
39: Seio urogenital
Este capítulo levará aproximadamente 13 minutos para ler.
Introdução
O seio urogenital isolado é uma anomalia congênita rara do sistema urogenital feminino em que a uretra e a vagina não se separam durante o desenvolvimento, formando um canal comum. As anomalias do seio urogenital são encontradas em quatro cenários clínicos distintos:1
- Condições de ambiguidade genital (como hiperplasia adrenal congênita)
- Cloaca persistente com envolvimento retal
- Extrofia feminina
- Seio urogenital isolado
Este capítulo se concentrará no seio urogenital isolado.
Epidemiologia
A incidência de seio urogenital isolado não é bem conhecida, embora fontes relatem uma taxa de incidência que varia de 6/100,000 a 1/250,000 nascimentos do sexo feminino.2,3
Embriologia/Etiologia
O seio urogenital comum (UGS) é uma estrutura transitória normal no desenvolvimento embrionário que posteriormente se separa e dá origem à uretra e ao terço distal da vagina. A etiologia do seio urogenital isolado não é bem compreendida, mas é geralmente aceita como resultado de uma interrupção do desenvolvimento da formação urogenital feminina no primeiro trimestre, em que a uretra e a vagina não formam aberturas perineais separadas.4 Postula-se que uma interrupção precoce da diferenciação vaginal formará um canal comum longo (confluência alta), ao passo que uma interrupção mais tardia da diferenciação formará um canal comum curto (confluência baixa) (Figura 1).5
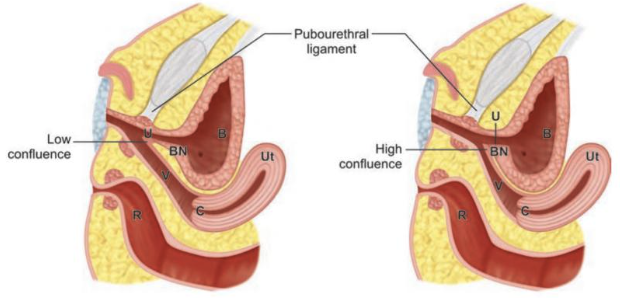
Figura 1 Diagrama mostrando confluência baixa (esquerda) e confluência alta (direita). Observe a localização da confluência da uretra (U) e da vagina (V) em relação ao colo vesical (BN) e ao ligamento pubouretral. Outras estruturas representadas incluem o útero (Ut), a bexiga (B), o reto (R) e o colo do útero (C). Carrasco “Surgical Techniques in Pediatric and Adolescent Urology”.6
Avaliação Clínica
Apresentação Clínica
Muitos casos são identificados por meio de ultrassonografia pré-natal mostrando estruturas pélvicas preenchidas por líquido que frequentemente representam hidrocolpos ou hidrometrocolpos (Figura 2).1,6
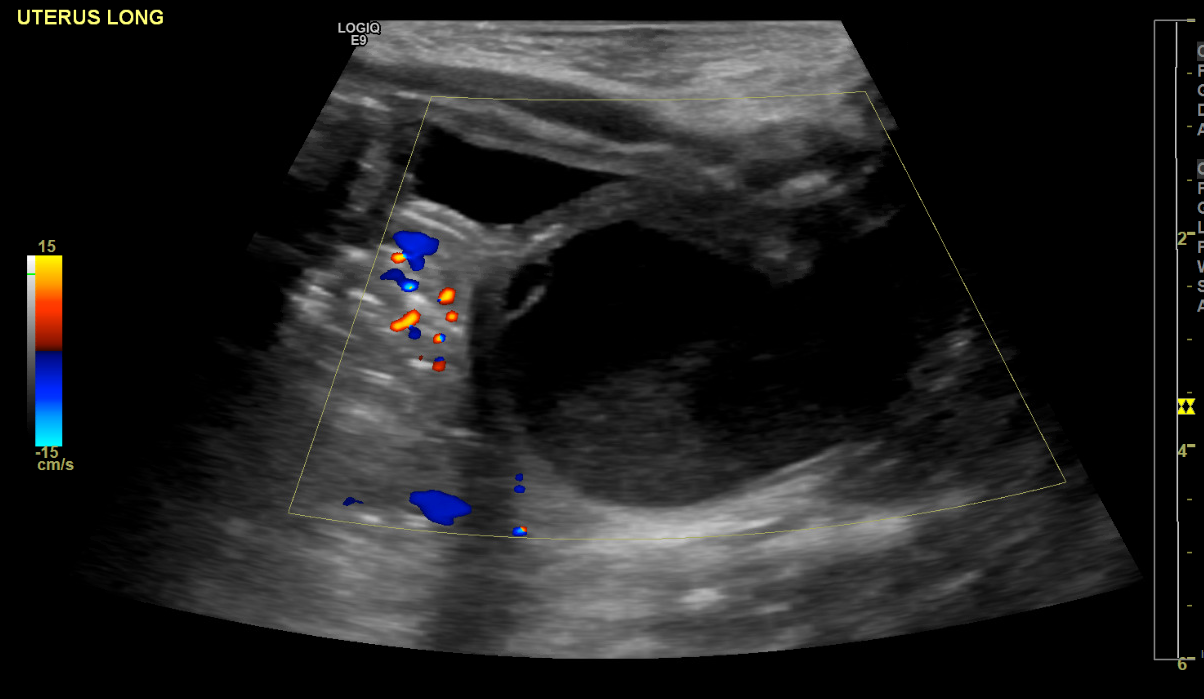
Figura 2 Ultrassonografia mostrando a bexiga anteriormente e hidrocolpos posteriormente.
Sinais e sintomas de apresentação: pacientes que não são identificados na ultrassonografia pré-natal podem posteriormente apresentar o seguinte:
- Infecção do trato urinário
- Incontinência urinária
