
35: Anomalías del prepucio
Este capítulo durará aproximadamente 17 minutos para leer.
Embriología
La embriología de los genitales externos masculinos es un proceso complejo. Antes de la novena semana de gestación, el desarrollo de los genitales externos es similar en ambos sexos. Durante las semanas 9 a 13 de gestación, la producción de testosterona por las células de Leydig, su conversión a dihidrotestosterona (enzima 5α-reductasa) y la interacción con los receptores de andrógenos darán como resultado la diferenciación normal del tubérculo genital, los pliegues y las tumefacciones.
La estimulación androgénica provoca la elongación del tubérculo genital, así como la fusión de los pliegues uretrales, creando la uretra de proximal a distal. El prepucio se forma entre la 13a y la 18a semana de gestación, solapándose con el desarrollo de la uretra. Los pliegues prepuciales se desplazan desde la base del cuerpo del pene hacia distal hasta su fusión con el glande, creando el rafe medio. La subsiguiente descamación normal de la fusión epitelial entre el glande y el prepucio permitirá la separación del prepucio y su retracción futura.1
Fimosis
La fimosis es la incapacidad de retraer el prepucio exponiendo el glande. Fimosis fisiológica existe debido a las adhesiones naturales entre la piel prepucial interna y el glande y, en algunos casos, debido a la presencia de un anillo constrictivo (Figura 1). La separación normal se produce por la acumulación normal de detritos epiteliales llamada esmegma y por las erecciones intermitentes durante los primeros años de vida.

Figura 1 Fimosis fisiológica en un niño de 1 año.
La fimosis fisiológica disminuye con la edad: solo el 10% permanecerá con esta condición a los 3 años y menos del 1% a los 17 años de edad. La fimosis primaria suele resolverse espontáneamente durante la infancia.1,2
Es importante diferenciar la fimosis de las adherencias del glande (adherencias balanoprepuciales), que son uniones entre la cara interna del prepucio y el glande. También pueden ser secundarias, tradicionalmente después de una circuncisión, entre la línea de incisión y el glande. Las adherencias fisiológicas se resolverán espontáneamente debido a la separación epitelial y a las erecciones durante la infancia. En pacientes con adherencias prepuciales asintomáticas se debe evitar la retracción manual. Con poca frecuencia, las adherencias persistentes en pacientes mayores pueden ser liberadas en el consultorio tras la aplicación de analgésicos tópicos.1,2
La fimosis secundaria puede resultar de diferentes causas como retracciones forzadas y traumáticas con formación cicatricial secundaria o la presencia de balanitis xerótica obliterante (BXO) (Figura 2). Debe promoverse durante la consulta la prevención de la fimosis secundaria evitando la retracción forzada.

Figura 2 Balanitis xerótica obliterante.
Se han propuesto diferentes sistemas de gradación para estratificar la gravedad de la fimosis. Uno de ellos es el propuesto por Sookpotarom et al., que va desde un grado 0 con retracción completa y total hasta un grado sin retracción (grado 5) (Figura 3).3
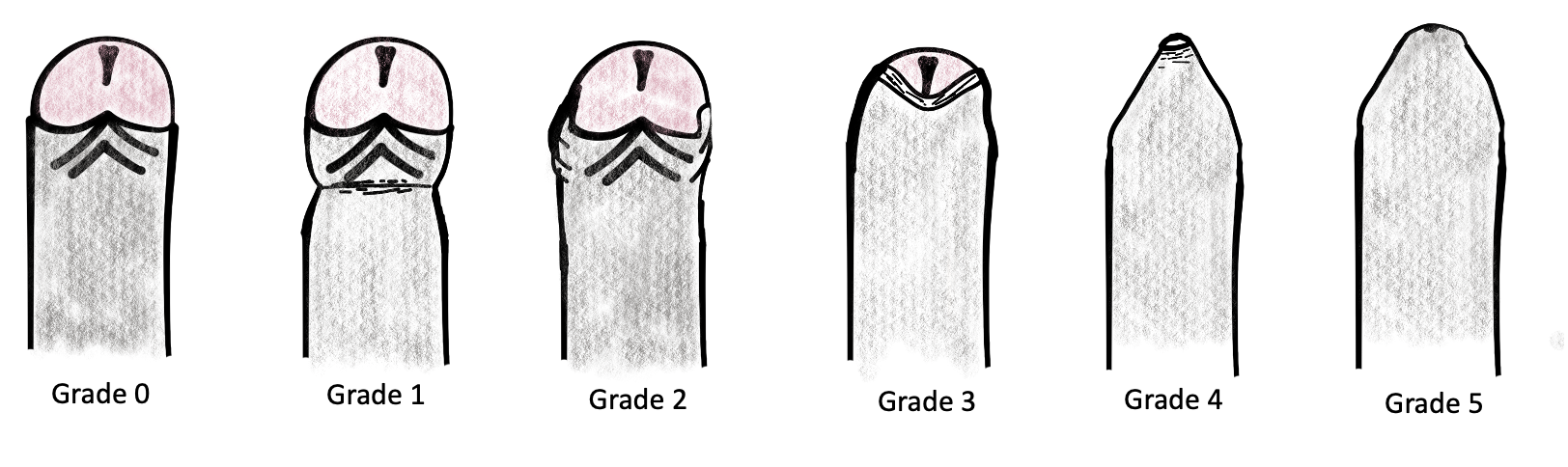
Figura 3 Escala de clasificación de la retracción del prepucio en la fimosis de Sookpotarom et al.
