
56: 急性阴囊
阅读本章大约需要 8 分钟。
引言
“急性阴囊”是指阴囊疼痛和/或肿胀的症状快速起病。睾丸扭转(TT)是所有临床医生首先、最为担忧的诊断;若不及早干预,睾丸将因缺血时间过长而有发生坏死的风险。一旦排除TT,可再考虑其他病因。总的来说,儿科急性阴囊的鉴别诊断还包括睾丸阑尾扭转、附睾炎、睾丸炎、嵌顿疝、血管炎、睾丸外伤和蜂窝织炎。本章将重点介绍对睾丸扭转、睾丸或附睾附件扭转以及附睾炎的评估。这些疾病的主要致病原因与睾丸或附睾自身的解剖结构有关;而其他诊断则属于引起阴囊肿胀、疼痛或感染的继发性原因(例如,Paramyxoviridae病毒所致腮腺炎继发的睾丸炎)。对上述鉴别诊断中的其他疾病的诊断与处理需要针对原发病因进行治疗,相关内容在本教材其他部分讨论。
解剖学与胚胎学
阴囊是位于阴茎下方的由皮肤及其下方组织构成的囊,内含睾丸和附睾。在皮肤的深面是肉膜,它是会阴的Colles筋膜、阴茎的肉膜以及腹部的Scarpa筋膜的连续结构。肉膜本质上具有弹性。它为阴囊皮肤供血,并与提睾肌反射一起,通过收缩(上提)或松弛(下垂)整个阴囊来帮助调节睾丸的温度。阴囊由阴囊中隔分为左右侧间室。在内部,中隔由增厚的肉膜构成。在外观上,中隔表现为阴囊正中缝。
鞘膜是衬覆阴囊内部并包绕睾丸的结构性内衬。鞘膜源自 processus vaginalis(或 vaginal process),即胚胎期腹膜的一种外突,在其闭合之前沿腹股沟管全程延伸进入阴囊。腹股沟段闭合后,残余的远端囊袋包绕睾丸,并由两层构成:脏层与壁层。脏层与睾丸最外层的白膜密贴。壁层反折至阴囊的内面。
睾丸是位于阴囊两侧的卵圆形男性性腺,通过产生激素(即睾酮)和精子而发挥内分泌和生殖功能。精子在睾丸的曲细精管内产生,并经由睾网进入睾丸输出小管,后者与附睾头相连。附睾是一个蜿蜒盘曲的管道,位于睾丸的后外侧面。其功能是储存并使精子成熟,直到通过输精管排出,进入输精管壶腹,这里是精子成熟以备射出的储存库。
精索是位于阴囊内的一条主要结构。它起自腹壁的深(内)腹股沟环,经过腹股沟管,并穿过浅(外)腹股沟环进入阴囊。精索内含神经、血管和导管。其周围由三层筋膜组织包绕(自浅向深):外精筋膜(外斜肌筋膜的延续)、提睾肌(内斜肌肌群的延续)、以及内精索精索筋膜(腹横筋膜的延续。除了这些单独的层之外,精索还包括(图 1):
血管系统:
- 睾丸动脉(主动脉的分支)
- 提睾肌动脉和静脉(下腹壁血管的分支)
- 输精管动脉(上膀胱动脉的分支)
- 蔓状静脉丛(位于腹股沟环远端的静脉网络)
神经:
- 髂腹股沟神经(从腹股沟管内在外精筋膜浅面与精索伴行,为阴囊上部和阴茎皮肤提供感觉)
- 生殖股神经的生殖支(支配提睾肌的运动,并为阴囊前部提供感觉)
- 自主神经
其他:
- 输精管
- 淋巴管
- 腹膜鞘状突
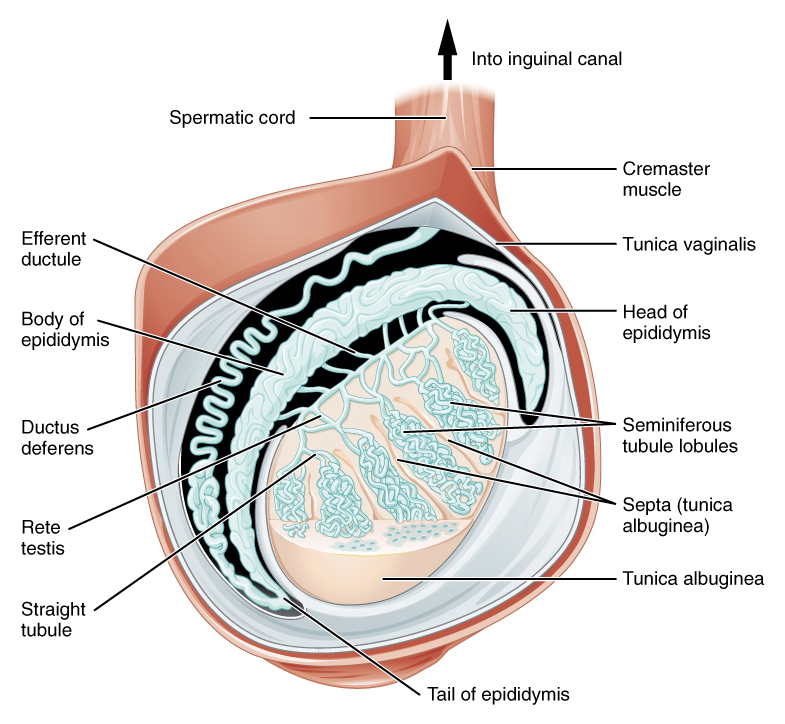
图 1 精索与睾丸鞘膜的远端内容物。来源:OpenStax College
睾丸的分化、发育和下降在其他章节中已有描述。
一般评估与诊断
对于出现急性睾丸疼痛和/或阴囊肿胀的儿童患者,应进行仔细的病史采集和体格检查。
应获取患者病史中的关键要素,包括年龄、疼痛起病性质(如起病骤然或渐进、是否有外伤)、疼痛的部位及放射情况,以及伴随症状(如腹痛、恶心或呕吐、血尿、尿痛、发热、便秘)。伴随症状既可帮助巩固对TT的诊断,也可在考虑其他诊断时排除TT。TT常见表现为腹痛、恶心和/或呕吐。另一方面,尿痛和全身性发热提示其他病因,如附睾炎。
体格检查应包括腹部检查和生殖器检查。腹部检查应包括对肋脊角压痛的评估,以寻找侧腰痛的证据,该疼痛可能代表输尿管绞痛,其牵涉痛可放射至腹股沟。还应注意并记录腹股沟区域是否有疝或蜂窝织炎的证据。1 即便仅表现为单纯腹痛,也应进行生殖器检查以排除急性阴囊,尤其是对于年幼且无法充分表达其症状的男孩、发育迟缓的男孩,以及可能存在意识状态改变的男孩。2
生殖器检查包括对阴囊及双侧睾丸的评估,先视诊后触诊。对皮肤的检查应注意是否有提示蜂窝织炎的红斑。在肤色较浅的儿童中,患有睾丸阑尾或附睾阑尾扭转的儿童,阴囊外侧皮肤可能可见淡蓝色调(“蓝点”征),尽管该体征仅见于少数病例,且对肤色较深的儿童不适用。3 通过将整个睾丸表面置于拇指与食指(及中指)之间轻轻滚动可完成轻柔触诊。由于睾丸水肿及相关的反应性、紧张性鞘膜积液,在 TT 情境下该检查常难以实施。与对侧相比处于高位的睾丸应予记录,且提示 TT(因精索扭转并缩短而使睾丸被上提)。睾丸的取向,无论是垂直还是水平,也值得关注。重要的是,钟锤畸形会使睾丸呈水平位,见于鞘膜与精索附着异常偏高的男性。这种解剖变异允许睾丸自由旋转,使患者易发生鞘膜内扭转(后文讨论)。需注意,该异常在常规情况下即难以辨别,而在 TT 情境下由于水肿和皮肤改变更不可能被明确。
