
37: 女性尿道上裂
阅读本章大约需要 6 分钟。
引言
膀胱外翻(BE)是一种严重的先天性泌尿道畸形,患儿出生时膀胱经腹壁外翻并暴露于体表,尿道背侧开放,并伴有生殖器的显著继发性畸形。它被广泛认为是泌尿道中外科治疗最具挑战性且最复杂的先天性疾病。1 BE 的严重程度不一,构成一个被称为膀胱外翻-尿道上裂复合体(BEEC)的连续谱。2 BEEC 的发病率为 ~每10,000人中1例。2
泄殖腔外翻(CE)属于膀胱外翻–尿道上裂复合体(BEEC)谱系中最为严重的一端。CE 是一种罕见的先天性疾病,在活产儿中的发病率为每 200,000–400,000 名活产儿中 1 例。3,4 常见相关畸形包括脐膨出、膀胱外翻、肛门闭锁和脊柱裂。4 其他特征包括:位于中线的盲肠外翻板,其两侧分别为膀胱的 2 个半部;有一段回肠自盲肠板脱垂;以及盲端的发育不全后肠,并伴有肛门闭锁。4
位于该疾病谱另一端的是尿道上裂。尿道上裂最常作为 BE 和 CE 的一个组成部分出现,但当其在缺乏 BE 和 CE 的情况下单独发生时,被认为是 BEEC 中最轻的变异。尿道上裂的定义为背侧尿道的融合不全。5 其表现范围从皮肤覆盖的阴茎上的轻度龟头部缺陷,到近端延伸至膀胱颈并在男性或女性中导致完全性尿失禁的阴茎耻骨型。5 有趣的是,据称尿道上裂的首例描述对象为拜占庭皇帝赫拉克略(公元 610–641 年)。6 孤立性男性尿道上裂是一种罕见的畸形,报告的发生率为每 117,000 名男性中 1 例。6 孤立性女性尿道上裂更为罕见,其发生率为每 484,000 名女性患者中 1 例。6 本章将专门讨论女性尿道上裂。
1928年,Davis 根据严重程度将女性尿道上裂分为三类。该分类系统至今仍在使用。7 在轻度尿道上裂中,尿道口仅表现为松弛、扩张。中度尿道上裂表现为尿道沿其大部分长度在背侧裂开。最重度尿道上裂中,尿道裂隙累及尿道全程,并使括约肌机制丧失功能。值得注意的是,女性尿道上裂的真实患病率可能高于报告,因为在较轻病例中外生殖器的改变可能很小,而若不存在尿失禁,患者常未被诊断。8,9
胚胎学
Marshall 和 Muecke 提出的关于外翻畸形胚胎发育异常的主要理论之一认为,其基本缺陷是在妊娠第4周的泄殖腔膜异常过度发育,这会阻止间充质组织向中线迁移并使下腹壁不能正常发育。这种有缺陷的泄殖腔膜发生破裂的时间被认为决定了由此产生的变异类型。10 一般认为,泄殖腔膜未能因中胚层的长入而得到加固。泄殖腔膜是位于胚盘尾端、占据脐下腹壁的双层结构。泄殖腔膜外胚层与内胚层之间的间充质长入,促成了下腹部肌肉和骨盆骨的形成。泄殖腔膜容易发生过早破裂;如果仅导致一个小的脐下缺损,或破裂发生在发育较晚阶段,则被认为会出现尿道上裂;而在缺损更大或破裂更早的情况下,则可出现 BE 或 CE。10,11
关于膀胱外翻-尿道上裂复合体病因的其他合理学说亦有提出。生殖丘位于正常位置的尾侧而发生异常发育,并在正中线融合
位于泄殖腔膜之下而非其上,已被其他研究者所采纳。11,12 另一种仍具争议的有趣假说描述了体柄的尾侧异常插入,导致中线的间充质组织间置失败。13 由于这一失败,泄殖腔不会转位至腹腔深部。停留在脐下浅表位置的泄殖腔膜代表一种不稳定的胚胎状态,具有很强的解体倾向,这一点已被 Thomalla et al 的实验室研究所支持。14,15 另一种有趣的理论则认为,骨盆的发育不良反而是膀胱外翻发生的诱发因素。Beaudoin et al 提出,骨盆环原基缺乏”旋转”会使附着于骨盆环的结构无法在中线合拢,从而允许膀胱发生疝出。16
流行病学
女性完全性尿道上裂是一种极为罕见的先天性缺陷,在活产中约为1/484,000,发生率远低于BE,后者估计为1/10,000至1/50,000。6 根据多项系列研究,膀胱外翻的男女性别比为2.3:1;女性尿道上裂也比男性尿道上裂更少见,后者在男性中的报告发病率为1/117,000。17