Las afecciones relacionadas con el pene no circuncidado se muestran a continuación.
Balanitis y postitis
Estos son procesos inflamatorios del glande y del prepucio, respectivamente, secundarios a una higiene deficiente en un paciente con fimosis. Estas afecciones suelen presentarse simultáneamente. Una higiene meticulosa es la piedra angular de la prevención. Los antecedentes de estos episodios deberían fomentar un manejo prepucial más cuidadoso.
Parafimosis
Es el atrapamiento del prepucio detrás del glande, produciendo dolor, hinchazón, edema e incluso necrosis del prepucio si no se reduce a tiempo (Ver más adelante parafimosis).
ITU
La fimosis provoca colonización de la piel prepucial interna y perimeatal por uropatógenos, lo que aumenta el riesgo de ITU. La circuncisión reduce este riesgo de ITU, con un riesgo relativo de 4.5 en lactantes no circuncidados frente a circuncidados < 1 mes de edad, y un riesgo relativo de 3.7 durante el primer año de vida. El número necesario para tratar calculado es mayor de 100 para prevenir una ITU, pero este número se reduce a 4 en niños con reflujo vesicoureteral dilatado (VUR) (grado 3–5). Los pacientes con fimosis más grave también presentan una mayor prevalencia de ITU en comparación con los pacientes con fimosis de grado leve.4,5 La circuncisión debe considerarse como una opción en pacientes con VUR para reducir el riesgo de ITU según la Asociación Americana de Urología.4
Cáncer
La fimosis se ha descrito como un factor de riesgo significativo para el carcinoma de pene.1
Tratamiento
En pacientes asintomáticos con fimosis fisiológica, el manejo activo debería iniciarse después de los 2-3 años de edad o según la preferencia del cuidador.2 El manejo médico o quirúrgico de la fimosis debe fomentarse en algunas situaciones, como: postitis, balanitis, fimosis secundaria, BXO o infecciones del tracto urinario recurrentes.
Tratamiento médico con corticosteroides tópicos
El manejo prepucial combinado con el uso de corticosteroide tópico y retracción manual ha mostrado una alta tasa de éxito.2 La crema de betametasona (0,05%) es uno de los tratamientos tópicos más frecuentemente utilizados en la fimosis primaria sintomática o persistente sin cambios patológicos del prepucio. Se cree que el mecanismo fisiológico es secundario a la mejoría de la elasticidad de la piel prepucial.
La Asociación Europea de Urología recomienda el uso de corticosteroides tópicos en caso de persistencia de fimosis fisiológica con una tasa de éxito del 80% y una tasa de recurrencia del 17%.2 El protocolo más común es la administración de ungüento dos veces al día por un período mínimo de 4 a 8 semanas.
Circuncisión neonatal
La circuncisión electiva durante el período neonatal es un tema de debate controvertido. La Academia Americana de Pediatría, en el Grupo de Trabajo publicado en 2012, hizo hincapié en que no debe recomendarse la circuncisión rutinaria para todos los recién nacidos varones, pero los beneficios son suficientes para justificar el acceso a este procedimiento para las familias que lo consideren.1
Uno de los puntos más importantes al realizar este tipo de circuncisión es la analgesia y la anestesia local. Se recomiendan diferentes opciones, como anestesia tópica, bloqueo del nervio dorsal del pene o un bloqueo en anillo del pene. Se han desarrollado varias técnicas y dispositivos para facilitar este procedimiento, como el Gomco Clamp, el Mogen Clamp y el dispositivo Plastibell.