额外的检查手法可能有助于确立诊断:
- 阴囊包块应通过透照试验(提示为鞘膜积液)以及尝试复位(提示鞘状突未闭)来加以界定。
- 应通过轻划受累睾丸同侧的大腿内侧来评估提睾肌反射。该反射通常会引起提睾肌收缩,使睾丸在阴囊内上提。对急性阴囊疼痛的患者,反射缺如经典上提示TT的诊断;这一发现的敏感性为100%,特异性为66%。4 然而,在年幼儿童中,反射弧可能发育不全,因而即使在其他方面健康者也可缺如。5,6 因此,首先在对侧”正常”一侧评估提睾肌反射以建立基线检查非常重要。
- 抬高阴囊内容物是一种用于区分附睾炎与TT的操作手法。抬高阴囊可缓解疼痛,传统称为Prehn征阳性,提示附睾炎;而在TT中通常不出现这一现象,尽管该检查在儿童中并非总是可靠。1
初始诊断性检查(将进一步讨论)通常包括:
- 尿液分析(UA)和尿液培养。进行这些检查是为了排除泌尿道感染和细菌性附睾炎。表现为 TT 的儿童在规范采集的尿液标本中一般不会有感染征象
- 彩色多普勒超声检查(CDUS)。这是一项确诊性检查,用于识别某侧睾丸血流缺乏
睾丸扭转
流行病学
TT的报告发病率在25岁及以下男性中可高至每4,000人1例7,在18岁及以下男性中则低至每10万人3.8例。8 发病率呈双峰分布,在生命的第一年(通常为出生后第1个月)和青春期(12岁)达到高峰。该双峰分布与新生儿期和围青春期发病机制的差异相对应(分别为鞘外性精索扭转与鞘内性精索扭转)。
发病机制
TT 发生于睾丸围绕其精索发生旋转时。扭转的精索压迫睾丸的静脉网,导致睾丸水肿、静脉回流受限,继而动脉入流闭塞。持续缺血具有破坏性,若不予以解除,将使睾丸存活的机会降至最低。
TT有两种类型:鞘膜内扭转和鞘膜外扭转。
鞘膜外睾丸扭转是指当睾丸鞘膜及其内容物(包括睾丸)围绕精索轴整体扭转时发生的情况。该现象之所以可能,是由于新生儿期阴囊各层尚未融合,使鞘膜能够在由阴囊肉膜衬里的半侧阴囊腔室内活动。鞘膜外扭转仅见于新生儿期或产前时期,亦有报道可迟至出生后1–3个月发生。9 与鞘膜内扭转相比,新生儿期TT较为少见,其发生率为每10万例6.1例。10
鞘膜内睾丸扭转 是指睾丸围绕精索在鞘膜内发生扭转。所谓 “钟锤畸形” 是使患者易发生鞘膜内睾丸扭转的主要危险因素。正常情况下,鞘膜的脏层与壁层在后方和下方彼此融合,将睾丸固定于鞘膜腔内。存在钟锤畸形的男性中,鞘膜在无脏层与壁层融合点的情况下,完全包绕睾丸、附睾以及精索的远端部分。11 一项尸检系列报告钟锤畸形的发生率为12%,值得注意的是,高于TT的发生率。12 双侧钟锤畸形的高发生率,支持在对侧未受累侧行预防性睾丸固定术。
需注意,围产期(鞘膜外)扭转一般不被认为与对侧钟锤畸形及其随后发生鞘膜内TT的风险相关。相反,一侧发生鞘膜内扭转很可能提示存在对侧钟锤畸形,并有随后发生异时性对侧鞘膜内鞘膜内扭转的风险。在一项由单一术者完成、连续纳入的50例因不可触及睾丸而入手术室探查并证实为睾丸残端的病例系列中,仅1例显示对侧钟锤畸形的证据。作者将此与27例年长男童的单纯TT病例进行对比,其中21例(78%)存在对侧钟锤畸形。13
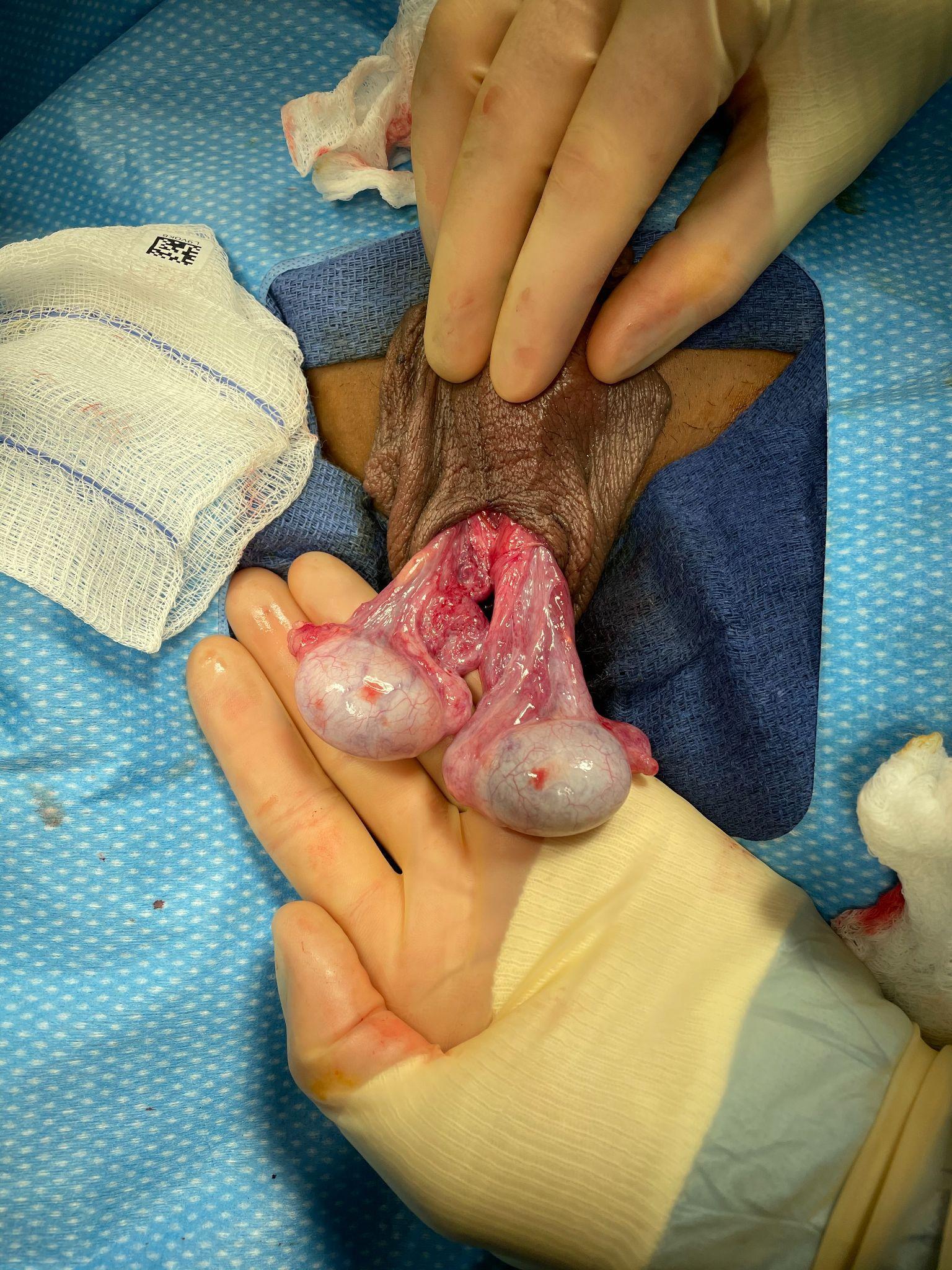
图 2 鞘膜内扭转病例中的钟舌样畸形(左侧睾丸已解扭)。两侧睾丸的鞘膜脏层与壁层均未融合,因此鞘膜退缩至精索的高位,双侧睾丸呈自由悬垂,相对于精索呈横位。可以想象,若鞘膜壁层保持完整,睾丸将完全悬置于鞘膜内,宛如钟舌一般。
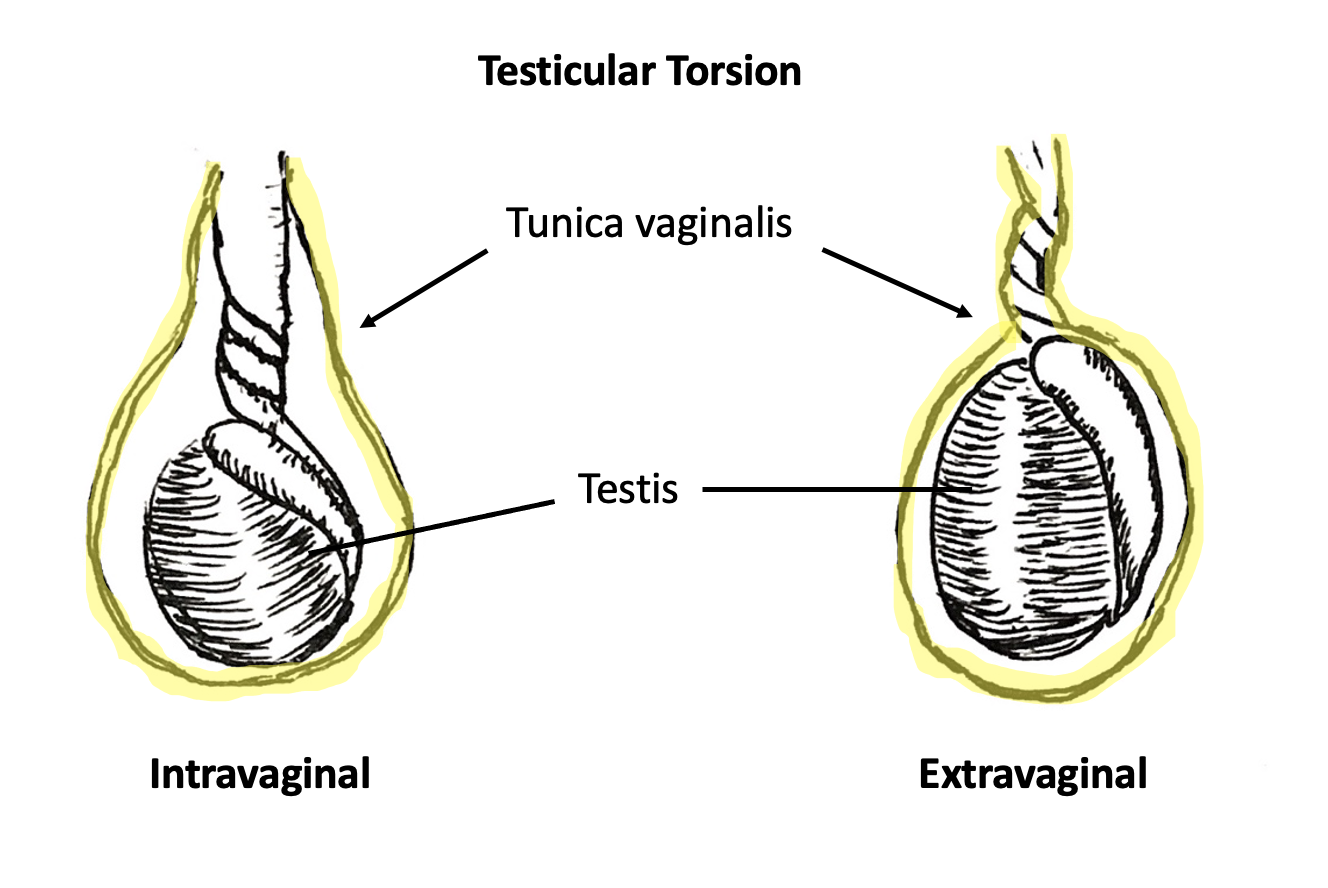
图 3 鞘膜内扭转(左)与鞘膜外扭转(右)。鞘膜以黄色标示。在鞘膜内扭转中,精索在鞘膜内单独发生扭转。在鞘膜外扭转中,精索与鞘膜作为一个整体发生扭转。
新生儿睾丸扭转的评估与诊断
患有鞘外型 TT 的新生儿的临床表现多变,这既可能反映疾病过程,也与分娩及新生儿早期护理的相关情况有关。新生儿在分娩过程中可出现会阴部水肿,出生后最初数小时内阴囊可能显得特别肿大并呈红斑样改变。还可能受到母体激素的影响。先天性鞘膜积液很常见,并且在出生后即刻可能达到最大。总体而言,这些改变可能使临床医生仅凭触诊难以区分附睾与睾丸的具体解剖结构。