- Gotejamento pós-miccional
- Acúmulo de líquido vaginal
- Hematúria menstrual7
- Ou pode ser assintomático
Exame Físico
O exame físico deve incluir:
- Exame abdominal
- Pode revelar uma massa suprapúbica palpável representando uma bexiga distendida e/ou hidrometrocolpo1
- Exame da coluna
- O exame da coluna lombar deve ser realizado, pois anomalias do seio urogenital podem estar associadas a anomalias da medula espinal1
- Exame genital
- Mostrará um único orifício perineal (Figura 3)
- Para examinar lactentes, o uso de aplicadores com ponta de algodão pode auxiliar na separação dos lábios para visualizar adequadamente o orifício perineal.

Figura 3 Abertura perineal única no exame genital. Imagem adaptada de Grey’s Anatomy, prancha 1119 (imagem em domínio público).
Exames Diagnósticos
Exames de imagem
O papel dos exames de imagem na avaliação do seio urogenital isolado é limitado. A ultrassonografia do sistema urinário e do sistema reprodutor deve ser realizada para excluir quaisquer outras anomalias e para definir a localização desses órgãos.1
Um genitograma pode ser obtido para delinear melhor a anatomia, mas pode ter utilidade limitada no seio urogenital isolado.
Exames de imagem da coluna vertebral podem ser necessários para avaliar anomalias da medula espinhal.
Endoscopia
A avaliação diagnóstica mais importante no seio urogenital isolado é feita por cistoscopia e vaginoscopia. Isso permite ao cirurgião avaliar o comprimento do canal comum e a localização da confluência uretral e vaginal em relação ao colo vesical, o que é crucial para determinar a abordagem cirúrgica adequada.6 Essa avaliação endoscópica é realizada no momento do reparo cirúrgico e será discutida mais adiante em uma seção posterior deste capítulo.
Tratamento cirúrgico
Manejo imediato
Se um paciente necessitar drenagem de hidrocolpos, pode-se, sob anestesia, optar por um cateter por via do canal comum (intermitente ou de demora), um cateter suprapúbico ou uma vaginostomia. Caso contrário, a urina provavelmente continuará a se acumular na vagina e/ou no útero. A cateterização pode ser necessária até a realização de cirurgia reconstrutiva posterior.
Tratamento definitivo
Indicações cirúrgicas
A correção cirúrgica está indicada se os pacientes estiverem sintomáticos devido ao seio urogenital, especialmente se houver problemas de acúmulo de urina, como hidronefrose ou hidrocolpos.6 Se os pacientes forem assintomáticos, a correção cirúrgica pode ser adiada.
