
43: 膀胱恶性肿瘤
阅读本章大约需要 5 分钟。
引言
尿路上皮癌(UCC)在儿科人群中极为罕见,发病率约为0.1%-0.4%。2019年一项综述仅发现年龄<18岁的患者中有记录的UCC病例243例,平均年龄为12.5岁,且男性占优势(3:1)。总体而言,儿科人群UCC的复发率被认为较低(8.6%),死亡非常罕见,<4%。鉴于其罕见性,目前尚无关于儿科人群UCC诊断与治疗的已发表指南。本章旨在基于目前已发表的文献,概述儿科UCC的病因与发病机制、评估与诊断、治疗及随访。
病因/发病机制
成人尿路上皮癌(UCC)的发生有明确的危险因素,包括吸烟、接触各种工作场所化学物质(如苯胺染料和纺织厂化学品)、非那西汀,以及接受化疗或放疗。遗传性疾病也与成人膀胱UCC的发生有关,包括林奇综合征、考登病,以及一级亲属患有UCC。在儿童中,遗传和环境危险因素尚缺乏充分研究,多由成人数据外推。早期烟草暴露、肿瘤易感综合征(如科斯特洛综合征)、膀胱发育异常、放射暴露、环磷酰胺暴露以及寄生虫感染已被认为是儿童UCC发生的可归因危险因素。尽管如此,近87%的儿科UCC患者可能并无明显的已知危险因素。
在儿科人群中,复发和与膀胱癌相关的死亡的危险因素包括UCC的家族史、高级别组织学,以及诊断时肿瘤较大。复发和死亡较为罕见,因此,这些因素通常是从成人文献中外推而来。
评估与诊断
患者表现
与成人相似,儿童患者常表现为无痛性肉眼血尿(90%),尽管尿痛、尿频、尿急等刺激性排尿症状也较为常见。鉴于该诊断在儿童中较为罕见,且儿童肉眼血尿的鉴别诊断多为良性(例如良性尿道溢血、外伤、尿路感染、先天性泌尿系统畸形、肾实质疾病、排尿功能障碍等),已有报道多达26%的患者其诊断被延误至少1年。
UCC在儿童中通常表现为单发膀胱肿瘤,而在成人更常见为多灶性(94% vs. 6%)。93.4%的肿瘤为低级别(pTa 或 pT1),且通常无淋巴结受累或转移的证据。表 1 概述了美国癌症联合委员会(AJCC)膀胱癌分期。
表 1 AJCC 尿路上皮细胞癌分期
| T stage | Description |
|---|---|
| Ta | 非浸润性乳头状癌 |
| Tis | 原位癌(CIS) |
| T1 | 肿瘤侵及固有层 |
| T2 | 肿瘤侵及固有肌层 |
| T2a | 肿瘤侵及固有肌层浅层(内半) |
| T2b | 肿瘤侵及固有肌层深层(外半) |
| T3 | 肿瘤侵及膀胱周围组织/脂肪 |
| T3a | 肿瘤在显微镜下侵及膀胱周围组织/脂肪 |
| T3b | 肿瘤以肉眼可见方式侵及膀胱周围脂肪组织(膀胱外肿块) |
| T4 | 肿瘤侵及前列腺、子宫、阴道、盆壁或腹壁 |
| T4a | 肿瘤侵及邻近器官(子宫、卵巢、前列腺间质) |
| T4b | 肿瘤侵及盆壁和/或腹壁 |
初始评估
2020年AUA关于非肌层浸润性尿路上皮癌(UCC)的指南对成人肉眼血尿的评估提出了明确建议,包括行膀胱镜检查、通过CT或MR尿路造影进行上尿路影像学评估,以及在某些情况下使用尿细胞学检查。鉴于UCC在儿科患者中的自然病程——即通常为不复发的低级别肿瘤——对出现肉眼血尿的儿科患者的初始检查往往采取较为保守的策略。
评估应从病史采集和体格检查开始。首次就诊可进一步进行的检查手段包括尿液分析(特别关注红细胞的存在/数量以及感染指标,如白细胞酯酶、亚硝酸盐和细菌)、尿培养,以及膀胱/肾脏超声检查。