在某一家系中,BE复发的风险约为1/100。18 Shapiro 等人 通过问卷调查发现,在约2,500例已登记病例中,仅有9例出现BE和尿道上裂的复发。19 Shapiro 等人 确定,在患有BE和尿道上裂的个体的后代中,BE的风险为每70例活产中有1例,较一般人群的发生率高出500倍。17
发病机制
我们目前对尿道上裂的发病机制尚不完全清楚。由于缺乏高质量研究,专家们仍不确定导致尿道上裂的胚胎学起源和遗传机制。然而,近年来在鉴定BEEC中的候选基因方面已取得进展,这也涵盖了孤立性尿道上裂的发生。von Lowtow et al 评估了169例BEEC个体(受试者主要招募自欧洲,未报告地理-族裔遗传来源)。20 他们在多名受试者中发现了致病性拷贝数变异,其中包括一例22q11区域先前报道的重复。该区域也与22q11缺失综合征(DiGeorge综合征)以及CAKUT相关。21 随后的GWAS荟萃分析,整合了568名BEEC患者与3,241名欧洲血统对照,鉴定出与包含转录增强子ISL1的位点相关联(p = 2.22 × 10−08)。22,23,24,25,26 进一步的功能学与模型研究强化了ISL1在BEEC中的可能因果作用。例如,发育生物学模型被用来阐明ISL1在发育中的泌尿道内的活性定位。26 利用谱系示踪小鼠模型对ISL1表达细胞进行遗传谱系分析,显示在小鼠胚胎的泌尿道中存在ISL1表达细胞。26
评估与诊断
即便采用现代超声技术,BE 的产前诊断仍常常难以明确界定,而孤立性尿道上裂的产前诊断则几乎不可能。27 2012 年 Goyal et al. 发现,BEEC 病例中仅有 25% 在产前被诊断出。27 多个研究团队尝试勾勒出 BE 产前诊断的重要标准,但对于尿道上裂并无特异性征象。他们发现,对于经典型 BE,反复检查均未见正常充盈的膀胱提示该诊断,而下腹壁可见一团超声高回声组织亦同样提示诊断。28,29 脐带附着点至生殖结节的距离低于相应孕周的第 5 百分位,也提供了一项可据以评估 BE 诊断的定量指标。30 在对 25 例产前超声检查且随后出生为 BE 新生儿的回顾中,Gearhart et al 作出以下观察:1 无膀胱充盈,2 低位脐,3 耻骨支增宽,4 生殖器体积小,以及5 随着妊娠进展及腹腔内脏器体积增加而逐渐增大的下腹部肿块。31 不难理解,为何孤立性尿道上裂的产前诊断更为困难。在上述产前观察中,只有低位脐、耻骨支增宽和生殖器体积小可能在孤立性尿道上裂的情境下出现。上述所有发现于孤立性尿道上裂中的程度都会更轻,而在孤立性女性尿道上裂的情境下,“生殖器体积小”并不适用。
因此,孤立性女性尿道上裂的诊断一般在出生后通过体格检查作出。外生殖器外观的改变可能很轻微,尤其是在轻型尿道上裂病例中。外观上可见以分裂阴蒂为特征的生殖器缺陷。耻丘呈凹陷形态,表面覆以光滑、无毛的皮肤区。在该区域之下,可能有中等量的皮下组织与脂肪,或该处皮肤可能直接位于耻骨联合表面的前下方。小阴唇通常发育不良,前方终止于分裂阴蒂相应的一侧半部处,局部可见包皮皱襞的残迹。耻骨联合通常闭合,但也可能分离,仅由一条狭窄的纤维带连接。分开阴唇后可见尿道异常,其表现随尿道上裂的程度而差异很大。尿道异常可从远端短小缺损到近端延伸至膀胱颈的缺损(图 1)。阴道和内生殖器通常正常。由于外观改变可能很轻微,有些患儿仅因持续性尿失禁而被发现;而在无尿失禁的轻型病例中,可能从未得到诊断。这也解释了女性尿道上裂的真实患病率可能高于文献报道。8,9 因此,孤立性女性尿道上裂必然累及尿道异常,但膀胱颈可合并存在异常,在处理这些患者时不可忽视。在较重型女性尿道上裂中,膀胱可能较小,可与已行关闭术的膀胱外翻患者的膀胱相当,因为胎内不存在膀胱的充盈—排空循环。事实上,所有伴尿失禁的尿道上裂患者中,有三分之一的膀胱容量小于60 mL,膀胱输尿管返流的发生率为30%~75%。32