Aconselhamento pré-operatório
Objetivos Cirúrgicos
Os objetivos da correção cirúrgica devem ser discutidos com os pais antes de prosseguir e devem incluir o seguinte:
- genitália com aparência normal
- orifícios uretral e vaginal separados
- drenagem de urina
- abertura vaginal de tamanho adequado para produtos menstruais e futuras relações sexuais
Momento cirúrgico
Recomendamos que a correção cirúrgica seja realizada entre 6 e 12 meses de idade.6 O momento ideal para o seio urogenital isolado não foi estabelecido na literatura e é extrapolado a partir de pacientes com hiperplasia adrenal congênita e seio urogenital associado.
Aqueles que defendem a correção cirúrgica precoce sustentam que os tecidos podem ser mais maleáveis em idade precoce e que o estrogênio materno residual circulante pode favorecer a cicatrização de feridas.1 Os que defendem a correção cirúrgica na idade puberal alegam os mesmos benefícios hormonais, além da participação do paciente e de seu assentimento em prosseguir.1
Técnicas Cirúrgicas
Preparação pré-operatória
- A preparação intestinal não é necessária
- Devem ser administrados antibióticos pré-operatórios para cobrir a flora cutânea e vaginal
- A correção cirúrgica envolve 2 partes distintas:
- Avaliação endoscópica para determinar o comprimento do canal e sua relação com o colo vesical
- Correção definitiva por vaginoplastia
- A abordagem da vaginoplastia é determinada pela avaliação endoscópica
Exame sob anestesia e cistoscopia e vaginoscopia
O paciente deve ser posicionado em posição de litotomia dorsal. O exame sob anestesia (EUA) deve incluir a avaliação do intróito e da abertura perineal única.
Em seguida, a avaliação endoscópica deve ser concluída. Durante isso, o cirurgião deve medir o comprimento de certos parâmetros anatômicos, como o comprimento da uretra, da vagina e do canal comum em relação ao colo vesical. O comprimento do canal e sua relação com o colo vesical são os parâmetros mais cruciais para determinar a abordagem cirúrgica do reparo definitivo.
- Comprimento do canal de < 3 cm → Vaginoplastia com retalho ou PUM/TUM
- Comprimento do canal de > 3 cm → Vaginoplastia por Pull-Through ou Abordagem sagital anterior transretal (ASTRA)
A avaliação endoscópica deve começar com cistoscopia utilizando um cistoscópio rígido de calibre adequado. O cistoscópio deve ser avançado através do canal comum, na uretra, que será o orifício anterior, e então na bexiga. A bexiga deve ser inspecionada minuciosamente para garantir que não haja outras anomalias anatômicas.
Em seguida, realiza-se vaginoscopia com o cistoscópio. O tamanho geral, a elasticidade e a forma (ou seja, anomalias de duplicação) devem ser avaliados.6
Após a conclusão do EUA e da avaliação endoscópica, o cirurgião deve então determinar qual abordagem de vaginoplastia é mais adequada para o paciente.
Mobilização Urogenital Total e Parcial
Descrito pela primeira vez por: Alberto Pena em 19979
Indicações: Comprimento uretral adequado, dissecção extensa ao nível do colo vesical não prevista
Posição: variável, dependendo do método de vaginoplastia
Descrição breve: Todo o seio é dissecado circunferencialmente e mobilizado em direção ao períneo.1
Isto é categorizado como mobilização urogenital parcial (PUM) ou mobilização urogenital total (TUM), dependendo da transecção do ligamento pubouretral (Figura 4).6 Este procedimento também permite a mobilização de todo o seio urogenital para proporcionar um vestíbulo revestido por mucosa. Ele possibilita que uma confluência em nível médio atinja o períneo sem exigir separação vaginal.