尿液分析可确认持续存在的镜下血尿,并有助于排除血尿的其他潜在原因,包括内科性肾脏疾病或感染。尿培养可证实不存在感染。膀胱/肾脏超声可明确上、下尿路的解剖结构,并评估肉眼血尿的潜在病因。鉴于儿童体型较小,该检查在检测小的腔内肿瘤方面具有很高的敏感性。
影像学检查、膀胱镜检查与细胞学检查
在成人人群中,膀胱镜检查是检测膀胱肿瘤的金标准,而CT或MR尿路造影是对上尿路进行成像的标准方法。在儿科人群中,需要权衡一些因素,包括膀胱镜检查需全身麻醉、进行CT或MRI成像需镇静,以及CT的辐射暴露。
已有少数研究评估了超声在儿童上、下尿路肿块检测中的敏感性和特异性。研究发现,膀胱超声在检测膀胱肿瘤方面的敏感性为83–93%,特异性为93–100%,并可检出小至5mm的膀胱病变。考虑到儿科患者在多年UCC监测过程中可能累积的辐射剂量,超声成为一种颇具吸引力的检查方式,既可在以肉眼血尿就诊时作为初筛检测,也可用于切除后肿块复发的监测。
膀胱镜检查适用于在超声检查中发现膀胱病变的患者,或无其他解释的持续性血尿患者。在儿童患者中,肿瘤通常为单发、非浸润性,且约52%位于膀胱侧壁 (图 1) 儿童行膀胱镜检查需要麻醉,因此常将膀胱镜检查与经尿道膀胱肿瘤切除术(TURBT)一并实施,作为该手术预期的一部分。需要获取组织以确立诊断并评估浸润深度(T分期)。这也是去除整个肿瘤的初始治疗。
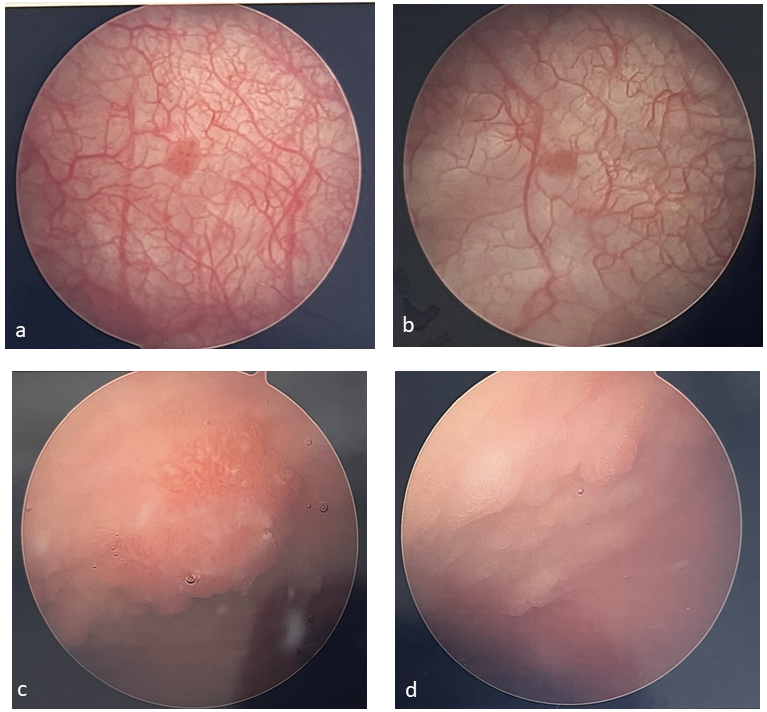 图 1 膀胱肿瘤示例。膀胱肿瘤常为单发且呈乳头状(a、b),在接受过膀胱扩大术的患者中(c、d)更难识别。
图 1 膀胱肿瘤示例。膀胱肿瘤常为单发且呈乳头状(a、b),在接受过膀胱扩大术的患者中(c、d)更难识别。
在儿科患者中,尿细胞学的临床价值极有限,因为这些膀胱肿瘤通常为低级别,而细胞学对低级别肿瘤的敏感性相当低。
处理
儿童人群中的膀胱癌复发率较低,5年生存率良好,为97.3%。由于这些差异,其管理与成人显著不同。然而,两类人群之间也存在一些相似之处,因此在管理方面亦有一些共同点。
经尿道膀胱肿瘤切除术(TURBT)
与成人相同,经尿道切除术既具有诊断意义,也具有治疗意义。该操作需要切除所有肉眼可见的肿瘤,并达到足够深度以取得下方逼尿肌的取样。这对于降低复发风险是必要的,同时也有助于充分分期。对于体型较小的患儿,需使用电切镜的TURBT手术可能难以实施,因为在小口径镜鞘上操作电切袢非常具有挑战性。部分患儿可能需要进行冷杯活检并对肿瘤基底进行电灼,但须注意获取深层组织活检以进行逼尿肌取样。在进行TURBT时还应对膀胱进行双合诊,以完成分期。
膀胱内治疗
总体而言,围手术期化疗灌注一般不用于儿童患者。被发现具有更高级别和分期肿瘤的儿童患者,其表现更可能类似于成人UCC,因此可能最好按此进行治疗,尽管关于这种罕见情形的前瞻性研究尚不存在。这些患者可能需要采用由AUA和NCCN组织为成人制定的膀胱内化疗和随访监测方案。有一些报道描述膀胱癌儿童患者在TURBT术后进行膀胱内灌注BCG、丝裂霉素或表柔比星。总体而言,所用剂量和方案与成人所述一致,严重不良事件较少。膀胱内治疗通常仅保留用于高级别或复发性疾病患者,但数据仅限于病例报告,因此目前没有明确数据来确立其明确定义的作用。
随访与监测
成人指南因复发常见,已制定了积极、明确且成熟的监测与复发管理方案。然而在儿童中,由于该肿瘤罕见且复发更为罕见,目前尚无明确建议。2019年的一项综述报告显示复发率仅为8.6%,与成人相比差异显著。