Es imperativo no realizar la circuncisión neonatal en pacientes con otras condiciones urológicas que requerirán un prepucio íntegro para su corrección quirúrgica en el futuro, como el hipospadias. Para excluir este tipo de anomalías, se debe realizar una exploración genital adecuada con una separación completa del prepucio del glande antes del procedimiento.
Balanitis xerótica obliterante
BXO (también denominado liquen escleroso) es una enfermedad inflamatoria crónica que puede afectar el prepucio, el glande y la uretra. El nombre deriva de los tres componentes de la enfermedad, que son balanitis (inflamación crónica del glande del pene), xerótica (aspecto anormalmente seco de la lesión) y obliterante (asociación con endarteritis ocasional).6
La incidencia reportada es de 0,4 casos/1000 varones por año y la prevalencia publicada de BXO en pacientes fimóticos varía entre 9 y 50%. Se ha informado que la edad promedio al momento de la presentación es de 8,9 - 10,6 años, con un pico de incidencia entre los 9 y 11 años de edad.7,8,9
En una publicación reciente de Filho et al., se diagnosticó histológicamente BXO en el 32% de los pacientes con fimosis sin sospecha clínica de BXO tras la circuncisión. El grado de fimosis no se correlacionó con la presencia de BXO.7,9
El diagnóstico es principalmente clínico. En los casos leves con BXO, pueden encontrarse áreas de decoloración blanquecina grisácea en el glande o en la lámina interna del prepucio (Figura 2). A medida que esta afección progresa, la piel se vuelve inelástica, con placas blanquecinas descoloridas junto con fimosis fibrótica progresiva. En los casos más graves, pueden observarse ulceración y afectación del meato y la uretra.6,9
La mayoría de los pacientes pediátricos son asintomáticos, pero algunos de ellos refieren disuria o episodios de retención urinaria y balonamiento del prepucio. El diagnóstico se confirma mediante histología que revela hiperqueratosis y atrofia de la capa basal de la epidermis, con pérdida de fibras elásticas y alteraciones del colágeno con infiltrado inflamatorio.
La etiología de esta enfermedad aún es desconocida. Existe evidencia que respalda un mecanismo autoinmunitario subyacente. Las lesiones se caracterizan histológicamente por una abundancia de linfocitos T citotóxicos autorreactivos infiltrantes y por un metabolismo alterado de la matriz extracelular. Asimismo, se han detectado autoanticuerpos contra proteínas de la matriz extracelular en el suero de los pacientes afectados. Las causas infecciosas, la predisposición genética, la irritación crónica por exposición a la orina y las influencias hormonales son otras teorías postuladas.6
Manejo de BXO
El tratamiento más aceptado y recomendado para la BXO es la circuncisión, que puede ser un tratamiento definitivo en muchos casos (Figura 4). Sin embargo, un número significativo de centros están realizando cirugía conservadora del prepucio, como la preputioplastia, como una opción quirúrgica menos agresiva. Wilkinson et al comunicaron sus resultados comparando niños con BXO tratados con preputioplastia combinada con inyecciones de triamcinolona en las lesiones de forma intraoperatoria frente a aquellos tratados con circuncisión. Durante el seguimiento, el 19% de los niños circuncidados requirió cirugía meatal posterior, en comparación con el 6% de aquellos sometidos a preputioplastia. La tasa de éxito de la cirugía conservadora comunicada fue del 81%.10 Recientemente, Green et al publicaron un estudio similar que comparó la circuncisión y la preputioplastia en pacientes con BXO, sin encontrar diferencias significativas en la tasa de procedimientos complementarios a nivel del meato, la tasa de reintervención, la infección posoperatoria ni la hemorragia secundaria entre los grupos de preputioplastia y circuncisión. Concluyen que la preputioplastia con esteroides intralesionales puede ser un tratamiento quirúrgico de primera línea válido para la BXO.11
