de piel prepucial sana disponible, la utilizamos con preferencia a otros injertos. Sin embargo, por lo general, es necesario tomar injertos de localizaciones alternativas. Estos suelen ser el injerto cutáneo retroauricular (Wolfe), el injerto de mucosa bucal de la cara interna de la mejilla y los injertos compuestos (injerto de mucosa bucal más prepucio interno). Se obtiene el injerto cutáneo de elección y luego se desengrasa antes de aplicarlo a la zona cruenta de la superficie ventral del pene. Los injertos suelen ser rectangulares (al menos 2 cm de ancho), se suturan circunferencialmente con 6/0 monocryl y los fijamos a los cuerpos cavernosos con suturas adicionales de acolchado. Los injertos se comprimen contra el tronco del pene utilizando un jelonet enrollado (gasa de parafina) y se suturan en su lugar uniendo entre sí los bordes de la piel del tronco por encima. Luego cubrimos el pene y aplicamos presión adicional utilizando una espuma y un vendaje externo con cinta Elastoplast. Según la edad del paciente, se utiliza un stent de goteo o un catéter de drenaje continuo (todos los pacientes menores de seis años tendrán un stent de goteo).
Se administrarán antibióticos y anticolinérgicos durante la primera semana Se retira el apósito y se inspecciona el injerto bajo anestesia general. Se instruye a los padres a aplicar pomada de cloranfenicol sobre el injerto dos veces al día durante diez días. Tras la revisión a los tres meses en la clínica de consultas externas, se planifica el procedimiento de segunda etapa si el injerto es satisfactorio. De no ser así, se empleará un período de aplicación de pomada de dihidrotestosterona para madurar aún más el injerto y estimular el crecimiento peniano. Los procedimientos de segunda etapa se realizan no antes de seis meses, y la mayoría de los casos se reparan más cerca de 1 año. La placa uretral y el glande se cierran alrededor de un catéter 8-Fr, utilizando suturas Monocryl 6-0. Se aplica otro apósito de espuma con drenaje por catéter, antibióticos y anticolinérgicos durante una semana. Posteriormente, el retiro del apósito lo realiza nuestro personal de enfermería en la sala (sin ninguna sedación). Los pacientes se controlan a los 3 y 12 meses en la clínica de consultas externas.
Fístula uretrocutánea
La fístula uretrocutánea es una de las complicaciones más frecuentes tras la reparación primaria del hipospadias, con una incidencia citada entre el 5% y el 15%. Entre los riesgos reconocidos se incluyen la edad al momento de la reparación, el hematoma, la necrosis del injerto, la extravasación urinaria, la infección de la herida y la experiencia del cirujano operador. Una revisión retrospectiva multicéntrica de 591 pacientes realizada por Duarsa et al concluyó que el drenaje suprapúbico reduce el riesgo de fístula uretrocutánea tras la reparación de hipospadias. Los autores postularon que la creación percutánea de una derivación urinaria temporal reduce el drenaje urinario hacia la neouretra y minimiza la reacción tisular, la movilidad de las suturas y el riesgo de infección.10 También es fundamental descartar una estenosis del neomeato distal o isquemia de la piel ventral. El manejo quirúrgico dependerá del tamaño del meato, del número de fístulas y de si existen estenosis concomitantes de la neouretra. Kulkarni et al han descrito sus técnicas de reparación de fístulas, según las cuales, en casos de meato estrecho con una estenosis uretral, la uretra se incide ventralmente hasta visualizar una uretra de buen calibre. Si la placa uretral mide más de 8 mm, se realiza una uretroplastia de aumento con injerto dorsal inlay en un solo tiempo según Asopa. Si la anchura es inferior a 8 mm, se emplea un abordaje en dos tiempos para tubularizar una neouretra. Por último, si la uretra es de buen calibre y no hay obstrucción distal, la fístula uretrocutánea puede cerrarse de forma primaria.24
Curvatura peneana ventral recurrente