新生儿的鞘膜外型TT常表现为一侧半阴囊肿大、变硬。分娩与产后护理团队需要对两侧半阴囊检查中的细微差异保持敏感。应分别对右侧和左侧半阴囊进行视诊与触诊,而不是将其作为一个整体。若发现一侧质地增硬、阴囊皱褶消失,或出现侧别性的皮肤改变,应予以记录,并提示需要重复检查。初次检查中的显著异常或在连续检查中出现的变化,应促使紧急泌尿外科会诊。
出生时即注意到的鞘外扭转不太可能得到挽救。对文献的回顾显示,被视为”产前”或”产后”的新生儿扭转中,超过90%接受了单侧睾丸切除术。14 比挽救更明显受累的一侧更重要的是及时诊断或预防异时性鞘外扭转。这常常需要手术探查,因为单侧阴囊体检所见可能非常显著,足以掩盖对侧的发现。此外,在新生儿中进行CDUS在技术上较为困难,尤其是在超声技师不习惯为新生儿成像的中心。对于怀疑单侧新生儿鞘外扭转的情况,是否紧急探查新生儿阴囊存在争议。当单侧检查提示鞘外扭转时,是否对新生男婴进行阴囊手术探查的决策,需要在患侧睾丸挽救可能性低及新生儿的麻醉风险,与异时性鞘外TT虽罕见但后果灾难性的可能性之间进行权衡。文献中不乏关于双侧、异时性鞘外扭转的病例报告。近期发表的研究尝试量化新生儿发生异时性扭转的风险。一项涵盖152项研究、代表1336名患者的文献综述报告称,所有新生儿扭转事件中有11.8%为异时性,第二次扭转的中位时间为1天。作者计算得到,为避免双侧睾丸切除术,需治疗人数(例如行手术探查)为1.6;为避免孤立睾丸萎缩,需治疗人数为2.6。另一项为期20年的单机构病历回顾报告称,围产期异时性双侧扭转的风险为3%。15 鉴于近几十年围产期麻醉安全性的改善,作者认为在单侧围产期扭转的情形下应考虑早期和紧急手术探查的益处。
年长儿童的评估与诊断
对于任何以急性起病的阴囊疼痛就诊的患者,应当尽快确诊或排除TT。这是对该器官构成最具时间敏感性威胁的诊断。临床医生应牢记,有针对性的病史采集和体格检查是进行手术探查的唯一先决条件。CDUS可用于证实怀疑的TT诊断,或排除终末器官缺血。CDUS上存在血流并不能排除正在发展的缺血(因为在出现限制动脉流入的水肿和血管充血之前,静脉回流很可能已先减少)、近期或间歇性TT,或不完全或部分扭转。在后者情况下,精索可能围其轴发生足以导致血供受损的旋转,但尚不足以使血流骤然中断。
病史
鞘膜内睾丸扭转(TT)的典型表现是在围青春期男性中急性起病的睾丸疼痛。患者或其父母常描述为疼痛突然发作且剧烈。疼痛可在静息时开始,患者常报告在睡眠中被突发疼痛惊醒。患者也可能在阴囊外伤后诉说疼痛。在后一种情况下,推测外伤本身不太可能是TT的原因,而是误记或无关的事件。事实上,近期生殖器外伤史已被认为是导致误诊并因此延误治疗的原因。2
常见的相关症状可能包括腹痛、恶心和呕吐。16 重要的是,有或无呕吐的腹痛和/或恶心可能先于睾丸疼痛的出现。这会造成诊断上的困境,并可能对那些将检查集中于腹部而忽略泌尿生殖系统检查的临床医师带来不利后果。研究显示,单纯腹痛与延迟就诊(>24小时)以及更高的睾丸切除术发生率显著相关。2
伴随症状的存在可能有助于在鉴别诊断中确定优先顺序,因为睾丸阑尾或附睾扭转以及附睾炎或睾丸炎更可能表现为单纯性阴囊疼痛。患者很少报告尿痛或疼痛逐渐起病。这些症状应提示临床医生考虑其他诊断,例如附睾炎(无菌性或细菌性)、睾丸炎或尿路感染。
体格检查
应进行腹部和泌尿生殖系统检查。阴囊皮肤可能出现红斑、硬结或温热感。常可见紧张性鞘膜积液,伴阴囊皱褶减少。在肤色较浅且延迟就诊的患者中,呈暗色调的紧张性鞘膜积液可能提示睾丸坏死和/或血鞘膜积液。此类皮肤改变已被证明可预测TT。17
异常的提睾反射提示发生TT的可能性增加。17,18 然而,存在正常的提睾反射并不足以排除TT的诊断。19 同样,提睾反射的缺如对该诊断的特异性并不高。在检查提睾反射时,医务人员应先检查对侧,因为只有在存在对侧反射的情况下,同侧反射的缺如才具有临床意义。临床医生可能会发现患侧睾丸呈水平位(钟锤样畸形)或呈”高位”(由扭转的精索将睾丸抬高至腹股沟管内)。
使用TWIST评分(由Barbosa等于2013年提出)可能使临床医生仅凭体格检查就将患者按TT风险分层为低风险、中等风险和高风险。在确定5项症状是否存在后,计算总分为0-7:睾丸坚硬(2分)、睾丸肿胀,2 提睾反射消失,1 恶心/呕吐,1 以及高位睾丸。120 根据评分算法,高风险患者(评分≥5)对于TT的阳性预测值为100%,因此临床医生可考虑直接进行外科探查,因为CDUS的益处极小。低风险患者(≤2)对于TT的阴性预测值为100%,因此无需CDUS来排除扭转。中等风险患者可通过CDUS确认诊断而获益。一项在非泌尿科的非医师医疗提供者中评估TWIST评分有用性的研究显示,当将高风险定义为>6分、中等风险为1-5分、低风险为0分时,PPV为93.5%,NPV为100%。21 (图4)