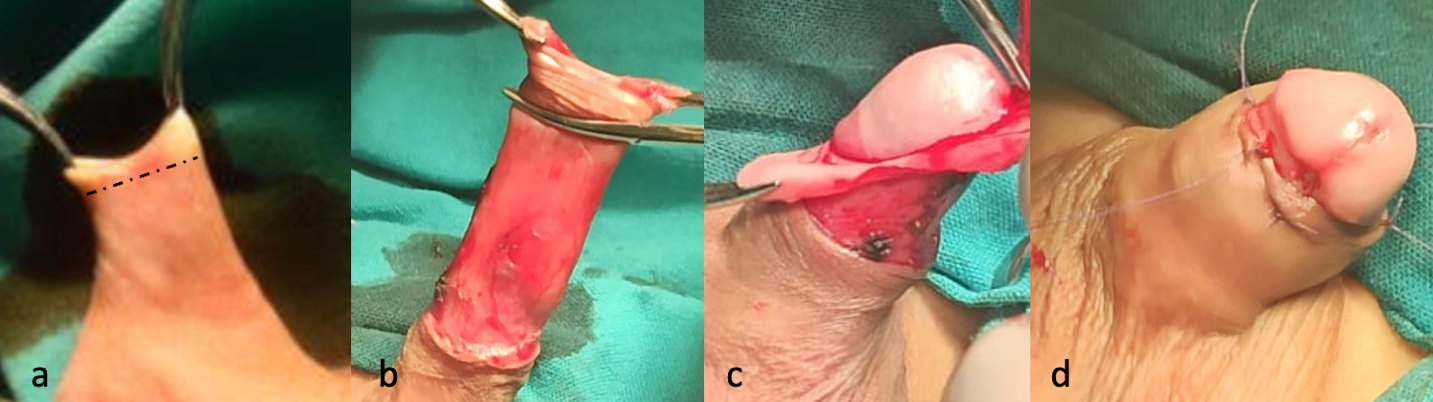
Figura 4 Circuncisión quirúrgica: (a) Se realiza una incisión cutánea por debajo del anillo fimótico (b) Se diseca el prepucio interno del prepucio externo (c) Resección del prepucio interno dejando un collar mucoso de 5 mm (d) Sutura entre el collar mucoso y la piel con sutura reabsorbible.
Una revisión sistemática realizada por Folaranmi que abordaba la propuesta de utilizar corticosteroides tópicos como alternativa a la circuncisión encontró que la tasa de éxito promedio de respuesta fue del 35% para el tratamiento tópico en pacientes con BXO. El único ensayo clínico aleatorizado, doble ciego y prospectivo incluido en esta revisión demostró que ningún paciente con BXO respondió a los corticosteroides tópicos y que todos requirieron circuncisión.9
El uso de inmunosupresores tópicos como el tacrolimus también se ha descrito. Ebert et al informaron que la aplicación de ungüento de tacrolimus al 0,1% tras la circuncisión resultó en recurrencia en el 9%, la cual se trató con éxito con un nuevo ciclo del fármaco. Concluyen que esta terapia es una opción tras la cirugía si existe riesgo de un desenlace complicado causado por afectación del meato o del glande.6
Cuando se detecta afectación meatal por BXO, debe realizarse una endoscopia para determinar la extensión del proceso inflamatorio. Una meatoplastia combinada con corticoides tópicos o inmunosupresores es obligatoria en estos casos.
En algunos pacientes, especialmente con antecedentes de estenosis meatal recurrente o una respuesta deficiente al tratamiento local, deberían considerarse cirugías reconstructivas con injerto de mucosa bucal.6
Complicaciones
La tasa de complicaciones de la circuncisión se ha informado entre 0,2% y 5%. Las complicaciones pueden ocurrir inmediatamente después del procedimiento o muchos años después. La complicación más frecuente descrita es el sangrado, que es más común en niños mayores. Aunque la compresión será eficaz para controlar esta complicación en la mayoría de los casos, puede requerirse cauterización en algunos de ellos (Figura 5).1

Figura 5 Hematoma posoperatorio. La hemorragia es la complicación más frecuente después de la circuncisión.
La resección cutánea excesiva después de la circuncisión puede producir un pene atrapado por fibrosis cicatricial. Puede tratarse con betametasona en conjunto con retracción manual como primera opción. En algunos casos, pueden ser necesarias incisiones de relajación o una reparación formal con colgajos cutáneos.
La estenosis meatal ocurre casi únicamente en pacientes tras la circuncisión, y es consecuencia de una reacción inflamatoria local y de la formación de tejido cicatricial. Los pacientes con sospecha de estenosis meatal pueden referir dolor peneano al inicio de la micción y/o un chorro urinario estrecho.
Parafimosis
La parafimosis es una emergencia urológica que afecta a varones no circuncidados, en la que el prepucio del pene queda retraído detrás del surco coronal, lo que produce estrangulación del glande (Figura 6). Si no se reduce a tiempo, el prepucio retraído puede causar edema prepucial y del glande, congestión venosa y, finalmente, necrosis y gangrena del glande. Esta afección puede presentarse a cualquier edad, pero es más frecuente en adolescentes, con una incidencia reportada del 0,7% en niños no circuncidados.12,13,14

Figura 6 Parafimosis.