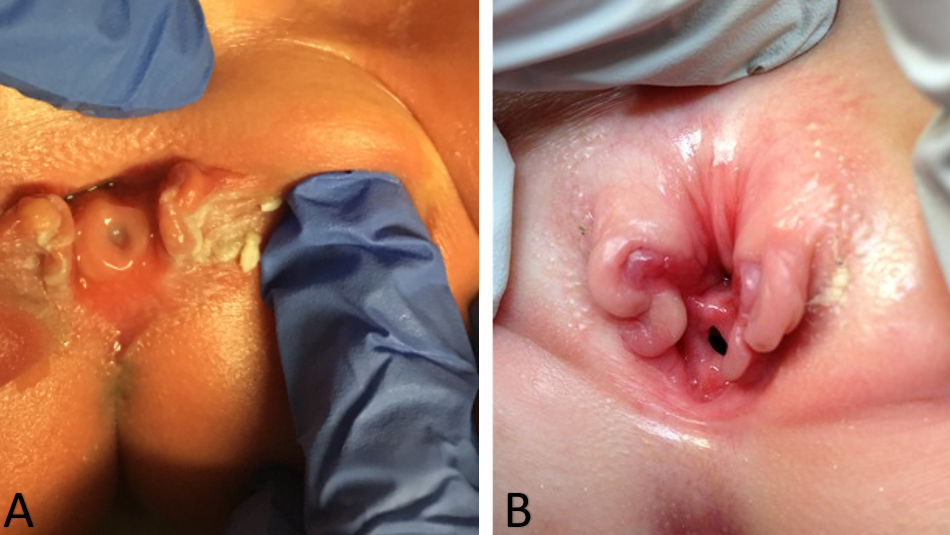
图 1 女性尿道上裂的重度病例。新生儿的阴茎耻骨型尿道上裂(A)。4岁儿童的阴茎耻骨型尿道上裂(B)。
治疗与预后
对于女性尿道上裂患者,治疗目标是实现尿控、保护上尿路,并重建功能正常且外观可接受的外生殖器。对于尿道上裂程度较轻、能够保持干燥(无尿失禁)且外生殖器仅有轻微改变的患者,可能无需手术重建。对于更严重形式的女性尿道上裂,则需要进行手术重建以获得尿控并矫正外生殖器的异常。
从历史上看,曾有许多手术被报道用于试图在尿道上裂患者群体中实现控尿,但结果令人失望。这些手术包括经阴道对尿道和膀胱颈行褶皱缝合术、肌肉移植术、尿道扭转术、尿道烧灼术、膀胱瓣术,以及 Marshall-Marchetti 膀胱尿道悬吊术。33,34,35,36 这些手术旨在增加尿道阻力,但由于未尝试使尿道和膀胱颈的解剖结构正常化,未能纠正尿失禁。
如前所述,无尿失禁的远端尿道上裂患者可能不需要任何外科干预。对于近端女性尿道上裂的情况,我们通常同时进行尿道上裂修补和膀胱颈重建,并可同期选择行或不行截骨术(图 2)。这与我们在膀胱外翻(BE)病例中实施的完全一期修复相似,通常在生后 3–6 个月进行。我们发现,尿道上裂修补和膀胱颈重建所增加的阻力有利于实现膀胱的周期性充盈-排空,并且常可导致膀胱容量增加。其他作者也证实了这些发现:在膀胱外翻已闭合的儿童中,行上裂尿道的一期闭合可在不引起肾积水的情况下增加膀胱容量。这一策略已应用于男女尿道上裂患者。37,38,39

图 2 严重女性尿道上裂患者在行尿道上裂修复术及膀胱颈重建术后的图像。
在孤立性尿道上裂的女性中,控尿率被发现介于67-87.5%之间。6,32,40 据报道,从重建术后到获得控尿的平均间隔为18至30个月。6,41 也有罕见的报告称,患者在重建术后数年才达到完全控尿。32 人们推测,这种获得控尿的延迟较长是继发于骨盆肌肉随时间逐渐增强的发育,尤其是在青春期激素变化之后。32
并发症
尿道上裂的外科治疗众所周知极具挑战性,因此并发症并不少见。修复尿道上裂后可能出现的并发症包括尿道皮肤瘘、尿道外口狭窄以及尿道狭窄。对于需要行膀胱颈手术的患者,术后密切随访的重要性再怎么强调也不为过。当膀胱出口阻力被提高时,患者有发生高压膀胱的风险,因为膀胱为对抗高阻力而收缩,从而使其上尿路面临风险。因此,外科医生在重建术后必须非常密切地随访患者,以便及早发现新发肾积水或其他高压系统的征象。对于术前存在容量小、顺应性差的膀胱的患者,这一点尤为重要,尽管在尿道上裂中这种情况非常罕见。此外,膀胱颈手术后,患者仍可能出现尿失禁,可能需要进一步手术以实现控尿。
对于严重近端型尿道上裂的患者,为通过减少耻骨分离来减轻闭合部位的张力,可能需要在泌尿重建时行双侧髂骨截骨术。与双侧髂骨截骨术相关的风险包括失血、下肢灌注减少,而在极为严重的情况下还可能出现阴蒂灌注减少。若截骨术后将耻骨靠拢过于紧密,阴蒂灌注减少可能发生。对于需要进行膀胱颈重建的患者,也可能出现膀胱皮肤瘘。有趣的是,当 Suson et al 将22名完全性尿道上裂的女童与23名经典型 BE 的女童进行比较时,他们未发现手术次数、获得控尿能力(无论是否需要膀胱颈重建),或最终是否需要控尿性尿路改道方面存在差异。5
建议的随访
对于远端型尿道上裂且能够正常排尿、上尿路健康的患者,通常仅需监测,并在随访一段时间后有可能结束专科管理。或者,病情更为严重并接受重建手术的尿道上裂患者,应在整个儿童期并持续至成人期接受随访。至关重要的是,进入成人期后,应将其医疗管理转交给具有治疗复杂先天性泌尿系统畸形经验的过渡期泌尿科医生。