总体而言,监测的类型和时机应根据儿童的复发风险进行个体化调整。应综合考虑病灶数目、病理分期与分级、肿瘤大小、复发史以及年龄。对于已确诊膀胱癌的儿童,因超声具备高敏感性且为无创检查,进行定期超声筛查是合理的选择。如发现病灶,可随后行膀胱镜检查。对于高风险儿科患者(如多发病灶、高级别病灶、复发、年龄较大等),即便超声结果正常,仍可能需要常规的随访性膀胱镜检查。与诊断时相似,鉴于儿童通常为低级别、分化良好的肿瘤,尿细胞学的收益可能有限。
与成人方案不同,目前缺乏用于指导UCC患儿随访监测时长的数据。一项大型文献综述发现,如果发生与低级别/低分期UCC相关的复发或死亡,最有可能在初次确诊后的第一年内出现。复发或死亡的平均时间为8.6个月。
表 2 儿科患者低级别、低分期膀胱尿路上皮癌(UCC)的随访时间表(由 Rezaee 等人 改编)1
| 0-12 个月 | 18-24 个月 | 36-48 个月 | >60 个月 | |
|---|---|---|---|---|
| 超声检查 | 每3个月 | 每6个月 | 每年 | 由医疗服务提供者酌情决定 |
| 尿常规检查 | 每3个月 | 每6个月 | 每年 | 由医疗服务提供者酌情决定 |
| 膀胱镜检查 | 每3个月 | 每6个月 | 可选择每年一次 | 由医疗服务提供者酌情决定 |
| 细胞学检查 | — | — | — | — |
此外,在初始诊断和治疗后三年以后发生复发或死亡事件的可能性极低。已发表的最远期复发发生在初始诊断后32个月。基于2019年文献回顾队列,Rezaee 等人 概述了一个针对低级别、低分期 UCC 的潜在随访监测计划,并在表 2中进行了总结。需要注意,这一随访计划尚未通过前瞻性随机研究得到严格的安全性验证,且仅作为低级别/低分期疾病的起始参考。
神经源性膀胱人群中的膀胱肿瘤
对先天性神经源性膀胱(如脊柱裂、膀胱外翻等)患者的长期随访发现,该人群发生膀胱癌的风险显著增高(估计发生率约为4%)。与非神经源性膀胱人群的膀胱癌不同,该队列通常在偶然情况下被诊断,且腺癌的发生比例更高(50%)。绝大多数患者就诊时已属局部进展期或广泛播散性疾病(>70%),生存率较差。诊断往往在疾病晚期才确立,结局不佳。
对于膀胱癌风险增加的最初假设,主要认为膀胱扩大成形术是一个危险因素。尽管使用胃段确实会增加随后发生恶性肿瘤的风险,但采用其他肠段进行膀胱扩大似乎并不会增加恶性肿瘤风险。通过多项回顾性研究,现在看来,恶性肿瘤的风险源于先天性膀胱异常本身,而非源于扩大手术。
当最初有关该人群中晚期、致命性恶性肿瘤的描述发表时,曾提出并研究了多种措施,旨在更早发现这些肿瘤。不幸的是,没有一种被证明有益。每年进行膀胱镜检查的检出率很低,即便筛查结果正常的患者也会发生晚期膀胱癌。有人提出,若膀胱镜能检测到所有恶性肿瘤,在10年随访期间需要进行980次检查才能诊断出1例癌症。由于慢性脓尿、间歇性导尿以及预期的肠源性细胞脱落,该人群的尿细胞学价值不大,且假阳性率很高。当将上述筛查措施的有效性纳入考虑后,预期寿命的增加仅为2.3个月,而人均终身费用为>$55,000。这主要是由于恶性肿瘤发生率低,以及为发现单例恶性肿瘤所需的筛查次数极多所致,且这一结果与诊断时的分期无关。