表 1 TWIST 评分及风险分层组别。改编自 Barbosa 2013
| 症状 | 分值 |
|---|---|
| 睾丸坚硬 | 2 |
| 睾丸肿胀 | 2 |
| 提睾反射消失 | 1 |
| 高位睾丸 | 1 |
| 恶心和/或呕吐 | 1 |
| 总分 | |
| 高风险 | ≥5 |
| 中等风险 | 3-4 |
| 低风险 | ≤2 |
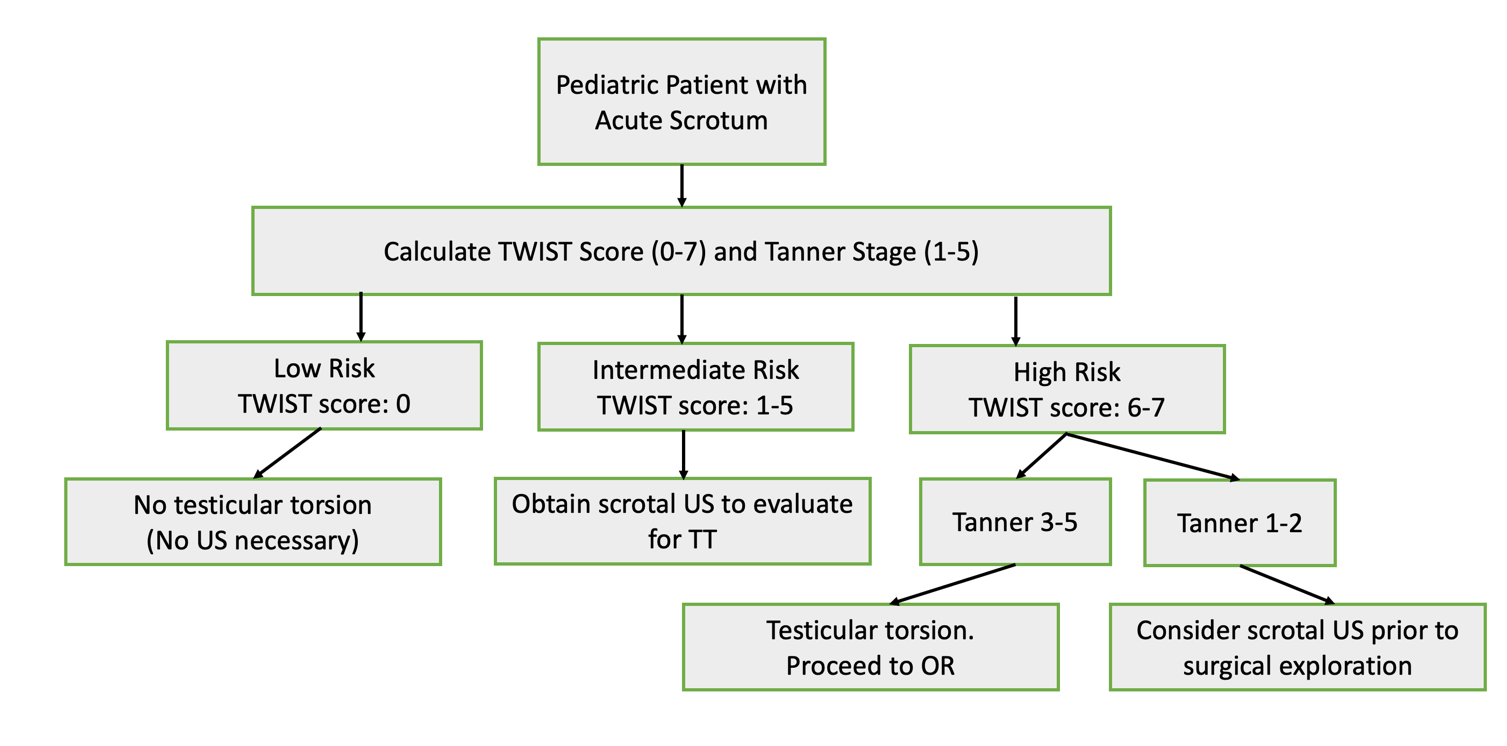
图 4 睾丸扭转的建议处理流程图,改编自 Sheth 2016。值得注意的是,该研究在非泌尿科的非医师提供者中(以模拟急诊室分诊人员)评估了 TWIST 评分的实用性,并且对于低、中、高风险评分采用了不同于 Barbosa 等. 2013 年原始描述的阈值
初步检查
尿液分析(UA)是一种低成本、快速的检测,在急性阴囊疼痛的情境下很有用。它有助于将TT与细菌性附睾炎或尿路感染区分开来,后两者的UA一般可见脓尿。对于TT,UA通常无异常。
影像学
常规使用 存在争议,评估影像检查准确性与实用性的研究不胜枚举。22,23,24 如果根据收集到的病史和体格检查对 TT 的诊断仍不明确,则可以考虑进行影像检查。然而,影像检查不应被用作充分的病史采集和体格检查的替代。不必要的影像检查会延误手术并增加医疗成本。诊断 TT 并不需要影像检查。
彩色多普勒超声检查
CDUS 有助于可视化睾丸解剖结构,包括精索结构、睾丸血流以及睾丸回声纹理。在超声上,睾丸血流减少或消失对于TT的特异性为99%,敏感性为63%。24 作为经验法则,影像学应始终与对侧未受累的一侧进行比较。在TT中,受累睾丸可表现为水肿和增大。当CDUS表现不明确时,临床医生应特别关注双侧睾丸体积的比较,因为这可能是诊断的线索。还可能出现反应性鞘膜积液。25 在无多普勒信号的情况下出现不均匀的回声纹理,很可能提示不可存活的睾丸已开始发生凝固性坏死。
偶尔,在TT患者中可以观察到动脉血流正常或增多,从而产生具有误导性的假阴性结果。一项多中心研究显示,在术前CDUS检查中,24%的已确诊精索扭转病例表现为睾丸血流正常或增多。26 从概念上推测,随着精索发生扭转,睾丸的静脉回流很可能先于动脉流入受到影响。因此,在静脉回流缺失或减少的情况下,动脉血流减少或维持不变可能预示睾丸缺血的起始,且不应被视为令人放心的表现。血流减少可能提示部分或不完全扭转以及精索的间歇性扭转。需要强调的是,多普勒及血管波形的测量高度依赖超声技师,并且在婴儿和幼儿中获取这些参数要困难得多。当病史、体格检查与CDUS结果不一致时,临床医师应对TT的部分或间歇性形式保持高度怀疑。
高分辨率超声检查
与CDUS相比,高分辨率超声(HRUS)是一种更敏感(97.3%)且更特异(99%)的成像方法。26 它能够直接可视化被扭转的精索。研究表明,经过良好训练的超声医师和放射科医师可以通过所谓的“蜗牛样”或“涡旋样”精索征象,准确识别精索的螺旋样盘绕。关于HRUS识别精索“涡旋征”的实用价值,文献中仍存在争议。当在睾丸血流异常的背景下得到正确识别时,这些精索异常可作为正在进行的鞘膜内扭转的确凿证据。然而,对HRUS所见精索异常的一个常见批评是:相关文献在强调这些异常时,未能明确病例的分母,即在TT患儿中有多少人并无可识别的精索改变。换言之,未发现或未报告精索迂曲征象不应排除TT的诊断,且临床医师不应仅凭HRUS上精索的发现作为手术探查的指征。
核素显像
该检查使用静脉注射锝-99m 过锝酸盐来评估睾丸灌注。在 CDUS 之前,闪烁显像是怀疑 TT 时的首选影像学检查。研究报道其敏感性和特异性与 CDUS 相当。27,28 然而,该扫描可能需要数小时才能完成,并不总是容易获得,并且还存在延长睾丸缺血时间的风险。基于这些原因,在现代对 TT 的诊断中很少采用闪烁显像。
治疗选项
TT 需要及时手术矫治。疼痛起始至今的时间(概念上等同于睾丸缺血时间)及精索扭转的程度直接影响睾丸保全率。29,30 经验而言,若在症状出现后的前6小时内进行阴囊探查,睾丸最有可能可存活(>90% 的可能性)。初始6小时窗口之后,睾丸仍可能存活,但概率会急剧下降,这凸显了及时干预的重要性。31 然而,即便在这一时间窗内,患者也可能因缺血损伤而出现一定程度的术后睾丸萎缩。
手法复位
手法复位,即在床旁于阴囊内旋转睾丸,是在等待泌尿科会诊以及急诊手术治疗或转至其他医疗机构期间的初始处理选项。该操作可部分恢复睾丸的血流,并在手术探查时提高睾丸存活的可能性。32,33 手法复位并不能取消手术的必要性,且不应延误手术干预。