Etapas
- A UGS é marcada circunferencialmente na sua junção com os lábios menores e ao longo da linha média do períneo em direção à borda anterior do ânus
- A dissecção começa na parede posterior da UGS, estendendo-se lateralmente e depois anteriormente até que a UGS esteja mobilizada circunferencialmente
- A dissecção das paredes lateral e anterior deve permanecer medial ao músculo bulboesponjoso para evitar sangramento
- A mobilização deve ser continuada até que a uretra e a vagina possam alcançar o intróito com mínima ou nenhuma tensão6
- A mobilização urogenital parcial para ao nível do ligamento pubouretral para reduzir o possível risco de incontinência de esforço ou encurtamento da vagina (Figura 4)
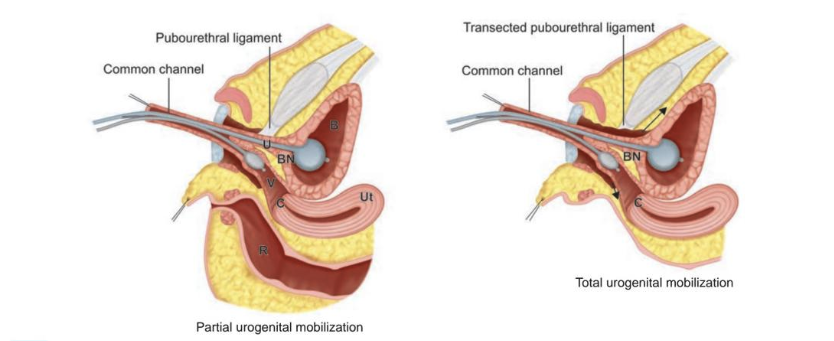
Figura 4 Mobilização urogenital parcial (à esquerda) e total (à direita) com cateteres na bexiga (B) e na vagina (V) para auxiliar na tração. Observe que, na mobilização urogenital total, o ligamento pubouretral é seccionado e a dissecção é levada proximalmente (setas) até que a uretra e a vagina possam alcançar o períneo. Outras estruturas representadas incluem o útero (Ut), o colo vesical (BN) e o reto (R). Fonte: Carrasco “Surgical Techniques in Pediatric and Adolescent Urology”.6
Vaginoplastia com retalho
Descrito pela primeira vez por: Fortunoff et al em 196410
Indicações: confluência baixa, canal comum curto
Posição: litotomia
Descrição breve: O intróito e o seio urogenital são amplamente abertos; o nível de confluência não se altera
Durante este procedimento, as paredes posteriores do seio e da vagina são abertas, a parede anterior da vagina é mantida intacta, e o retalho perineal posterior se encaixa na vagina aberta; portanto, a pele está cobrindo o aspecto posterior do intróito e da parede vaginal.
Etapas
- Uma incisão em U invertido ou em forma de ômega sobre o períneo na borda posterior do UGS é feita.11
- O retalho deve ser suficientemente longo para possibilitar uma anastomose sem tensão com a vagina e suficientemente amplo para proporcionar um introito de calibre normal, sem comprometer a irrigação sanguínea do corpo perineal.1
- O UGS é dissecado paralelamente à parede posterior do UGS em direção à parede vaginal posterior, afastando-se do reto
- A dissecção lateral deve ser minimizada para evitar sangramento
- A dissecção posterior deve continuar até que a confluência possa alcançar facilmente o introito
- Após concluir a dissecção posterior, a parede posterior do UGS é dividida na linha média, assim como a parede vaginal posterior, até que se obtenha uma abertura vaginal de tamanho adequado
- O ponto médio do retalho cutâneo perineal é então suturado à parede vaginal posterior dividida (Figura 5)
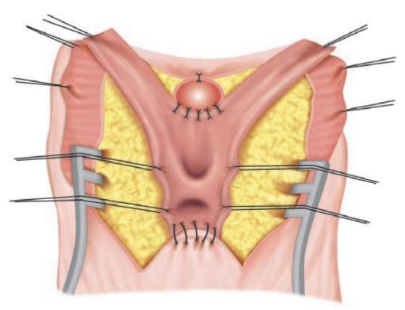
Figura 5 Diagrama representando a vaginoplastia com retalho. O canal comum foi incisado na linha média, expondo a uretra e a vagina. Observe a ancoragem do ápice anterior do UGS e a ancoragem do ápice posterior ao retalho cutâneo em U. A parede redundante do canal comum pode ser excisada ou utilizada para reconstrução adicional da comissura posterior. Fonte: Carrasco “Técnicas Cirúrgicas em Urologia Pediátrica e do Adolescente”.6
Vaginoplastia por Tração
Primeiramente descrita por: Hendren e Crawford em 196913
Indicações: confluência alta com comprimento uretral curto, ou quando se prevê mobilização extensa do colo vesical6
Posição: prona
Descrição breve: A vagina é separada do seio urogenital e trazida separadamente ao períneo, enquanto o UGS é utilizado para criar uma uretra. Isso é ideal quando há comprimento vaginal longo com excelente elasticidade.6
Etapas