Husmann 方案已被广泛采用,用于指导神经源性膀胱患者的随访,既用于恶性肿瘤检测,也用于对已行或未行膀胱重建患者的常规评估(图2) 其内容包括每年评估尿路感染、血尿、膀胱/盆腔/肋区疼痛以及新发失禁。若出现任何异常或较基线的变化,应考虑进行尿培养、膀胱镜检查、CT扫描 ± 尿动力学检查。所有患者每年应检测肌酐/胱抑素C、电解质、血清维生素B12水平,并进行尿液分析。类似地,若有 <50 RBCs/hpf,应开具肾脏/膀胱超声检查。若超声异常,或有肉眼血尿或 ≥50 RBCs/hpf,则应考虑进行尿培养、膀胱镜检查、CT扫描 ± 尿动力学检查。 对含结肠段的患者,结肠癌筛查的常规膀胱镜检查应从50岁开始。

图 2 用于膀胱扩大术患者膀胱癌监测的 Husmann 方案。2
要点
- 儿科患者中膀胱癌很罕见
- 目前尚无明确的儿童膀胱癌发生危险因素,但常将成人的危险因素外推并应用于该人群
- 大多数儿童膀胱癌患者以无痛性肉眼血尿或刺激性排尿症状就诊
- 大多数儿科UCC为低级别、低分期,且不复发
- 初始评估应从病史与体格检查、尿常规、尿培养以及膀胱/肾脏超声开始
- 膀胱超声在检测膀胱肿瘤方面具有极佳的敏感性和特异性,应作为一种筛查手段予以考虑
- 由于大多数儿科UCC为低级别,尿液细胞学没有应用价值
- 若超声发现病灶,应行膀胱镜检查并实施TURBT
- 经尿道膀胱肿瘤切除应包括逼尿肌取样以便准确分期
- 膀胱内化疗的作用尚不明确,但对于高分期、高级别或复发患者可以合理考虑
- 诊断后至少前3年应对儿科UCC患者进行随访监测,但超过此时间的监测可能没有必要
- 先天性神经源性膀胱(CNB)患者罹患膀胱癌的风险更高,且除胃段膀胱扩大外,该风险与膀胱扩大术无关;病理多为腺癌
- CNB患者常为偶然发现,且多为更高分期和局部进展期肿瘤,生存率较差
- 常规以膀胱镜和尿液细胞学进行筛查无益,不予推荐
- 推荐对CNB患者随访采用Husmann方案,旨在有针对性地识别恶性风险更高的患者(血尿、尿路感染增多、疼痛、新发尿失禁、实验室/影像学异常)
结论
儿童患者的膀胱癌较为罕见,整体预后良好。大多数肿瘤为单发、低级别,且不复发。诊断评估应从病史及体格检查、尿常规、尿培养和膀胱/肾脏超声开始,随后行膀胱镜检查并对膀胱病灶进行经尿道膀胱肿瘤切除术(TURBT)。鉴于病理多为低级别,通常可避免行膀胱内灌注化疗。对于高级别或分期较高的肿瘤,或复发性肿瘤,可以考虑膀胱内灌注化疗;然而,目前尚无关于其在儿童中应用的循证指南。应通过定期尿常规、膀胱/肾脏超声及膀胱镜相结合的方式,随访至少3年。超过3年的随访可能并非必要,但应采用医患共同决策来确定这一时长。
推荐视频
参考文献
- Karatzas A, Tzortzis V. Lower urinary tract symptoms and bladder cancer in children: The hidden scenario. Urol Ann 2019; 11 (1): 102–104. DOI: 10.4103/UA.UA_60_18.
- Rezaee ME, Dunaway CM, Baker ML, Penna FJ, Chavez DR. Urothelial cell carcinoma of the bladder in pediatric patients: a systematic review and data analysis of the world literature. Journal of Pediatric Urology 2019; 15 (4): 309–314. DOI: 10.1016/j.jpurol.2019.06.013.