La curvatura ventral (CV) se observa con mayor frecuencia en pacientes sometidos a plicatura dorsal, en contraste con los sometidos a un procedimiento de alargamiento peneano ventral. Otro factor contribuyente es la contractura de la piel ventral cicatrizada y del tejido fibroso periuretral. Flynn et al comunicaron la aparición tardía de curvatura peneana recurrente tras la reparación de hipospadias, después de la pubertad. La mayoría de sus pacientes refirieron que la curvatura peneana se asociaba con el crecimiento del falo en la pubertad. Postularon que la CV recurrente, especialmente en adolescentes, se debe a la asimetría de la pared de los cuerpos cavernosos, que puede ser secundaria a un crecimiento desproporcionado de la pared ventral hipoplásica de los cuerpos cavernosos o de la uretra reconstruida.26 Una desproporción entre una uretra ventral corta y los tejidos de los cuerpos cavernosos es crucial en la curvatura ventral recurrente.27 En la mayoría, una curvatura ‘leve’ (menos de 30 grados) puede corregirse mediante disección cutánea o transección de la placa uretral. La mayoría en reintervenciones de hipospadias requerirá abordar una desproporción corporal subyacente con, esencialmente, dos opciones: acortar el lado largo o alargar el lado corto. Entre los pacientes con hipospadias en los que la longitud es valiosa, probablemente sea mejor evitar la plicatura dorsal. Se prefieren las corporotomías ventrales transversas en las curvaturas ventrales recurrentes, lo que conduce a un grado razonable de corrección. En casos de curvatura mayor de 30 grados, puede considerarse una reparación en etapas que comience con la exéresis de la uretra y la colocación de un injerto dérmico sobre los cuerpos cavernosos, y cobertura con colgajo de dartos y colgajo cutáneo local.24

Figura 5 Aspecto final tras la tubulización al final de la 2.ª etapa de la reparación. Se dejará el catéter durante siete días; posteriormente se retirará el apósito en la sala de hospitalización.

Figura 6 Presencia de una fístula uretrocutánea aislada tras la reparación de hipospadias. Es susceptible de una simple escisión y cierre de la fístula
Cuidados postoperatorios
La reparación secundaria de hipospadias en el GOSH se realiza como un procedimiento de ingreso de un día, con alta del niño al día siguiente tras una noche de observación. Cateterizamos a todos los niños con una sonda de alimentación blanda de 8 French y la fijamos al glande con un punto de fijación de prolene 4-0, que permanece en su lugar durante siete días. Un vendaje oclusivo circunferencial optimiza la cicatrización posoperatoria al promover la inmovilización, la protección del sitio quirúrgico, la adhesión tisular y la compresión. Actualmente, no existe consenso sobre el tipo de vendaje más eficaz o siquiera si aplicar un vendaje es beneficioso. Un ensayo aleatorizado no encontró diferencias significativas en las tasas de complicaciones ni en los resultados clínicos al comparar pacientes con vendaje y sin vendaje. Cabe destacar que hubo un aumento significativo de las llamadas posoperatorias de los padres en el grupo sin vendaje.28 Siguiendo la técnica de vendaje descrita anteriormente, colocamos doble pañal en los niños que aún no han adquirido el control de esfínteres. El catéter y el vendaje se retiran a los siete días, bajo anestesia general en las reparaciones de primera etapa con injerto y de forma local en la sala tras las reparaciones de segunda etapa. En los niños mayores, se conecta un catéter Foley a una bolsa de drenaje. Prescribimos antibióticos orales según nuestra política local de microbiología y oxibutinina 0.2 g/kg una vez al día hasta que se retire el catéter para prevenir espasmos vesicales. El bloqueo nervioso caudal preoperatorio ayuda a mitigar el dolor posoperatorio.29 Un mayor control del dolor se logra con dosis bajas de analgésicos AINE (antiinflamatorios no esteroideos).
Conclusión
La reoperación por hipospadias es una entidad quirúrgicamente desafiante de tratar y manejar entre los cirujanos que atienden activamente a niños con hipospadias. Debido a su baja tasa de complicaciones y a técnicas reproducibles, los autores recomiendan una reparación en dos etapas para una cirugía de reoperación por hipospadias. No obstante, si todo falla a pesar de los mejores intentos, puede considerarse también la uretrostomía perineal como una opción para preservar la calidad de vida en estos pacientes. Existe evidencia de alta calidad limitada en la literatura actual que examine los diversos aspectos del manejo quirúrgico de la reoperación por hipospadias. Por lo tanto, debería incentivarse un mayor esfuerzo de investigación adicional para mejorar los resultados de los pacientes. A continuación se presenta el esquema de un algoritmo sencillo para el manejo quirúrgico de la reoperación por hipospadias.