- Cria-se um retalho cutâneo perineal posterior semelhante ao da vaginoplastia com retalho
- As paredes posteriores e laterais do UGS são dissecadas, estendendo-se às paredes posteriores e laterais da vagina
- O corpo perineal pode ser dividido para exposição adicional, se necessário
- A parede vaginal posterior é então incisada na sua junção com o UGS para expor a confluência da uretra e da vagina
- A parede uretral posterior é separada da parede vaginal anterior (Figura 6, A)
- Frequentemente não há um plano verdadeiro entre essas estruturas
- A dissecção deve tender para o lado vaginal para minimizar o risco de lesão da uretra (incluindo o esfíncter1), do colo vesical e dos ureteres
- A dissecção é levada o mais proximalmente possível até que o óstio vaginal possa ser trazido ao períneo com tensão mínima
- O defeito do canal comum é fechado e agora o canal comum passa a ser a uretra (Figura 6, B)
- O retalho perineal posterior é suturado à vagina de maneira semelhante à vaginoplastia com retalho
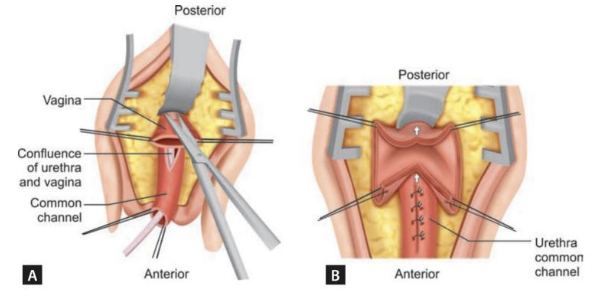
Figura 6 Diagrama ilustrando vaginoplastia por abaixamento (pull-through). A: A parede vaginal posterior foi incisada no nível da confluência da uretra com a vagina. B: As paredes vaginais anterior e posterior são dissecadas proximalmente (setas) para permitir a mobilização da vagina em direção ao períneo. Observe que a junção da vagina com o canal comum é fechada, tornando o canal comum uma continuação da uretra. Fonte: Carrasco “Surgical Techniques in Pediatric and Adolescent Urology”.6
Abordagem sagital anterior transretal
Descrito pela primeira vez por: Domini et al em 199714
Indicações: confluência alta
Posição: prona
Descrição breve: A confluência alta é acessada posteriormente através da parede anterior do reto para separar a vagina do seio urogenital
Etapas
- Realiza-se uma incisão perineal na linha média desde a borda anal anterior até a abertura do UGS.15
- Realiza-se incisão da parede retal anterior e do esfíncter anorretal, expondo a parede vaginal posterior
- Realiza-se incisão da parede vaginal posterior o mais próximo possível da junção com a uretra
- A vagina é mobilizada póstero-lateralmente e, em seguida, dissecada da uretra
- A abertura uretral é fechada
- A vagina é trazida ao períneo, utilizando-se retalhos de pele perineais, se necessário
- A parede anorretal é fechada em 2 planos
- O esfíncter anorretal e o corpo perineal são reconstruídos
Abordagens laparoscópicas e assistidas por robô
Há alguns relatos de abordagens laparoscópicas e robóticas para a reconstrução do seio urogenital.16,17 A abordagem laparoscópica ou robótica permite a dissecção do útero e da vagina, afastando-os da bexiga e do reto a partir do interior do abdome. A vagina é então trazida ao períneo.
Cuidados pós-operatórios
- Os cuidados pós-operatórios são variáveis, dependendo da extensão do reparo cirúrgico e da idade do paciente.6
- Um paciente jovem submetido a um reparo mais limitado (p. ex., vaginoplastia com retalho) poderia receber alta para casa no mesmo dia.
- Um paciente mais velho submetido a um reparo mais extenso (p. ex., vaginoplastia pull-through) deve ser internado para observação.
- O tamponamento vaginal pode ser considerado em pacientes adolescentes.
- A duração do cateter de Foley é de 3–7 dias para uma vaginoplastia com retalho, e de pelo menos 7 dias para todos os outros reparos.
- Uma pomada à base de petrolato deve ser aplicada ao intróito pelo menos 4 vezes ao dia nas primeiras semanas para criar uma barreira entre as linhas de sutura, a fim de evitar a aderência da roupa íntima à ferida e dos tecidos entre si.