El manejo consiste en reducir el edema del pene y del glande, seguido de reposicionar el prepucio sobre el glande en su posición anatómica. Antes de intentar cualquier maniobra, es muy importante asegurar una analgesia adecuada. Los anestésicos locales de uso más común son el gel de lidocaína al 2% o la crema EMLA (lidocaína al 2,5% y prilocaína al 2,5%). Los analgésicos opioides por vía oral o intravenosa pueden utilizarse en combinación con anestésicos tópicos para lograr un control óptimo del dolor.
Se han descrito varias técnicas no invasivas para reducir la parafimosis. Cuando las medidas conservadoras fracasan, pueden emplearse métodos más invasivos (Figura 7).
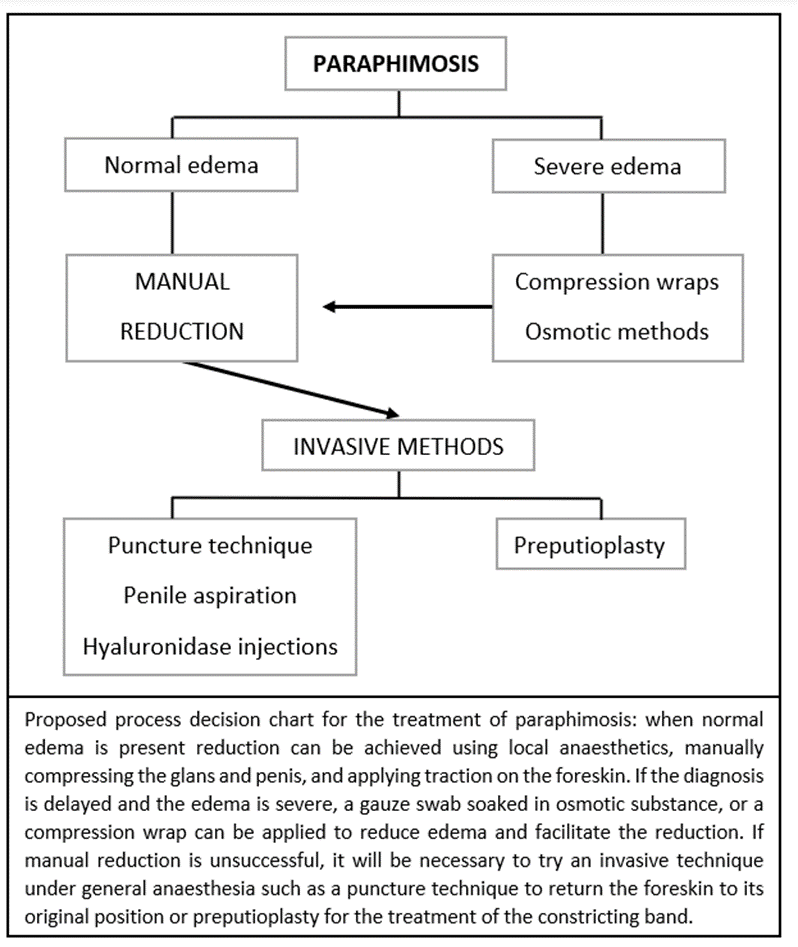
Figura 7 Algoritmo de manejo de la parafimosis.
Técnicas no invasivas:
- Reducción manual: Primero, se aplica presión circunferencial con una mano enguantada sobre la parte distal del pene durante varios minutos para reducir el edema. Tras unos minutos de compresión, se colocan ambos pulgares comprimiendo el glande, mientras se aplica contratracción sobre el prepucio justo proximal a la banda constrictiva tensa. Esta técnica puede facilitarse aplicando hielo sobre la zona algunos minutos antes de iniciar la maniobra.
- Vendajes compresivos: un vendaje flexible autoadherente se envuelve alrededor del pene comenzando en el glande y se retira después de 5 a 20 min. El vendaje genera una presión constante y suave que empuja el líquido proximalmente por debajo de la banda constrictiva tensa de tejido. Si no ocurre la reducción espontánea, puede emplearse una reducción manual suave.
- Métodos osmóticos: se utiliza una sustancia con alta concentración de solutos en la superficie del pene y el prepucio, reduciendo el edema de los tejidos y facilitando la reducción. Se envuelven gasas empapadas alrededor del prepucio edematoso, con compresión manual mínima intermitente durante 1 a 2 horas. Se han utilizado varias sustancias para la reducción osmótica de la parafimosis: glicerina, sulfato de magnesio, azúcar granulada, solución de dextrosa al 50% y solución de manitol al 20%.