- Lerena J, Krauel L, García-Aparicio L, Vallasciani S, Suñol M, Rodó J. Transitional cell carcinoma of the bladder in children and adolescents: Six-case series and review of the literature. Journal of Pediatric Urology 2010; 6 (5): 481–485. DOI: 10.1016/j.jpurol.2009.11.006.
- Egbers L, Grotenhuis AJ, Aben KK, Alfred Witjes J, Kiemeney LA, Vermeulen SH. The prognostic value of family history among patients with urinary bladder cancer. Int J Cancer 2015; 136 (5): 1117–1124. DOI: 10.1002/ijc.29062.
- Wild P, Giedl J, Stoehr R. Genomic aberrations are rare in urothelial neoplasms of patients 19 years or younger. The Journal of Pathology 2007; 211 (1): 18–25. DOI: 10.1002/path.2075.
- Fine SW, Humphrey PA, Dehner LP, Amin MB, Epstein JI. Urothelial Neoplasms In Patients 20 Years or Younger: A Clinicopathological Analysis Using The World Health Organization 2004 Bladder Consensus Classification. Journal of Urology 2005; 174 (5): 1976–1980. DOI: 10.1097/01.ju.0000176801.16827.82.
- Paner GP, Zehnder P, Amin AM, Husain AN, Desai MM. Urothelial Neoplasms of the Urinary Bladder Occurring in Young Adult and Pediatric Patients: A Comprehensive Review of Literature With Implications for Patient Management. Adv Ant Pathol 18 (1): 79–89.
- Bladder Cancer: Non-Muscle Invasive Guideline - American Urological Association. .