Complicações pós-operatórias
Complicações Imediatas
- Sangramento: pode ser minimizado com tamponamento vaginal em pacientes pós-puberais.6
- Necrose do retalho: rara
- Prefira reparo tardio para evitar fibrose tecidual local
- Infecção da ferida: rara
- Geralmente tratada com antibióticos
- Deiscência de ferida: incomum se a anastomose foi realizada sem tensão
- Pode ser manejada de forma conservadora para permitir cicatrização por segunda intenção
- Retenção urinária: rara
- Se o paciente não consegue urinar, o cateter deve ser substituído por um cateter Coudé. Isto é particularmente importante após vaginoplastia pull-through, pois a parede posterior do UGS é delicada e propensa à formação de falsa via.6
- Formação de fístula: maior risco após uma vaginoplastia pull-through
- Pode ocorrer em qualquer local do trato urinário inferior, mas o local mais comum é na confluência do canal comum onde a vagina foi separada
Complicações tardias e resultados cirúrgicos
Os dados sobre desfechos de longo prazo após a reconstrução isolada do seio urogenital são muito limitados. A maior parte dos dados sobre os desfechos da vaginoplastia provém de pacientes com hiperplasia adrenal congênita, que tendem a apresentar anatomia mais complexa e requerer outros procedimentos adjuvantes.6
- Vaginoplastia com retalho:
- Sem relatos de incontinência, o que está de acordo com a dissecção mínima necessária
- Pode haver micção pela vagina devido a um meato hipospádico
- Crescimento de pelos intravaginais a partir do retalho cutâneo perineal, o que pode interferir com a relação sexual
- Estenose vaginal:
- A taxa varia amplamente de 3% a 83%
- A taxa de revisão cirúrgica também apresenta ampla variação, de 25% a 86%
- Geralmente pode ser manejada com dilatação vaginal
- Os dados de desfechos da vaginoplastia PUM, TUM e pull-through são limitados
- Pode apresentar maior risco de incontinência, dada a extensão da dissecção do assoalho pélvico necessária.6
- Parece ter menor risco de estenose vaginal
- Desfechos do ASTRA:
Pontos-chave
- Seio urogenital isolado é uma anomalia congênita rara do sistema urogenital feminino em que a uretra e a vagina não se separam durante o desenvolvimento, formando um canal comum.
- O diagnóstico é feito principalmente no exame físico da genitália externa de uma paciente do sexo feminino, mostrando um único orifício perineal.
- Cistoscopia e exame sob anestesia são geralmente realizados para compreender melhor a anatomia. Genitograma é opcional.
- As técnicas de reconstrução cirúrgica dependem do comprimento do canal comum. Canais mais longos exigem técnicas cirúrgicas mais invasivas para mobilizar a uretra e a vagina até a pele perineal. Canais mais curtos são mais comuns e apresentam excelentes resultados após a reconstrução.
Conclusão
Seio urogenital é uma malformação congênita rara que resulta na confluência da uretra e da vagina em um canal comum que se apresenta como um único orifício perineal. Isso é comumente encontrado em pacientes com hiperplasia adrenal congênita. A avaliação diagnóstica e a reconstrução podem variar, mas, em geral, para canais comuns curtos, os desfechos são favoráveis no curto a médio prazo. As pacientes devem ser acompanhadas até a puberdade para avaliar a adequação da vagina antes da menarca.
Leituras recomendadas
- Carrasco A. Urogenital Sinus Reconstruction. Surgical Techniques in Pediatric and Adolescent Urology. New Delhi: Jaypee Brothers; 2020.
Referências
- Rink RC. Surgical Management of Differences of Sexual Differentiation and Cloacal and Anorectal Malformations. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, Wein AJ, editors. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021.
- Clavelli A. Persistent Urogenital Sinus. J Anat Soc India 2004; 59 (2): 1. DOI: 10.1016/s0003-2778(10)80034-6.
- Urogenital Sinus. The Fetal Medicine Foundation; . DOI: 10.1515/iupac.88.1463.
- Rowe CK, Merguerian PA. Developmental Abnormalities of the Genitourinary System. Avery’s Diseases of the Newborn 2023: 1260–1273. DOI: 10.1016/b978-0-323-82823-9.00076-3.