Métodos invasivos:
- Técnica de punción: Se utiliza una aguja de calibre 26 para realizar aproximadamente 20 orificios de punción en el prepucio, reduciendo el edema para permitir la reducción.15,16
- Aspiración peneana: se aplica un torniquete en el cuerpo del pene y luego se introduce una aguja de calibre 20 paralela a la uretra para aspirar de 3 a 12 ml de sangre del glande. Este procedimiento reduce el volumen del glande para facilitar la reducción manual.16
- Inyecciones de hialuronidasa: se inyecta 1 ml de hialuronidasa a 150 unidades/mL en 2 o 3 sitios del prepucio. La hialuronidasa descompone el ácido hialurónico viscoso del líquido extracelular y facilita la disipación del edema, de modo que luego el prepucio puede retraerse suavemente sobre el glande.
- Prepucioplastia: se identifica el anillo constrictor y se realiza una incisión longitudinal dorsal de 1–2 cm. La liberación del anillo constrictor permite la reducción del edema del glande, para que el prepucio pueda ser reducido. La incisión se sutura luego de manera transversal con suturas reabsorbibles interrumpidas (Figura 8).15,17

Figura 8 Prepucioplastia.
Pene inconspicuo
Es una anomalía peniana en la que un pene con longitud normal (desde la punta del glande hasta el pubis) y diámetro del cuerpo del pene, aparenta ser más pequeño. En esta definición se incluyen diferentes entidades como pene enterrado, pene atrapado o pene con pliegue penoescrotal.1,18
Pene enterrado
Es un pene normal que está oculto por el panículo adiposo suprapúbico. También se denomina pene oculto o escondido
Se han descrito varias categorías diferentes según la causa del ocultamiento:
- Una forma congénita con falta de fijación entre la piel y la base del pene que da lugar a un efecto en tienda. Se cree que su origen embriológico es secundario a un fallo de separación de los planos de migración durante el desarrollo de los genitales externos masculinos. Esta anomalía da como resultado que los cuerpos peneanos queden fijados a la fascia profunda y que el escroto se sitúe alto en la ingle (Figura 9).
- Pueden identificarse fácilmente dos subcategorías según la presencia o no de megaprepucio, que es la asociación de un anillo fimótico con una gran balonización del prepucio interno durante la micción (Figura 10). Este fenómeno puede causar cierto grado de molestia al paciente. La tumefacción hemisférica también se denomina vejiga prepucial y suele ser diagnosticada por los padres durante los primeros meses de vida, quienes necesitan comprimirla manualmente para permitir la salida de la orina a través del orificio fimótico.