在TT手法复位的经典教学中,认为睾丸围绕精索由外侧向内侧方向扭转。为实现手法复位,步骤指导临床医生按相反方向将精索解扭:由内侧向外侧。将睾丸远离中线旋转的动作通常称为”打开书本”。临床医生应以其拇指和食指夹持患侧睾丸,在阴囊内向外朝大腿方向轻柔地将睾丸旋转360度。成功的手法复位通常提示为疼痛立即缓解以及在CDUS上动脉血流恢复。可能需要多次旋转,具体取决于精索扭转的圈数。理想情况下,可使用床旁超声或CDUS客观显示血流的改善。若未能缓解疼痛,或将睾丸从中线向外手法解扭反而加重疼痛,则可尝试通过向内(内侧)旋转来复位。
与这一经典教导相反,回顾性研究表明,他们的TT病例中至少有三分之一是朝外侧方向发生的。29,34 因此,尽管“打开书本”技术在多数情况下可能减轻精索扭转并有望恢复血流,但尝试手法解扭的临床医生需要注意两种可能性:其一,对于发生了多圈旋转的精索,可能解扭不完全;其二,反而会增加旋转的圈数,后者可能加重缺血程度。因此,作者认为,在手术干预可以迅速实施的情况下,不应尝试手法解扭。此外,若诊断存在疑问,或该操作会延误最终的明确手术干预,也不应尝试手法解扭。若实施手法解扭的临床医生并非提供最终明确手术干预者,务必沟通已尝试该操作及其结果。
手术矫正
手术处理包括解扭转和睾丸固定术(将睾丸固定于阴囊下垂侧壁)或患侧睾丸切除术,具体取决于术中检查时器官的活力。在任何一种情况下,鉴于对侧发生钟摆样畸形的概率较高,对侧睾丸的睾丸固定术是标准处理。
手术技术概述:
最常用的是沿阴囊正中缝切口或双侧横行切口。沿阴囊正中缝的切口使得每侧阴囊均可通过单一切口进行探查。
- 阴囊正中切口
- 采用电外科分离,经阴囊肉膜进入患侧半阴囊
- 经阴囊肉膜切口牵出鞘膜
- (对于新生儿扭转病例,检查鞘膜和精索是否存在鞘膜外扭转)
- 切开并翻转鞘膜,以便牵出并检查受累睾丸及附睾。注意是否存在精索的鞘膜内扭转,以及睾丸和附睾的颜色
- 对精索和睾丸进行解扭,记录扭转的方向和度数
- 将解扭后的睾丸用温热纱布垫包裹
- 在对侧半阴囊对阴囊肉膜进行同样的电外科分离,以显露对侧鞘膜和睾丸
- 切开并翻转鞘膜,以便牵出并检查对侧睾丸及附睾。注意是否存在钟锤样畸形
- 返回解扭后的睾丸并再次检查以判断其存活性。若明显不可存活,则行睾丸切除术;若可存活,则行睾丸固定术。这是一种主观评估,在不同术者之间往往存在差异。若存活性仍不明确,可选择进行睾丸微多普勒评估以寻找动脉血流,或在睾丸赤道部行切开,以在释放筋膜室综合征压力后观察到出血和外观健康的曲细精管。若赤道部鞘膜筋膜切开术导致出现鞘膜出血、外观健康的曲细精管以及睾丸颜色总体改善,已有文献描述可采用鞘膜补片增强睾丸白膜。35 (视频 1)
- 对被判定为可存活的患侧睾丸以及正常的对侧睾丸,应将其固定于阴囊内以预防将来再次扭转。睾丸应采用三点固定,可彼此固定(经阴囊中隔,如 “septopexy” 技术),或分别固定在各自半阴囊的低位。作者使用 5-0 聚丙烯(不可吸收)缝线
- 以常规方式关闭阴囊切口(可为单个或多个)。对于因睾丸扭转病程较长、延迟就诊且伴明显水肿而需行睾丸切除术的病例,可留置阴囊引流以帮助预防感染、血囊肿或鞘膜积液的形成
[视频 1](#video-1){:.video-link}. 睾丸扭转的术中管理。在本例中,外科矫治包括应用睾丸鞘膜瓣。注:本视频为美国泌尿外科学会核心课程教育视频库制作并收录。
建议的随访
接受睾丸扭转手术治疗的患者应至少进行一次门诊随访,以确认伤口愈合良好且体格检查无令人担忧的发现。在针对TT尝试进行睾丸解扭转和睾丸固定术之后,临床医生应记录睾丸的大小以及受累睾丸是否存在萎缩。术语“睾丸保留”最好仅用于那些在随访中显示体积保持的受累睾丸。
在随访过程中,作者通常会与患者及其家属讨论以下主题:
- 在对患侧睾丸进行睾丸固定术的情况下,若患者因其他原因再次接受彩色多普勒超声(CDUS),应关注患侧睾丸的外观及血流情况
- 在对患侧睾丸进行睾丸切除术的情况下,青春期完成后可考虑植入睾丸假体
- 尽管理论上复发性睾丸扭转不可能发生,患者仍可能因其他原因感到疼痛或出现异常。患者可能受益于每月自我检查,如出现疼痛或触及异常,应立即告知父母或医生
- 所有患者,尤其是因睾丸扭转(TT)接受睾丸切除术且现仅存单侧睾丸者,应在可能发生接触的运动和娱乐活动中佩戴防护运动护裆。现有现代的纤薄型护裆,可置于舒适的压缩短裤和滑裤中
睾丸附件扭转
