
52: Traumatismo renal
Este capítulo durará aproximadamente 6 minutos para leer.
Introducción
La lesión renal se considera una de las lesiones del tracto urinario más frecuentes observadas tanto en traumatismos cerrados como penetrantes. La mayoría son lesiones cerradas, con menos del 10% penetrantes. Los niños tienen un mayor riesgo de lesiones renales por traumatismo cerrado que los adultos debido a una menor grasa perirrenal de sostén y a que las costillas torácicas son más flexibles, lo que permite que la fuerza del traumatismo se transmita a los órganos sólidos.
El traumatismo renal rara vez ocurre como una lesión aislada y con mayor frecuencia se asocia a lesiones de otros órganos sólidos o se presenta como parte de un politraumatismo. El traumatismo renal se clasifica en 5 grados según su gravedad, y la mayoría de las lesiones son de bajo grado.
Anatomía
Es esencial comprender la anatomía del riñón al diagnosticar, clasificar y manejar la lesión renal. Cada riñón está situado dentro de la fascia de Gerota, que rodea el espacio renal, el cual está lleno de grasa perirrenal. Actúa como un amortiguador protector del riñón y es menos abundante en los niños.
Composición del hilio renal de anterior a posterior, se observa la vena renal como la más anterior, seguida de la arteria renal, y el uréter es la estructura más posterior.
La vena renal derecha suele ser más corta debido a su proximidad a la vena cava inferior. Tanto las venas gonadales como las suprarrenales drenan directamente en la vena cava inferior en el lado derecho. En cambio, en el lado izquierdo, la vena renal izquierda suele ser más larga y recibe tanto la vena gonadal izquierda como la vena suprarrenal izquierda.
Cada arteria renal se origina directamente de la aorta y se divide en cinco ramas: apical, superior, media, inferior y posterior. Ocasionalmente, ramas accesorias se originan directamente de la aorta.
Signos sugestivos de traumatismo renal:
- Hematuria
- Equimosis en el flanco
- Herida penetrante en la región
- Costillas fracturadas (especialmente las inferiores)
- Masa abdominal
- Dolor a la palpación abdominal
El concepto de “hematuria significativa” después de un traumatismo es objeto de debate en niños.1 Mientras que algunos autores consideran un punto de corte de >5 hematíes/CGA; otros abogan por >50 hematíes/CGA. Sin embargo, la hematuria por sí sola no es un marcador fiable de lesión renal. Además, el grado de** hematuria no se correlaciona con el grado de lesión**.
Con esto en mente, otros recomiendan investigar cualquier hematuria (microscópica o macroscópica) en cualquier niño con traumatismo abdominal cerrado asociado a un mecanismo de desaceleración (MVC, atropello de peatón, caída desde altura).1
Estudios diagnósticos
Ante la sospecha de lesión renal, la ecografía es la herramienta inicial para el manejo. Como se indicó antes, muchas lesiones renales ocurren en el contexto de traumatismo abdominal cerrado para los cuales los protocolos actuales incluyen como estudio de imagen inicial la ecografía FAST ,2,3 Esta ecografía proporcionará la imagen inicial de que el riñón posiblemente esté siendo afectado por el evento traumático.
Una vez diagnosticado el traumatismo renal, deben realizarse estudios más específicos para evaluar la extensión de la afectación del riñón. Entre el arsenal diagnóstico del médico, lo siguiente puede ayudar a determinarlo.
- US (ultrasonido): la US con Doppler puede usarse en aquellos con traumatismo muy leve y menor sospecha de lesión significativa, pero no puede distinguir orina extravasada de sangre y no puede visualizar con precisión el pedículo vascular.
- IVP (Pielografía intravenosa) se utilizaba ampliamente en el pasado y se usa actualmente cuando no hay Tomografía Computarizada disponible. Puede realizarse tanto en la sala de trauma como en el quirófano. Se administra un contraste intravenoso de 2 mL/kg y se toma una radiografía a los 10 minutos. Es útil para diagnosticar la funcionalidad de los riñones y la presencia de cualquier extravasación.
-
CT con contraste IV es el estándar de oro actual: Es válida para evaluar la anatomía y la funcionalidad de los riñones y del sistema renovascular de manera eficiente en el tiempo.
- Idealmente, una CT de “cuatro fases” con contraste IV visualiza las fases arterial, nefrográfica y pielográfica; sin embargo, esto rara vez se realiza debido al aumento de radiación asociado con cuatro pasadas.
- La CT estándar obtiene la fase arterial y la fase cortical temprana… lo que puede pasar por alto algunas lesiones parenquimatosas o del sistema colector.1
- Los hallazgos de la CT por sí solos NO determinan el manejo.4
- Angiografía o urografía IV intraoperatoria también son herramientas de imagen en algunos casos.