如前所述,接受尿道上裂修复术和膀胱颈重建的患者术后需要非常密切的随访。研究表明,未同时行膀胱扩大术而仅行膀胱颈手术的患者,存在出现膀胱压力升高并继发上尿路恶化的风险。即便进行了详尽的术前检查与评估,以确保术前膀胱压力和顺应性处于安全范围,仍然可能发生上述情况。尽管进行了术前筛选,膀胱动力学仍会发生显著改变,且有40%的神经源性膀胱患者随后需要进行膀胱扩大术。42 因此,每年进行肾脏与膀胱超声检查的随访对这些患者至关重要。
结论
孤立性女性尿道上裂是一种极为罕见的疾病,被认为是BEEC中严重程度最低的变异。其表现可从不影响控尿功能的轻度远端缺损,到向近端延伸至膀胱颈并导致完全性尿失禁的完全型不等。5 与BE类似,近端型尿道上裂被广泛认为是泌尿道先天畸形中手术挑战性和复杂性最高的疾病之一。1 在最严重的类型中,可能需要行尿道上裂修复术、膀胱颈重建术,甚至截骨术。许多尿道上裂患者需要由具有诊治复杂泌尿系统畸形经验的泌尿外科医师进行终身随访。
要点
- 尿道上裂是BEEC中最轻的亚型,其定义为尿道背侧融合不完全。
- 完全型女性尿道上裂是一种极其罕见的先天性缺陷,发生于约1/484,000的活产中,远低于BE,其估计发生率为1/10,000至1/50,000。
- 孤立性女性尿道上裂的诊断通常在出生后通过体格检查作出,因为经产前影像学的诊断并不可靠。
- 尿道异常的范围可从远端的短缺损到近端延伸至膀胱颈。
- 对于女性尿道上裂患者,治疗目标是实现控尿、保护上尿路,并重建功能性且美观可接受的外生殖器。
- 对于轻度尿道上裂、能保持干燥且外生殖器仅有轻微改变的患者,可能无需外科重建。
- 对于较为严重的女性尿道上裂,需进行外科重建以获得控尿并矫正外生殖器的异常。
- 孤立性女性尿道上裂患者的控尿率报道为67-87.5%。
参考文献
- Weiss DA, Shukla AR, Borer JG, Sack BS, Kryger JV, Roth EB, et al.. Evaluation of outcomes following complete primary repair of bladder exstrophy at three individual sites prior to the establishment of a multi-institutional collaborative model. J Pediatr Urol 2020; 16 (4): 435.e1–435.e6. DOI: 10.1016/j.jpurol.2020.05.153.
- Reutter H, Keppler-Noreuil K, E. Keegan C, Thiele H, Yamada G, Ludwig M. Genetics of Bladder-Exstrophy-Epispadias Complex (BEEC): Systematic Elucidation of Mendelian and Multifactorial Phenotypes. Curr Genomics 2005; 17 (1): 4–13. DOI: 10.2174/1389202916666151014221806.
- Phillips TM. Spectrum of cloacal exstrophy. Semin Pediatr Surg 2011; 20 (2): 113–118. DOI: 10.1053/j.sempedsurg.2010.12.007.
- Woo LL, Thomas JC, Brock JW. Cloacal exstrophy: A comprehensive review of an uncommon problem. J Pediatr Urol 2010; 6 (2): 102–111. DOI: 10.1016/j.jpurol.2009.09.011.