睾丸和附睾的上极常可见一个小的相关附属体。睾丸阑尾是副中肾管的胚胎遗迹。附睾阑尾是中肾管系统的胚胎遗迹。上述任一结构都可能绕其轴发生扭转,其方式与鞘内 TT 中精索的扭转相似,导致缺血并最终坏死。其临床表现可模拟 TT,表现为阴囊疼痛和肿胀的骤然起病。然而,在病史和体格检查中,将睾丸附件扭转与 TT 进行比较时,作者凭经验注意到一些关键的相关阴性发现:
- 发生睾丸附件扭转的患者不太可能诉恶心和呕吐。这可能与(相比于睾丸缺血)睾丸附件缺血缺乏内脏感觉有关。
- 发生睾丸附件扭转的患者不太可能出现阴囊内睾丸呈高位
- 发生睾丸附件扭转的患者在彩色多普勒超声(CDUS)上常可见睾丸血流良好,并具有特征性表现:在睾丸旁、与其分离的一个回声不均、无血流信号的小结构36 (参见图 5,为作者收集的代表性图像)
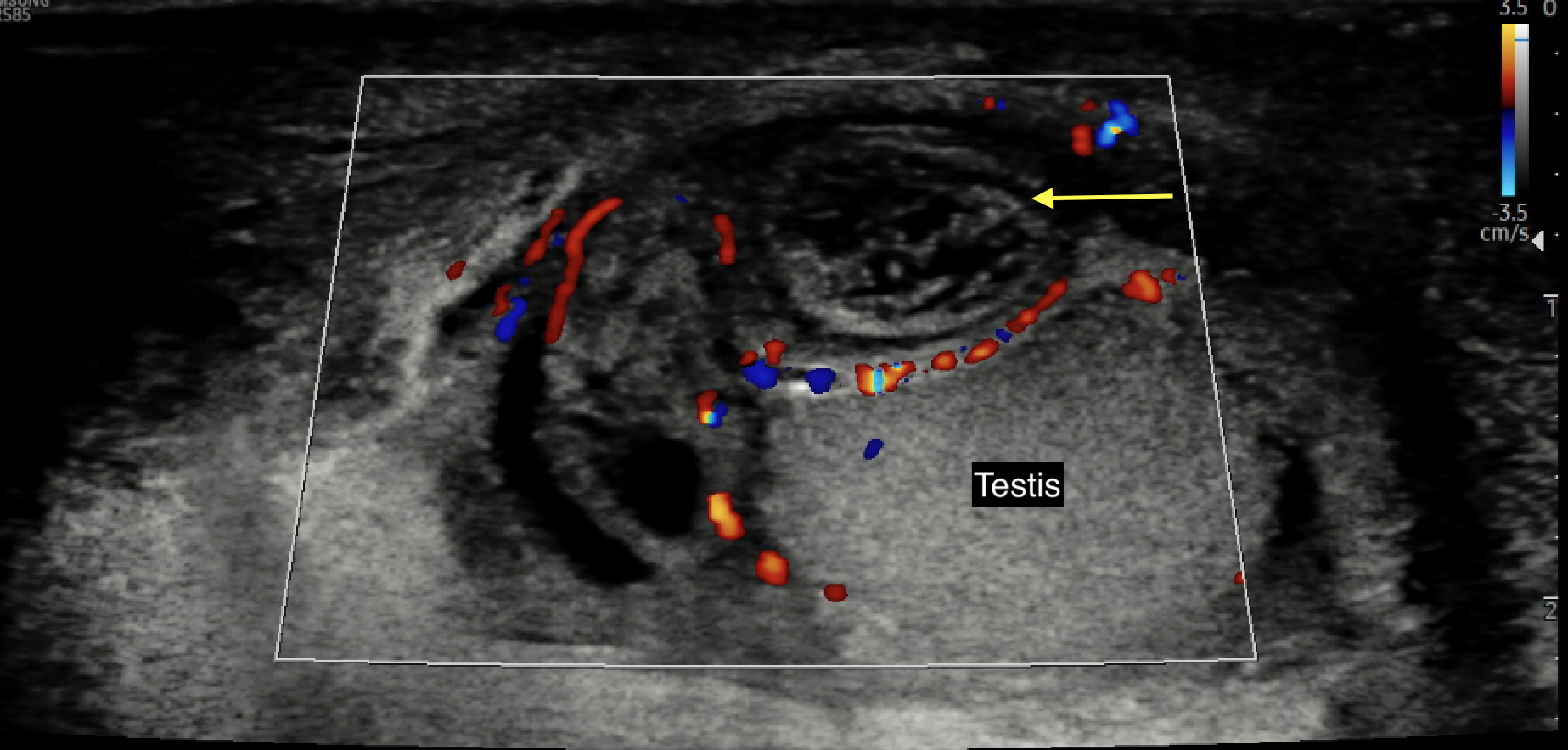
图 5 彩色多普勒超声图像,显示无血流信号、水肿且回声不均质的扭转性睾丸附属体或附睾(黄色箭头)
在体格检查中,睾丸附件扭转通常表现为肿胀、压痛的半侧阴囊。睾丸外观位置多为正常,呈自然下垂位。在皮肤较白皙的个体,偶可在阴囊外侧壁看到“蓝点征”,这是由于透明的鞘膜积液囊使阴囊皮肤变薄,从而可透见缺血的附属体所致。对于能够耐受彻底检查的患者,该点与局灶性压痛相对应。需注意,文献报道蓝点征在睾丸附件扭转病例中的出现率低至约10%,且在皮肤较深色的患者中不易识别。
若诊断存疑或无法排除睾丸缺血,建议行手术探查。在探查时,术者将发现扭转的附属体,而睾丸及附睾其余外观正常(图 6 和 图 7)。可手术切除该附属体并关闭阴囊切口。对于已证实睾丸血流良好、病史与客观资料与TT不一致且更可能为附属体扭转的病例,可延期手术探查。
睾丸附件扭转的治疗以保守为主,包括休息、急性期间歇性冰敷、抬高阴囊以及使用非甾体抗炎药物。作者常规会在疼痛持续时于一周内安排复查阴囊超声以确认诊断,并在疼痛缓解后4-6周复查,以记录初次阴囊超声所见的附件肿物已消退。

图 6 镊子夹持扭转的附睾阑尾
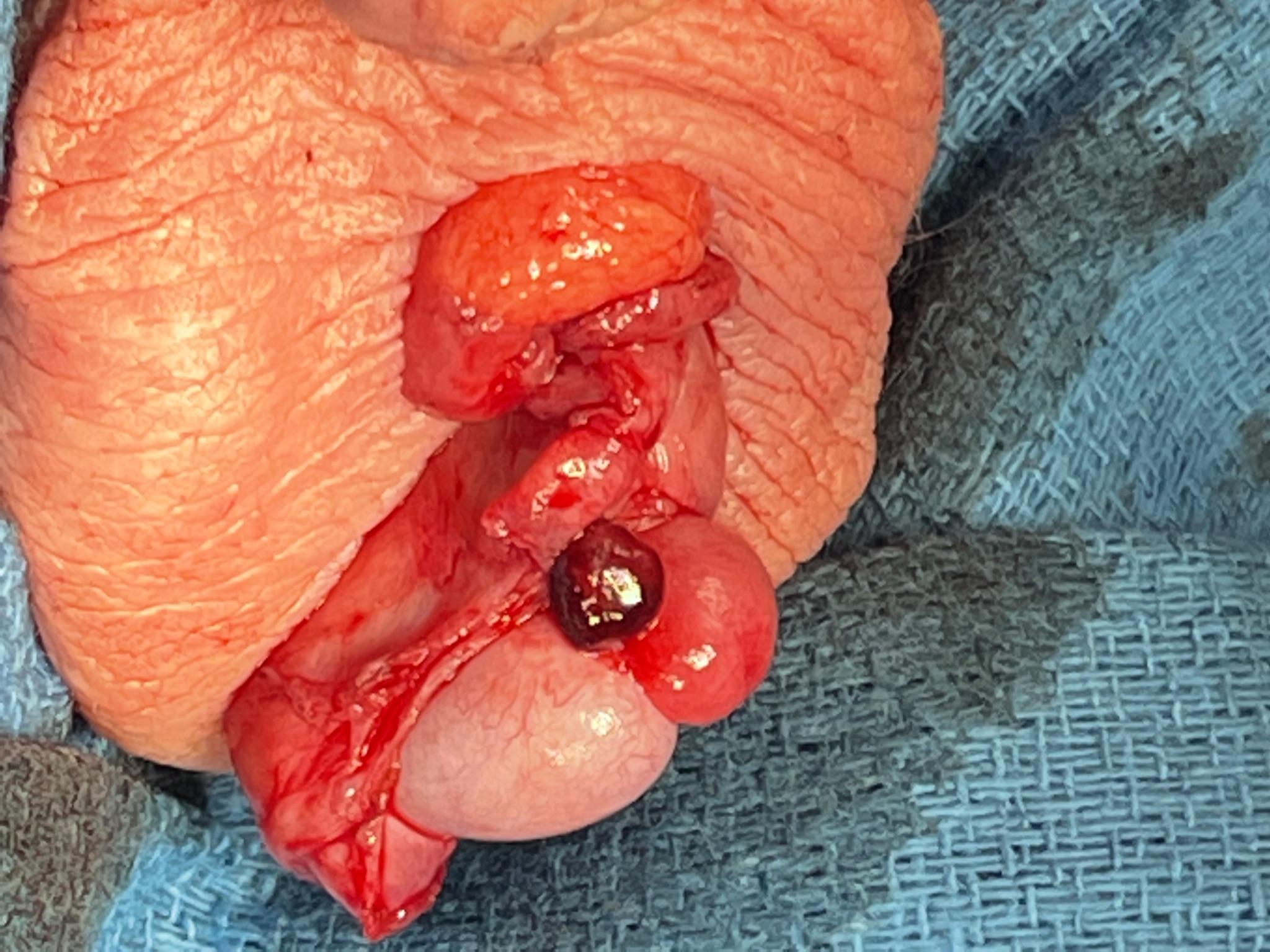
图 7 在被认为针对 TT 的检查结果不明确的情况下,阴囊探查中见充血肿大的附睾阑尾外观
附睾炎
流行病学
附睾炎是附睾的炎症:附睾是一种盘曲的管状结构,位于卵圆形睾丸的后上方。附睾的功能是将来自睾丸的精子输送并使其成熟。在青少年中,附睾炎占急性阴囊疼痛病例的35-71%。37 虽然该病最常见于有性行为的较年长青少年,但也可因病毒感染或化学性(尿液)炎症而发生于更年幼的患者。
发病机制
在年龄较大的患者中,附睾炎最常见地由细菌感染引起。通常,罪魁祸首是性传播感染(STI),这一点在年龄较轻的男性中尤为常见,可导致细菌从尿道迁移至输精管和附睾。Neisseria gonorrhea 和 Chlamydia trachomatis 是该人群中最常见的致病菌。同样,来自尿路感染的受感染尿液可能反流入输精管并引发附睾炎。这种情况可能由提举重物所诱发。
在较小年龄的儿童中,附睾炎最常见的病因为无菌性,继发于高压排尿将“无菌”尿液挤入射精管,并经输精管逆行至附睾(即所谓“无菌性”或“化学性”附睾炎)。其他较少见的病因包括继发于病毒感染(例如有明确命名的病毒,如Paramyxoviridae病毒导致的腮腺炎性睾丸炎,或未命名的病毒)、创伤和结核。
评估与诊断
附睾炎的诊断以临床为主,且常为排除性诊断。对于出现阴囊疼痛逐渐起病、阴囊肿胀,并(可能)伴有发热的患者,应高度怀疑附睾炎。他们还可能报告排尿困难、尿频、尿急、尿失禁和/或尿道分泌物等症状。对于怀疑化学性附睾炎的年幼儿童,应详细询问排尿和便秘史。家长常会反映这些孩子有长时间憋尿,随后出现明显尿急。便秘可能导致男孩在排尿和排便时都需要加压(用力),这两种情况都可使尿液在压力作用下沿射精管和输精管反流。
体格检查应显示睾丸呈正常的垂直位,正常的提睾反射,以及抬高睾丸可缓解疼痛(普雷恩征)。触诊睾丸后方的附睾可引出压痛。
检查评估应包括尿液分析和尿培养。对于病史或体检令人担忧的年龄较大的患儿,可能需要行CDUS以排除TT及其他病变,从睾丸破裂到阴囊脓肿。对于考虑为化学性附睾炎的年幼患儿,1)膀胱超声评估膀胱扩张和/或排尿后残余尿增多,2)腹部平片评估便秘,均可为诊断提供支持。
治疗
治疗方法因人而异,取决于附睾炎的病因。由性传播感染导致的附睾炎的主要治疗是使用合适的抗微生物药物。应同时给予头孢曲松和多西环素以治疗 N. gonorrhea 和 C. trachomatis。对多西环素过敏或存在禁忌的患者,可用阿奇霉素替代。其他支持治疗包括使用非甾体抗炎镇痛药和阴囊支托。性伴侣也应接受评估并用抗生素治疗。幼儿化学性附睾炎的治疗包括支持治疗,即按时使用非甾体抗炎镇痛药并穿着具有支撑作用的内裤。还需要同时处理憋尿、增加腹压排尿和便秘。