Clasificación
La Escala de Lesiones de Órganos de la Asociación Estadounidense para la Cirugía del Trauma (AAST-OIS) es el sistema de graduación más común utilizado para las lesiones de órganos sólidos, incluido el riñón.5 El sistema de graduación se basa en la tomografía computarizada y en los hallazgos quirúrgicos. Este sistema de graduación se adaptó de la población adulta y todavía se utiliza en el trauma pediátrico. Se divide en 5 grados: los grados 1-2 se consideran de bajo grado, mientras que 4-5 son de alto grado.
- Grado I – Contusión o hematoma subcapsular no expansivo
- Grado II – Hematoma perirrenal con laceración parenquimatosa < 1cm de profundidad
- Grado III – Como el Grado II con laceración >1cm de profundidad. No se compromete el sistema colector.
- Grado IV – Laceración que compromete el sistema colector (urinoma perirrenal)
- Grado V – Laceración parenquimatosa que compromete el sistema colector (riñón estallado) y/o laceración de la vena/arteria renal principal o avulsión de la arteria principal o trombosis de la vena renal.
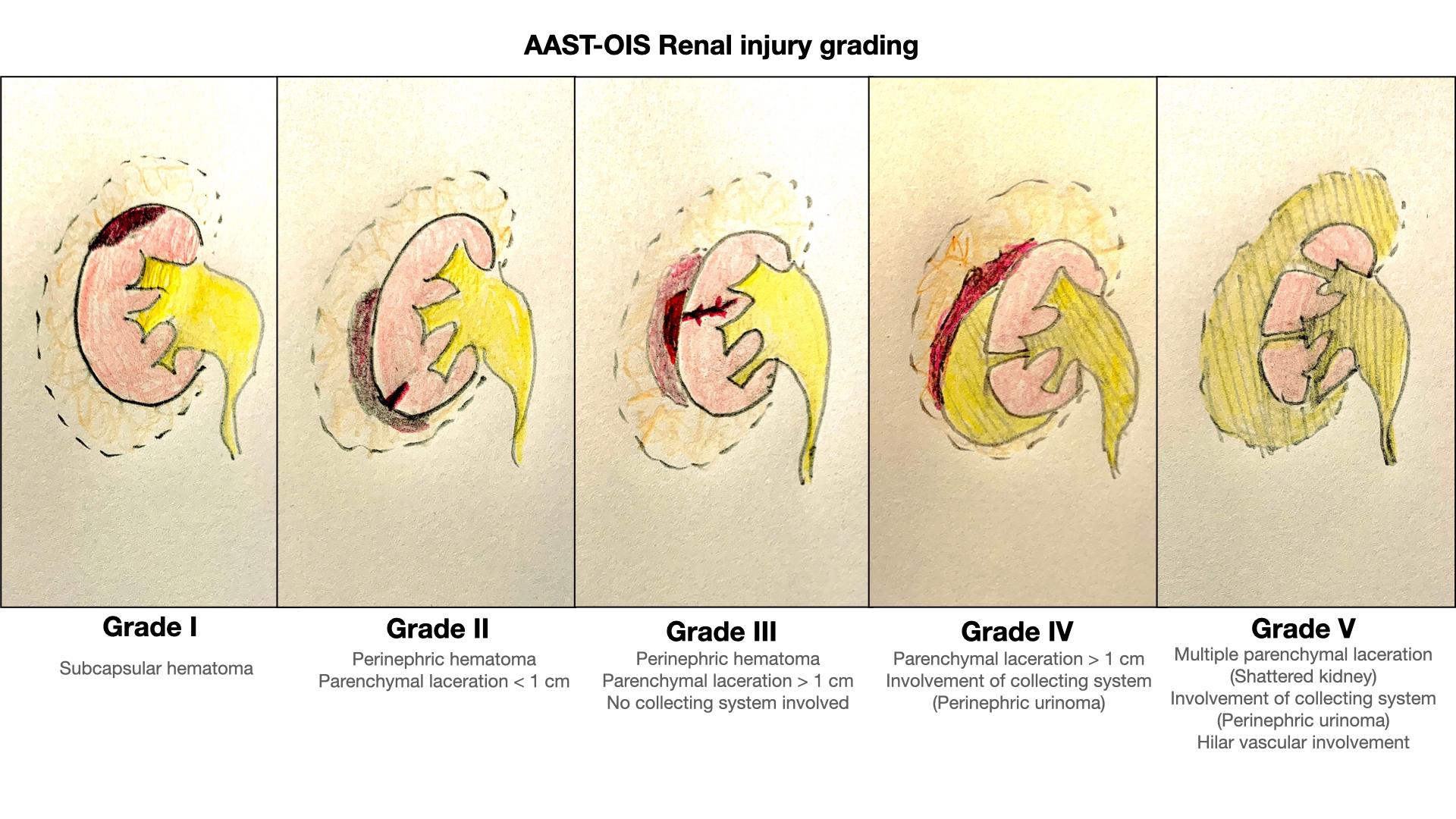
Figura 1 Sistema de graduación del traumatismo renal AAST-OIS.