- Suson KD, Preece J, Baradaran N, Di Carlo HN, Gearhart JP. The Fate of the Complete Female Epispadias and Exstrophy Bladder–Is There a Difference? J Urol 2013; 190 (4s): 1583–1589. DOI: 10.1016/j.juro.2013.01.093.
- Gearhart JP. Exstrophy-Epispadias Complex in Campbell-Walsh-Wein Urology 2021. Elsevier; .
- Davis DM. Epispadias in Females and Its Surgical Treatment. J Urol 1928; 20 (6): 673–678. DOI: 10.1016/s0022-5347(17)73196-5.
- Yeni E, Unal D, Verit A, Karatas OF. An adult female epispadias without exstrophy was presented with urinary incontinence: a case report. Int Urogynecol J 2004; 15 (3): 212–213. DOI: 10.1007/s00192-004-1131-2.
- Krishna Shetty MV, Sen TK, Bhaskaran VA. Female epispadias. Afr J Paediatr Surg 2011; 8 (2): 215. DOI: 10.4103/0189-6725.86066.
- Muecke EC. The Role of the Cloacae Membrane in Exstrophy: The First Successful Experimental Study. J Urol 1964; 92 (6): 659–668. DOI: 10.1016/s0022-5347(17)64028-x.
- Ambrose SS, O’Brien DP. Surgical Embryology of the Exstrophy-Epispadias Complex. Surg Clin North Am 1974; 54 (6): 1379–1390. DOI: 10.1016/s0039-6109(16)40493-7.
- Patten BM, Barry A. The genesis of exstrophy of the bladder and epispadias. Am J Anat 1952; 90 (1): 35–57. DOI: 10.1002/aja.1000900103.
- Mildenberger H, Kluth D, Dziuba M. Embryology of bladder exstrophy. J Pediatr Surg 1988; 23 (2): 166–170. DOI: 10.1016/s0022-3468(88)80150-7.
- Johnston JH, Kogan SJ. The exstrophic anomalies and their surgical reconstruction. Curr Probl Surg 1974; 11 (8): 1–39. DOI: 10.1016/s0011-3840(74)80011-0.