Figura 7 Algoritmo de manejo propuesto para hipospadias de reoperación o reintervención.
Recursos para la familia
- Recursos sobre hipospadias, Hospital de Niños de Filadelfia
- Información de urología para padres y visitantes, Hospital Great Ormond Street para Niños
Lecturas recomendadas
- Shukla AR, Patel RP, Canning DA. Hypospadias. J Pediatr Urol: 103–126. DOI: 10.1385/1-59259-421-2:103.
- Chapter 15: Hypospadia Paediatric Urology WebBook, European Society of Paediatric Urology. 20AD: 227–256.
Referencias
- Butwicka A, Lichenstein P, Landen M. Hypospadias and increased risk for neurodevelopmental disorders. Child Psychol Psychiatry 2015; 56 (2): 155–161.
- Jin TT, Wu WZ, Shen ML. Hypospadias and Increased Risk for Psychiatric Symptoms in Both Childhood and Adolescence: A Literature Review. Front Psychiatry 2022; 13: 799335. DOI: 10.3389/fpsyt.2022.799335.
- Craig W JR, C B, WO H, JM M, J.B.. Management of adults with prior failed hypospadias surgery. 2014; 3 (2): 196–204.
- Mundy AR. Failed hypospadias repair presenting in adults. Eur Urol 2006 (5): 774–776.
- Barbagli G, Perovic S, Djinovic R, Sansalone S, Lazzeri M. Retrospective descriptive analysis of 1,176 patients with failed hypospadias repair. J Urol 2010 (1): 207–211. DOI: 10.1016/s0084-4071(10)79536-1.
- Snodgrass WT. A Lorenzo Tubularized incised plate for hypospadias reoperation. BJU Int 2002; 89: 98–100. DOI: 10.1097/01.ju.0000125018.90605.a5.
- Al-Sayyad A, Pike JG, Leonard MP. Redo hypospadias repair: experience at a tertiary care children’s hospital. Can Urol Assoc J 2007; 1 (1). DOI: 10.5489/cuaj.39.
- Duarsa GWK, Tirtayasa PMW. Risk factors for urethrocutaneous fistula following hypospadias repair surgery in Indonesia. J Pediatr Urol 2020; 16 (3): 317.e1–317. DOI: 10.1016/j.jpurol.2020.04.011.
- Wilkinson DJ, Green PA, Beglinger S. Hypospadias surgery in England: Higher volume centres have lower complication rates. J Pediatr Urol 2017; 13 (5): 481.e1–481.e6.
- Fichtner J, Filipas D, Mottrie AM, Voges GE, Hohenfellner R. Analysis of Meatal Location in 500 Men: Wide Variation Questions Need for Meatal Advancement in All Pediatric Anterior Hypospadias Cases. J Urol 1995; 154 (2): 833–834. DOI: 10.1016/s0022-5347(01)67177-5.
- Dodds PR, Batter SJ, Shield DE, Serels SR, Garafalo FA, Maloney PK. Adaptation of Adults to Uncorrected Hypospadias. Urology 2008; 71 (4): 682–685. DOI: 10.1016/j.urology.2007.07.078.
- Chang C, White C, Katz A, Hanna MK. Management of ischemic tissues and skin flaps in Re-Operative and complex hypospadias repair using vasodilators and hyperbaric oxygen. J Pediatr Urol 2020; 16 (5): 672.e1–672.e8. DOI: 10.1016/j.jpurol.2020.07.034.
- Wright I, Cole E, Farrokhyar F, Pemberton J, Lorenzo AJ, Braga LH. Effect of Preoperative Hormonal Stimulation on Postoperative Complication Rates After Proximal Hypospadias Repair: A Systematic Review. J Urol 2013; 190 (2): 652–660. DOI: 10.1016/j.juro.2013.02.3234.
- Smith J, Patel A, Zamilpa I. Commentary to ‘Is parenteral antibiotic prophylaxis associated with fewer infectious complications stented, distal hypospadias repair?’ J Pediatr Urol 2017; 18 (6): 764. DOI: 10.1016/j.jpurol.2022.05.024.