- Gharibvand MM, Kazemi M, Motamedfar A, Sametzadeh M, Sahraeizadeh A. The role of ultrasound in diagnosis and evaluation of bladder tumors. J Family Med Prim Care 2017; 6 (4): 840–843. DOI: 10.4103/jfmpc.jfmpc_186_17.
- Berretini A, Castagnetti M, Salerno A. Bladder urothelial neoplasms in pediatric age: Experience at three tertiary centers. Journal of Pediatric Urology 2015; 11: 26 1–26 5. DOI: 10.1016/j.jpurol.2014.08.008.
- D DC, A F, K P. Management and follow-up of urothelial neoplasms of the bladder in children: A report from the TREP project. Pediatric Blood & Cancer 2015; 62 (6): 1000–1003. DOI: 10.1002/pbc.25380.
- ElSharnoby O, Fraser N, Williams A, Scriven S, Shenoy M. Bladder urothelial cell carcinoma as a rare cause of haematuria in children: Our experience and review of current literature. Journal of Pediatric Surgery Published Online September 2021; 17. DOI: 10.1016/j.jpedsurg.2021.09.007.
- Saltsman JA, Malek MM, Reuter VE. Urothelial neoplasms in pediatric and young adult patients: A large single-center series. Journal of Pediatric Surgery 2018; 53 (2): 306–309. DOI: 10.1016/j.jpedsurg.2017.11.024.
- Rague JT, High-grade LRSM. Nonmuscle Invasive Urothelial Carcinoma in a Prepubertal Patient With TURBT and Intravesical BCG. Urology 2019; 124: 257–259. DOI: 10.1016/j.urology.2018.10.028.
- Peard L, Stark T, Ziada A, Saltzman AF. Recurrent Bladder Cancer in a Teenage Male. Urology 2020; 141: 135–138. DOI: 10.1016/j.urology.2020.04.031.
- Soergel TM, Cain MP, Misseri R, Gardner TA, Koch MO, Rink RC. TRANSITIONAL CELL CARCINOMA OF THE BLADDER FOLLOWING AUGMENTATION CYSTOPLASTY FOR THE NEUROPATHIC BLADDER. The Journal of Urology 2004; 172 (4, Supplement): 1649–1652. DOI: 10.1097/01.ju.0000140194.87974.56.
- Austin JC, Elliott S, Cooper CS. Patients With Spina Bifida and Bladder Cancer: Atypical Presentation, Advanced Stage and Poor Survival. The Journal of Urology 2007; 178 (3): 798–801. DOI: 10.1016/j.juro.2007.05.055.
- Rove K, Higuchi T. Monitoring and malignancy concerns in patients with congenital bladder anomalies. Current Opinion in Urology 2016; 26 (4): 344–350. DOI: 10.1097/MOU.0000000000000297.
- Husmann D, Fox J, Higuchi T. Malignancy following bladder augmentation:recommendations for long-term follow-up and cancer screening. AUA Update Ser 2011; 30 (24): 222–227.
- Higuchi TT, Fox JA, Husmann DA. Annual Endoscopy and Urine Cytology for the Surveillance of Bladder Tumors After Enterocystoplasty for Congenital Bladder Anomalies. The Journal of Urology 2011; 186 (5): 1791–1795. DOI: 10.1016/j.juro.2011.07.028.
- Hamid R, Greenwell TJ, Nethercliffe JM, Freeman A, Venn SN, Woodhouse CRJ. Routine surveillance cystoscopy for patients with augmentation and substitution cystoplasty for benign urological conditions: is it necessary? BJU International 2009; 104 (3): 392–395. DOI: 10.1111/j.1464-410X.2009.08401.x.
- Kokorowski PJ, Routh JC, Borer JG, Estrada CR, Bauer SB, Nelson CP. Screening for Malignancy After Augmentation Cystoplasty in Children With Spina Bifida: A Decision Analysis. The Journal of Urology 2011; 186 (4): 1437–1443. DOI: 10.1016/j.juro.2011.05.065.
最近更新时间: 2025-09-22 08:00