- Thomalla JV, Rudolph RA, Rink RC, Mitchell ME. Induction of Cloacal Exstrophy in the Chick Embryo Using the CO 2 Laser. J Urol 1985; 134 (5): 991–995. DOI: 10.1016/s0022-5347(17)47573-2.
- Beaudoin S, Simon L, Bargy F. Anatomical basis of a common embryological origin for epispadias and bladder or cloacal exstrophies. Surg Radiol Anat 1997; 19 (1): 11–16. DOI: 10.1007/bf01627728.
- Shapiro E, Lepor H, Jeffs RD. The Inheritance of the Exstrophy-Epispadias Complex. J Urol 1984; 132 (2): 308–310. DOI: 10.1016/s0022-5347(17)49605-4.
- Ives E, Coffey R, Carter CO. A family study of bladder exstrophy. J Med Genet 1980; 17 (2): 139–141. DOI: 10.1136/jmg.17.2.139.
- Shapiro E, Jeffs RD, Gearhart JP, Lepor H. Muscarinic Cholinergic Receptors in Bladder Exstrophy: Insights Into Surgical Management. J Urol 1985; 134 (2): 308–310. DOI: 10.1016/s0022-5347(17)47139-4.
- Reutter H, Boyadjiev SA, Gambhir L, Ebert A-K, Rösch WH, Stein R, et al.. Phenotype Severity in the Bladder Exstrophy-Epispadias Complex: Analysis of Genetic and Nongenetic Contributing Factors in 441 Families from North America and Europe. J Pediatr 2011; 159 (5): 825–831.e1. DOI: 10.1016/j.jpeds.2011.04.042.
- WOOD HADLEYM, TROCK BRUCEJ, GEARHART JOHNP. In Vitro Fertilization and the Cloacal-Bladder Exstrophy-Epispadias Complex: Is there an Association? J Urol 2003; 169 (4): 1512–1515. DOI: 10.1097/01.ju.0000054984.76384.66.
- Lowtzow C von, Hofmann A, Zhang R, Marsch F, Ebert A-K, Rösch W, et al.. CNV analysis in 169 patients with bladder exstrophy-epispadias complex. BMC Med Genet 2016; 17 (1): 35. DOI: 10.1186/s12881-016-0299-x.
- Sanna-Cherchi S, Kiryluk K, Burgess KE, Bodria M, Sampson MG, Hadley D, et al.. Copy-Number Disorders Are a Common Cause of Congenital Kidney Malformations. Am J Hum Genet 2012; 91 (6): 987–997. DOI: 10.1016/j.ajhg.2012.10.007.
- Arkani S, Cao J, Lundin J, Nilsson D, Källman T, Barker G, et al.. Evaluation of the ISL1 gene in the pathogenesis of bladder exstrophy in a Swedish cohort. Hum Genome Var 2018; 5 (1): 18009. DOI: 10.1038/hgv.2018.9.
- Draaken M, Knapp M, Pennimpede T, Schmidt JM, Ebert A-K, Rösch W, et al.. Genome-wide Association Study and Meta-Analysis Identify ISL1 as Genome-wide Significant Susceptibility Gene for Bladder Exstrophy. PLoS Genet 2015; 11 (3): e1005024. DOI: 10.1371/journal.pgen.1005024.
- Reutter H, Draaken M, Pennimpede T, Wittler L, Brockschmidt FF, Ebert A-K, et al.. Genome-wide association study and mouse expression data identify a highly conserved 32 kb intergenic region between WNT3 and WNT9b as possible susceptibility locus for isolated classic exstrophy of the bladder. Hum Mol Genet 2014; 23 (20): 5536–5544. DOI: 10.1093/hmg/ddu259.
- Reutter H, Hoischen A, Ludwig M, Stein R, Radlwimmer B, Engels H, et al.. Genome-wide analysis for micro-aberrations in familial exstrophy of the bladder using array-based comparative genomic hybridization. BJU Int 2007; 100 (3): 646–650. DOI: 10.1111/j.1464-410x.2007.07086.x.