Posibles complicaciones
- Extravasación urinaria (complicación más común, particularmente con grados IV y V)
- Urinoma
- Puede presentarse de forma aguda o semanas-meses más tarde
- Los signos habituales son dolor, fiebre, íleo y una masa palpable
- Hemorragia secundaria
- Sangrado tardío, que ocurre en 13–25% de las lesiones de grado III–V
- Suele observarse en las primeras 2–3 semanas después del traumatismo
- Absceso perinéfrico (raro)
- Formación de fístula AV (rara y exclusivamente por heridas por arma blanca)
- Pseudoaneurisma
- Divertículos caliciales
- Deterioro de la función renal
- Hipertensión
Manejo
El primer determinante para el manejo es el estado hemodinámico. Los pacientes estables pueden proceder a completar los estudios para un posible manejo conservador (no quirúrgico). Los pacientes hemodinámicamente inestables que no responden a la reanimación con líquidos deben someterse a un manejo quirúrgico urgente.
En un niño alerta y comunicativo con síntomas mínimos y sin hallazgos físicos preocupantes que tiene <50 eritrocitos/CGA, puede ser razonable la observación o una ecografía de cribado con Doppler, en lugar de solicitar una TC únicamente para la evaluación renal.1
Una vez diagnosticado el daño renal secundario al traumatismo, se recomienda establecer un drenaje urinario completo a bajas presiones. Un catéter transuretral simple en la vejiga, solo como medida inicial, es lo más sencillo y eficaz (y a veces lo único necesario).
En general, el traumatismo renal en los niños se maneja de forma conservadora, incluso en lesiones de mayor grado.1,4,6 En concreto, todas las lesiones de Grado I–III pueden manejarse de forma no operatoria.7 Existe evidencia de que los Grados IV y V también pueden manejarse de forma conservadora.4 Estas lesiones de mayor grado requieren un enfoque cuidadoso y personalizado para cada individuo.1 Esto es particularmente relevante en pacientes pediátricos donde las lesiones de Grado IV son una heterogénea población.3
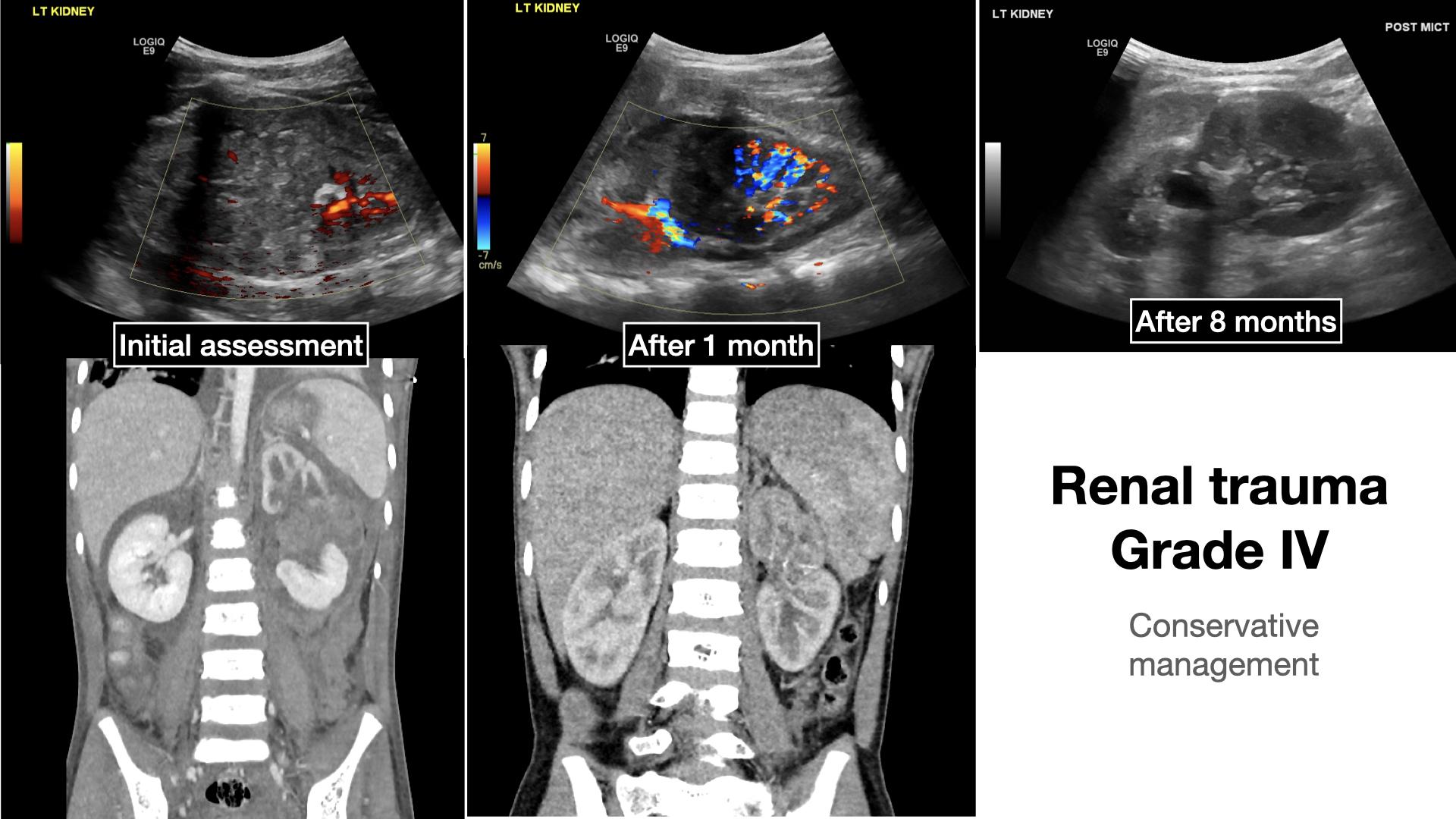
Figura 2 Paciente de ejemplo con traumatismo renal de grado IV en la presentación inicial, después de 1 mes y después de 8 meses.
Siempre debe tenerse en cuenta que el sistema de clasificación de la American Association for the Surgery of Trauma no es perfecto y genera controversias.6 La razón es que este sistema de clasificación se basa predominantemente en la población adulta y puede no reflejar adecuadamente a la población pediátrica.6 Algunos subdividen aún más el Grado IV por este motivo.