- Una forma adquirida debida a la obesidad (Figura 9). Esta debe diferenciarse de la forma transitoria en la primera infancia que se resuelve con el aumento de la edad y la deambulación
- Una forma cicatricial secundaria a cirugías peneanas como la circuncisión.
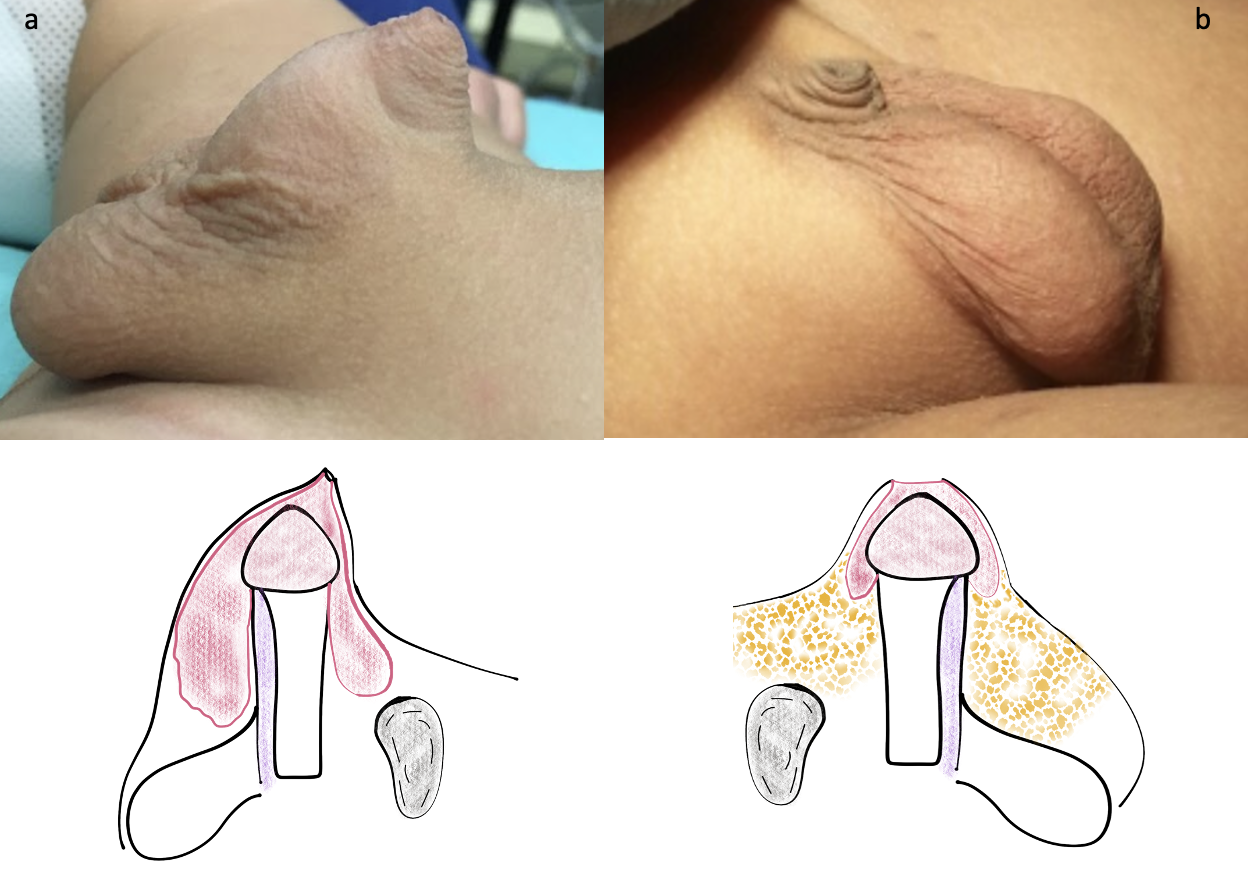
Figura 9 Diferentes formas de pene oculto: (a) Congénito con megaprepucio (b) Secundario a la obesidad
Un paso importante del examen físico es diferenciar esta entidad de un verdadero micropene, que se caracteriza por una longitud del pene estirado anormal.

Figura 10 Megaprepucio con balonamiento de la lámina interna del prepucio durante la micción.
Manejo
En pacientes con pene enterrado secundario a la obesidad, el tratamiento debe centrarse primero en la pérdida de peso mediante un programa de dieta y ejercicio proporcionado por el profesional de atención primaria.
La fimosis fisiológica o secundaria en pacientes sintomáticos con esta afección debería manejarse activamente con corticosteroides tópicos y tracción manual. En aquellos pacientes en los que este tratamiento sea ineficaz, debería planificarse una corrección electiva a partir de los 6 meses de edad o más.
Debe evitarse la circuncisión estándar en este grupo de pacientes debido al pobre resultado cosmético y a la necesidad de procedimientos adicionales en el futuro.
Se han descrito diversas técnicas de corrección quirúrgica de esta malformación, todas con los mismos objetivos:
- Eliminar el anillo prepucial estenótico aliviando los síntomas miccionales
- Restaurar los ángulos penopúbico y penoescrotal
La principal diferencia entre estas técnicas radica en la forma de cubrir la deficiencia de piel del eje peneano, que es una característica frecuente en estos pacientes.
Técnicas quirúrgicas que utilizan piel peneana (Figura 11):
- La infiltración del paquete neurovascular dorsal o el bloqueo caudal con bupivacaína se realizan según la preferencia del anestesiólogo y del cirujano.
- El primer paso es la retracción de la piel, que puede obtenerse con una incisión circunferencial limitada en el anillo estrecho del prepucio externo (Figura 11 b).
- Se coloca una sutura de tracción en el glande para facilitar la disección.
- La piel prepucial y la túnica de Dartos se disecan de la fascia de Buck, liberando el cuerpo del pene de sus adherencias anómalas.
- Se realiza una incisión vertical en la parte ventral de la piel prepucial, lo que permite una mejor exposición y disección en la base del pene, cerca de los huesos púbicos.
- Se reseca por completo el prepucio interno, dejando únicamente un manguito mucoso de 5 mm por debajo del glande (Figura 11 c-d).