- Baillargeon E, Duan K, Brzezinski A, Jednak R, El-Sherbiny M. The role of preoperative prophylactic antibiotics in hypospadias repair. Can Urol Assoc J 2014; 8 (7-8): 236. DOI: 10.5489/cuaj.1838.
- Hsieh MH, Wildenfels P, Gonzales ET. Surgical antibiotic practices among pediatric urologists in the United States. J Pediatr Urol 2011; 7 (2): 192–197. DOI: 10.1016/j.jpurol.2010.05.001.
- Chua ME, Kim JK, Rivera KC. Commentary to ‘The use of postoperative prophylactic antibiotics in stented distal hypospadias repair: a systematic review and meta-analysis.’ J Pediatr Urol 2019; 15 (2): 149. DOI: 10.1016/j.jpurol.2018.10.024.
- Zhu C, Wei R, Tong Y, Liu J, Song Z, Zhang S. Analgesic efficacy and impact of caudal block on surgical complications of hypospadias repair: a systematic review and meta-analysis. Reg Anesth Pain Med 2019; 44 (2): 259–267. DOI: 10.1136/rapm-2018-000022.
- Tanseco PP, Randhawa H, Chua ME, Blankstein U, Kim JK, McGrath M, et al.. Postoperative complications of hypospadias repair in patients receiving caudal block vs. non-caudal anesthesia: A meta-analysis. Can Urol Assoc J 2019; 13 (8): 249–257. DOI: 10.5489/cuaj.5688.
- Retik AB, Borer JG. Primary and Reoperative Hypospadias Repair With the Snodgrass Technique. J Urol 1998; 16 (3): 1561. DOI: 10.1097/00005392-199910000-00122.
- Bracka A. Hypospadias repair: the two-stage alternative. Br J. Br J Urol 1995; 76: 31–41. DOI: 10.1111/j.1464-410x.1995.tb07819.x.
- Bracka A. The role of two-stage repair in modern hypospadiology. Indian J Urol 2008; 24 (2): 210–218.
- Hayes MC, Malone PS. The use of a dorsal buccal mucosal graft with urethral plate incision (Snodgrass) for hypospadias salvage. BJU Int 1999; 83 (4): 508–509. DOI: 10.1046/j.1464-410x.1999.00043.x.
- Kulkarni S, Joglekar O, Alkandari M, Joshi P. Redo hypospadias surgery: current and novel techniques. Res Rep Urol 2018; Volume 10: 117–126. DOI: 10.2147/rru.s142989.
- S JN, T N, K OM, M CP. The two-stage repair for severe primary hypospadias. Eur Urol 2006; 50 (2): 366–371.
- Flynn JT, Johnston SR, Blandy JP. Late Sequelae of Hypospadias Repair. Br J Urol 1980; 52 (6): 555–559. DOI: 10.1111/j.1464-410x.1980.tb03114.x.
- Abosena W, Talab SS. Moneer K Hanna Recurrent chordee in 59 adolescents and young adults following childhood hypospadias repair. J Pediatr Urol 2020; 162 (e1-162.e5). DOI: 10.1016/j.jpurol.2019.11.013.
- Van Savage JG, Palanca LG, Slaughenhoupt BL. A Prospective Randomized Trial Of Dressings Versus No Dressings For Hypospadias Repair. J Urol 2000: 981–983. DOI: 10.1097/00005392-200009020-00015.
- O’Kelly F, Pokarowski M, DeCotiis KN, McDonnell C, Milford K, Koyle MA. Structured opioid-free protocol following outpatient hypospadias repair - A prospective SQUIRE 2.0-compliant quality improvement initiative. J Pediatr Urol 2020; 16 (5): 647.e1–647.e9. DOI: 10.1016/j.jpurol.2020.06.012.
- Shukla AR, Patel RP, Canning DA. Hypospadias. J Pediatr Urol: 103–126. DOI: 10.1385/1-59259-421-2:103.
- Chapter 15: Hypospadia Paediatric Urology WebBook, European Society of Paediatric Urology. 20AD: 227–256.
Última actualización: 2025-09-21 13:35