Se recomienda la cirugía para:1
- Pacientes hemodinámicamente INESTABLES
- Aquellos con lesiones intraabdominales PENETRANTES graves.
Puede ser necesaria la cirugía o la radiología intervencionista para:1
- Extravasación urinaria masiva en grados IV–V
- Extensión (>20%) de tejido no viable
- Lesión arterial
- Estadificación incompleta
Independientemente de la clasificación inicial, si se establece un manejo expectante, el seguimiento continuo del paciente se recomienda para evaluar si puede presentar lesión renal tardía. Cualquier cambio en los signos vitales y/o hematuria de nueva aparición debe reevaluarse de forma inmediata mediante estudios de imagen.
Puntos clave
- ¡No pase por alto la hematuria! ¡No todos necesitan una tomografía computarizada (TC), en todo caso!
- ¡Conozca las limitaciones de sus estudios de imagen! No puede ver lo que no se estudia por imágenes
- A menos que haya inestabilidad hemodinámica, por lo general, todos los traumatismos pueden manejarse de manera no operatoria
- Evalúe y reevalúe a su paciente, el cuadro clínico puede cambiar
Referencias
- Fernández-Ibieta M. Renal Trauma in Pediatrics: A Current Review. Urology 2018. DOI: 10.1016/j.urology.2017.09.030.
- Ollerton JE, Sugrue M, Balogh Z, D’Amours SK, Giles A, Wyllie P. Focused Assessment with Sonography in Trauma. J Trauma 2006; 60 (4): 785–791. DOI: 10.1017/cbo9780511544811.052.
- Root JM, Abo A. Cohen J. Point-of-Care Ultrasound Evaluation of Severe Renal Trauma in an Adolescent. Pediatr Emerg Care 2018; 34: 286–287. DOI: 10.1097/pec.0000000000001406.
- LeeVan E, Zmora O, Cazzulino F, Burke RV, Zagory J, Upperman JS. Management of pediatric blunt renal trauma: A systematic review. J Trauma Acute Care Surg 2016. DOI: 10.1097/ta.0000000000000950.
- Ballon-Landa E, Raheem OA, Fuller TW, Kobayashi L, Buckley JC. Renal Trauma Classification and Management: Validating the Revised Renal Injury Grading Scale. J Urol 2019; 202 (5): 994–1000. DOI: 10.1097/ju.0000000000000358.
- Murphy GP, Gaither TW, Awad MA, Osterberg EC, Baradaran N, Copp HL, et al.. Management of Pediatric Grade IV Renal Trauma. Curr Urol Rep 2017; 18: 23. DOI: 10.1007/s11934-017-0665-z.
- Bartley JM, Santucci RA. Computed tomography findings in patients with pediatric blunt renal trauma in whom expectant (nonoperative) management failed. Urology 2012; 80 (6): 1338–1343. DOI: 10.1016/j.urology.2012.07.077.
Última actualización: 2025-09-21 13:35