- Zhang R, Knapp M, Suzuki K, Kajioka D, Schmidt JM, Winkler J, et al.. ISL1 is a major susceptibility gene for classic bladder exstrophy and a regulator of urinary tract development. Sci Rep 2017; 7 (1): 42170. DOI: 10.1038/srep42170.
- Goyal A, Fishwick J, Hurrell R, Cervellione RM, Dickson AP. Antenatal diagnosis of bladder/cloacal exstrophy: Challenges and possible solutions. J Pediatr Urol 2012; 8 (2): 140–144. DOI: 10.1016/j.jpurol.2011.05.003.
- Mirk P, Calisti A, Fileni A. Prenatal sonographic diagnosis of bladder extrophy. J Ultrasound Med 1986; 5 (5): 291–293. DOI: 10.7863/jum.1986.5.5.291.
- VERCO PW, KHOR BH, BARBARY J, ENTHOVEN C. Ectopia Vesicae in Utero. Australas Radiol 1986; 30 (2): 117–120. DOI: 10.1111/j.1440-1673.1986.tb02400.x.
- Fishel-Bartal M, Perlman S, Messing B, Bardin R, Kivilevitch Z, Achiron R, et al.. Early Diagnosis of Bladder Exstrophy: Quantitative Assessment of a Low-Inserted Umbilical Cord. J Ultrasound Med 2017; 36 (9): 1801–1805. DOI: 10.1002/jum.14212.
- GEARHART J, BENCHAIM J, JEFFS R, SANDERS R. Criteria for the prenatal diagnosis of classic bladder exstrophy. Obstet Gynecol 1995; 85 (6): 961–964. DOI: 10.1016/0029-7844(95)00069-4.
- Kelalis PP, Kramer SA. Surgical Correction of Female Epispadias. Eur Urol 1982; 8 (6): 321–324. DOI: 10.1159/000473547.
- Jonuzi A, Popović N, Zvizdić Z, Milišić E, Karavdić K, Dewan P. Female Epispadias Presenting as Urinary Incontinence. APSP J Case Rep 2017; 8 (2): 10. DOI: 10.21699/ajcr.v8i2.548.
- Gross RE, Cresson SL. Exstrophy Of Bladder. J Am Med Assoc 1952; 149 (18): 1640. DOI: 10.1001/jama.1952.02930350028008.
- MARSHALL VICTORFRAY, MARCHETTI ANDREWA, KRANTZ KERMITE. The Correction of Stress Incontinence by Simple Vesicourethral Suspension. J Urol 1949; 88 (4): 1326–1331. DOI: 10.1097/00005392-200210010-00005.
- &Na;. Epispadias and Incontinence. Plast Reconstr Surg 1983; 37 (5): 468. DOI: 10.1097/00006534-196605000-00023.
- Ben-Chaim J, Peppas DS, Jeffs RD, Gearhart JP. Complete Male Epispadias: Genital Reconstruction and Achieving Continence. J Urol 1995; 153 (5): 1665–1667. DOI: 10.1016/s0022-5347(01)67499-8.
- Gearhart JP, Jeffs RD. Bladder Exstrophy: Increase in Capacity Following Epispadias Repair. J Urol 1989; 142 (2 Part 2): 525–526. DOI: 10.1016/s0022-5347(17)38804-3.
- Peters CA, Gearhart JP, Jeffs RD. Epispadias and Incontinence: The Challenge of the Small Bladder. J Urol 1988; 140 (5 Part 2): 1199–1201. DOI: 10.1016/s0022-5347(17)42001-5.
- Hanna MK, Williams DI. Genital Function In Males With Vesical Exstrophy And Epispadias. Br J Urol 1972; 44 (2): 169–174. DOI: 10.1111/j.1464-410x.1972.tb10062.x.
- Klauber GT, Williams DI. Epispadias with incontinence. Plast Reconstr Surg 1974; 54 (4): 504. DOI: 10.1097/00006534-197410000-00053.
- Weiss D. Faculty Opinions recommendation of Clinical outcomes after increasing bladder outlet resistance without augmentation cystoplasty in neurogenic bladder. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2021; 17 (2): 235 1–235 7. DOI: 10.3410/f.739262243.793583985.
最近更新时间: 2025-09-22 08:00