结论
总之,”急性阴囊”是用于描述阴囊疼痛或肿胀快速起病的临床术语。鉴别诊断包括但不限于睾丸扭转、睾丸阑尾扭转和附睾炎。在开展其他病因学评估之前,应首先排除睾丸扭转。
关键要点
- 睾丸扭转(TT)的发病率呈双峰分布:生命的第一年(~1月龄),此时扭转更可能为鞘外;以及青春期(~12岁),此时扭转更可能为鞘内
- 钟锤畸形是促发鞘内扭转的主要危险因素
- TT 为临床诊断: 有针对性的病史采集和体格检查是进行手术探查的唯一先决条件
- 在临床表现不明确的情况下,可使用彩色多普勒超声(CDUS)来确认终末器官缺血
- CDUS 显示存在血流并不一定能排除进行性缺血
- 若影像学检查会显著延误手术探查和确定性治疗,则不应进行影像学检查
- 警惕孤立性腹痛,并记得进行泌尿生殖系统检查。男性儿童仅以腹痛为唯一主诉与延迟就诊(>24小时)和更高的睾丸切除术发生率显著相关
参考文献
- Jefferies MT, Cox AC, Gupta A, Proctor A. The management of acute testicular pain in children and adolescents. Bmj 2015; 350 (apr02 5): h1563–h1563. DOI: 10.1136/bmj.h1563.
- Bayne CE, Villanueva J, Davis TD, Pohl HG, Rushton HG. Factors Associated with Delayed Presentation and Misdiagnosis of Testicular Torsion: A Case-Control Study. J Pediatr 2017; 186: 200–204. DOI: 10.1016/j.jpeds.2017.03.037.
- McCombe AW, Scobie WG. Torsion of Scrotal Contents in Children. J Urol 1988; 140 (1): 214–214. DOI: 10.1016/s0022-5347(17)41551-5.
- Kadish HA, Bolte RG. A Retrospective Review of Pediatric Patients With Epididymitis, Testicular Torsion, and Torsion of Testicular Appendages. Pediatrics 1998; 102 (1): 73–76. DOI: 10.1542/peds.102.1.73.
- Caesar RE, Kaplan GW. The Incidence of the Cremasteric Reflex in Normal Boys. J Urol 1994; 152 (2 Part 2): 779–780. DOI: 10.1016/s0022-5347(17)32707-6.
- Bingöl-Koloğlu M, Tanyel FC, Anlar B, Büyükpamukçu N. Cremasteric reflex and retraction of a testis. J Pediatr Surg 2001; 36 (6): 863–867. DOI: 10.1053/jpsu.2001.23956.
- Williamson RCN. Torsion of the testis and allied conditions. Br J Surg 1976; 63 (6): 465–476. DOI: 10.1002/bjs.1800630618.
- Zhao LC, Lautz TB, Meeks JJ, Maizels M. Pediatric Testicular Torsion Epidemiology Using a National Database: Incidence, Risk of Orchiectomy and Possible Measures Toward Improving the Quality of Care. J Urol 2011; 186 (5): 2009–2013. DOI: 10.1016/j.juro.2011.07.024.