- Grosfeld JL, Coran AG. Abnormalities of the Female Genital Tract. Eur J Pediatr Surg 2006; 2: 1935–1955. DOI: 10.1016/b978-0-323-02842-4.50125-x.
- Carrasco A. Urogenital Sinus Reconstruction. Surgical Techniques in Pediatric and Adolescent Urology. New Delhi: Jaypee Brothers; 2020.
- Ding Y, Wang Y, Lyu Y, Xie H, Huang Y, Wu M, et al.. Urogenital sinus malformation: From development to management. Intractable Rare Dis Res 2023; 12 (2): 78–87. DOI: 10.5582/irdr.2023.01027.
- Tan HH, Tan SK, Shunmugan R, Zakaria R, Zahari Z. A Case of Persistent Urogenital Sinus: Pitfalls and challenges in diagnosis. Sultan Qaboos Univ Med J 2018; 17 (4): 455. DOI: 10.18295/squmj.2017.17.04.013.
- Eapen A, Chandramohan A, Simon B, Putta T, John R, Kekre A. Imaging Evaluation of Disorders of Sex Development. Journal of Gastrointestinal and Abdominal Radiology 2020; 03 (02): 181–192. DOI: 10.1055/s-0039-3402101.
- Vaginoplasty technique for female pseudohermaphrodites. Plast Reconstr Surg 1964; 34 (3): 322. DOI: 10.1097/00006534-196409000-00031.
- Jenak R, Ludwikowski B, González R. Total Urogenital Sinus Mobilization: A Modified Perineal Approach For Feminizing Genitoplasty And Urogenital Sinus Repair. J Urol 2001; 165 (6 Part 2): 2347–2349. DOI: 10.1097/00005392-200106001-00032.
- Yang J, Syed H, Baker Z, Vasquez E. Urogenital Sinus Diagnosed During Workup of Recurrent Urinary Tract Infections: A Case Report. Urology 2023; 174: 165–167. DOI: 10.1016/j.urology.2022.12.031.
- Fares AE, Marei MM, Abdullateef KS, Kaddah S, El Tagy G. Laparoscopically Assisted Vaginal Pull-Through in 7 Cases of Congenital Adrenal Hyperplasia with High Urogenital Sinus Confluence: Early Results. J Laparoendosc Adv Surg Tech A 2019; 29 (2): 256–260. DOI: 10.1089/lap.2018.0194.
- Rink RC, Cain MP. Urogenital mobilization for urogenital sinus repair. BJU Int 2008; 102 (9): 1182–1197. DOI: 10.1111/j.1464-410x.2008.08091.x.
- Hardy Hendren W, Crawford JD. Adrenogenital syndrome: The anatomy of the anomaly and its repair. Some new concepts. J Pediatr Surg 1969; 4 (1): 49–58. DOI: 10.1016/0022-3468(69)90183-3.
- Dòmini R, Rossi F, Ceccarelli PL, Castro RD. Anterior sagittal transanorectal approach to the urogenital sinus in adrenogenital syndrome: Preliminary report. J Pediatr Surg 1997; 32 (5): 714–716. DOI: 10.1016/s0022-3468(97)90012-9.
- Salle JLP, Lorenzo AJ, Jesus LE, Leslie B, AlSaid A, Macedo FN, et al.. Surgical treatment of high urogenital sinuses using the anterior sagittal transrectal approach: a useful strategy to optimize exposure and outcomes. J Urol 2012; 187 (3): 1024–1031, DOI: 10.1016/j.juro.2011.10.162.
- Leite MTC, Fachin CG, Albuquerque Maranhão RF de, Shida MEF, Martins JL. Anterior sagittal approach without splitting the rectal wall. Int J Surg Case Rep 2013; 4 (8): 723–726. DOI: 10.1016/j.ijscr.2013.05.013.
- Huen KH, Holzman SA, Davis-Dao CA, Wehbi EJ, Khoury AE. Taking “Trans-ano-rectal” out of ASTRA: An anterior sagittal approach without splitting the rectum. J Pediatr Urol 2021; 18 (1): 96–97. DOI: 10.1016/j.jpurol.2021.12.007.
- Peña A. Total urogenital mobilization–An easier way to repair cloacas. J Pediatr Surg 1997; 32 (2): 263–268. DOI: 10.1016/s0022-3468(97)90191-3.
Ultima atualização: 2025-09-21 13:35