- Mano R, Livne PM, Nevo A, Sivan B, Ben-Meir D. Testicular Torsion in the First Year of Life – Characteristics and Treatment Outcome. Urology 2013; 82 (5): 1132–1137. DOI: 10.1016/j.urology.2013.07.018.
- Mathews John C, Kooner G, Mathew DE, Ahmed S, Kenny SE. Neonatal testicular torsion – a lost cause? Acta Paediatr 2008; 97 (4): 502–504. DOI: 10.1111/j.1651-2227.2008.00701.x.
- Taghavi K, Dumble C, Hutson JM, Mushtaq I, Mirjalili SA. The bell-clapper deformity of the testis: The definitive pathological anatomy. J Pediatr Surg 2021; 56 (8): 1405–1410. DOI: 10.1016/j.jpedsurg.2020.06.023.
- Caesar RE, Kaplan GW. Incidence of the bell-clapper deformityin an autopsy series. Urology 1994; 44 (1): 114–116. DOI: 10.1016/s0090-4295(94)80020-0.
- Martin AD, Rushton HG. The Prevalence of Bell Clapper Anomaly in the Solitary Testis in Cases of Prior Perinatal Torsion. J Urol 2014; 191 (5s): 1573–1577. DOI: 10.1016/j.juro.2013.09.013.
- O’Kelly F, Chua M, Erlich T, Patterson K, DeCotiis K, Koyle MA. Delaying Urgent Exploration in Neonatal Testicular Torsion May Have Significant Consequences for the Contralateral Testis: A Critical Literature Review. Urology 2021; 153: 277–284. DOI: 10.1016/j.urology.2020.10.064.
- Erlich T, Ghazzaoui AE, Pokarowski M, O’Kelly F, Lorenzo AJ, Bagli DJ, et al.. Perinatal testicular torsion: The clear cut, the controversial, and the "quiet" scenarios. J Pediatr Surg 2021; 57 (10): 288–297. DOI: 10.1016/j.jpedsurg.2021.10.003.
- Bayne CE, Hsieh MH. Testicular Torsion. In: Cabana MD, editor. The 5-minute Pediatric Consult. 8th. DOI: 10.1016/b978-0-323-47778-9.50163-x.
- Srinivasan A, Cinman N, Feber KM, Gitlin J, Palmer LS. Faculty Opinions recommendation of History and physical examination findings predictive of testicular torsion: an attempt to promote clinical diagnosis by house staff. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2011; 7: 470–474. DOI: 10.3410/f.11135959.12106058.
- Boettcher M, Bergholz R, Krebs TF, Wenke K, Aronson DC. Clinical Predictors of Testicular Torsion in Children. Urology 2012; 79 (3): 670–674. DOI: 10.1016/j.urology.2011.10.041.
- Beni-Israel T, Goldman M, Bar Chaim S, Kozer E. Clinical predictors for testicular torsion as seen in the pediatric ED. Am J Emerg Med 2010; 28 (7): 786–789. DOI: 10.1016/j.ajem.2009.03.025.
- Barbosa JA, Tiseo BC, Barayan GA. Development and Initial Validation of a Scoring System to Diagnose Testicular Torsion in Children. Yearbook of Urology 2013; 2013: 6–7. DOI: 10.1016/j.yuro.2013.06.025.
- Sheth KR, Keays M, Grimsby GM, Granberg CF, Menon VS, DaJusta DG, et al.. Diagnosing Testicular Torsion before Urological Consultation and Imaging: Validation of the TWIST Score. J Urol 2016; 195 (6): 1870–1876. DOI: 10.1016/j.juro.2016.01.101.
- Jefferson RH, Perez LM, Joseph DB. Critical Analysis of the Clinical Presentation of Acute Scrotum: A 9-Year Experience at a Single Institution. J Urol 1997; 158 (3): 1198–1200. DOI: 10.1016/s0022-5347(01)64426-4.
- Friedman N, Pancer Z, Savic R, Tseng F, Lee MS, Mclean L, et al.. Accuracy of point-of-care ultrasound by pediatric emergency physicians for testicular torsion. J Pediatr Urol 2019; 15 (6): 608.e1–608.e6. DOI: 10.1016/j.jpurol.2019.07.003.
- Karmazyn B, Steinberg R, Kornreich L, Freud E, Grozovski S, Schwarz M, et al.. Clinical and sonographic criteria of acute scrotum in children: a retrospective study of 172 boys. Pediatr Radiol 2005; 35 (3): 302–310. DOI: 10.1007/s00247-004-1347-9.
- Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol 2018; 48 (5): 735–744. DOI: 10.1007/s00247-018-4093-0.
- Kalfa N, Veyrac C, Lopez M, Lopez C, Maurel A, Kaselas C, et al.. Multicenter Assessment of Ultrasound of the Spermatic Cord in Children With Acute Scrotum. J Urol 2007; 177 (1): 297–301. DOI: 10.1016/j.juro.2006.08.128.
- NUSSBAUM BLASK ANNAR, BULAS DOROTHY, SHALABY-RANA EGLAL, RUSHTON GIL, SHAO CHENG, MAJD MASSOUD. Color Doppler sonography and scintigraphy of the testis: A prospective, comparative analysis in children with acute scrotal pain. Pediatr Emerg Care 2002; 18 (2): 67–71. DOI: 10.1097/00006565-200204000-00001.
- Paltiel HJ, Connolly LP, Atala A, Paltiel AD, Zurakowski D, Treves ST. Acute Scrotal Symptoms in Boys With an Indeterminate Clinical Presentation: Comparison of Color Doppler Sonography and Scintigraphy. J Urol 1998; 161 (4): 1408–1408. DOI: 10.1016/s0022-5347(01)61728-2.
- SESSIONS ANNETTEE, RABINOWITZ RONALD, HULBERT WILLIAMC, GOLDSTEIN MARTINM, MEVORACH ROBERTA. Testicular Torsion: Direction, Degree, Duration and Disinformation. J Urol 2003; 169: 663–665. DOI: 10.1097/00005392-200302000-00059.
- Castañeda-Sánchez I, Tully B, Shipman M, Hoeft A, Hamby T, Palmer BW. Testicular torsion: A retrospective investigation of predictors of surgical outcomes and of remaining controversies. J Pediatr Urol 2017; 13 (5): 516.e1–516.e4. DOI: 10.1016/j.jpurol.2017.03.030.
- Mellick LB, Sinex JE, Gibson RW, Mears K. A Systematic Review of Testicle Survival Time After a Torsion Event. Pediatr Emerg Care 2019; Publish Ahead of Print: 821–825. DOI: 10.1097/pec.0000000000001287.
- Dias Filho AC, Oliveira Rodrigues R, Riccetto CLZ, Oliveira PG. Improving Organ Salvage in Testicular Torsion: Comparative Study of Patients Undergoing vs Not Undergoing Preoperative Manual Detorsion. J Urol 2017; 197 (3 Part 1): 811–817. DOI: 10.1016/j.juro.2016.09.087.
- Garel L, Dubois J, Azzie G, Filiatrault D, Grignon A, Yazbeck S. Preoperative manual detorsion of the spermatic cord with Doppler ultrasound monitoring in patients with intravaginal acute testicular torsion. Pediatr Radiol 2000; 30 (1): 41–44. DOI: 10.1007/s002470050012.
- Yecies T, Bandari J, Schneck F, Cannon G. Direction of Rotation in Testicular Torsion and Identification of Predictors of Testicular Salvage. Urology 2018; 114: 163–166. DOI: 10.1016/j.urology.2017.11.034.
- Kutikov A, Casale P, White MA, Meyer WA, Chang A, Gosalbez R, et al.. Testicular Compartment Syndrome: A New Approach to Conceptualizing and Managing Testicular Torsion. Urology 2008; 72 (4): 786–789. DOI: 10.1016/j.urology.2008.03.031.
- Lev M, Ramon J, Mor Y, Jacobson JM, Soudack M. Sonographic appearances of torsion of the appendix testis and appendix epididymis in children. J Clin Ultrasound 2015; 43 (8): 485–489. DOI: 10.1002/jcu.22265.
- Lehmann C, Biro FM, Slap GB. Chapter 20 - Testicular and Scrotal Disorders. Adolescent Medicine. Philadelphia: Mosby; 2008.
最近更新时间: 2025-09-22 08:00