- Uno de los pasos más importantes es utilizar al menos 3 puntos de anclaje (a las 3, 9 y 12 horas) entre la piel y la fascia de Buck para crear el ángulo penopúbico. Preferimos suturas no absorbibles como polipropileno 5-0.
- Una incisión transversal ventral a nivel de la unión penoescrotal permite movilizar caudalmente la piel escrotal y reconfigurar el ángulo penoescrotal tras cerrarla de forma vertical (Figura 12 h-i).
- Se deja un vendaje compresivo durante una semana para prevenir el edema de la herida y el sangrado.
- En el abordaje anatómico descrito por Smeulders et al., se realizan una incisión longitudinal ventral y una incisión curva en la línea límite penoescrotal. Luego se lleva a cabo una disección profunda del pene cercana a la fascia de Buck y se reseca el prepucio interno redundante próximo al surco. Un colgajo cutáneo dorsal cuadrilátero se adelgaza y se ancla a la fascia de Buck y luego se envuelve alrededor del pene y se sutura al manguito mucoso. La incisión ventral se sutura de forma transversal creando el ángulo penoescrotal.19
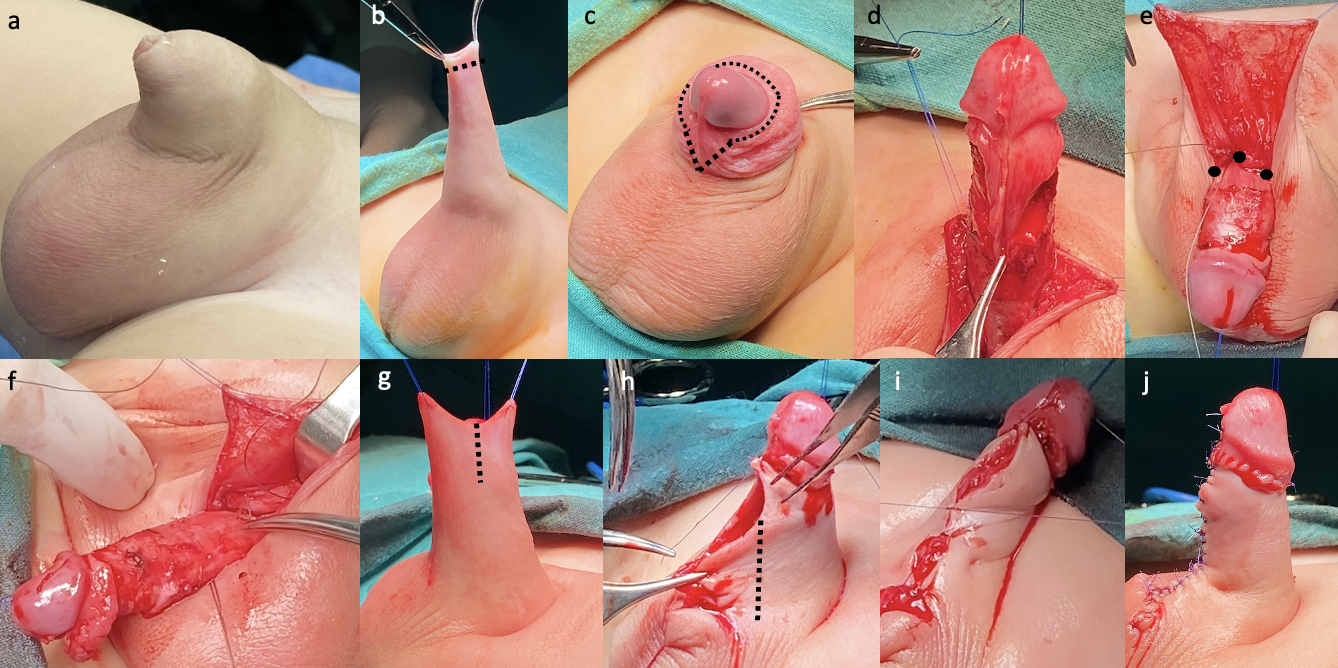
Figura 11 Técnica de reconstrucción quirúrgica del pene oculto con megaprepucio utilizando piel peneana: (b) Incisión en la piel del prepucio externo y retracción del prepucio fimótico (c-d) Escisión del prepucio interno (se deja en su lugar una mucosa ventral en forma de V para una eventual deficiencia cutánea) (e-f) Colocación de suturas no reabsorbibles de anclaje (a las 3, 9 y 12 horas) creando el ángulo penopúbico (g) Los colgajos dorsales de piel de Byars se utilizan para envolver el cuerpo del pene (h-i) Se realiza una incisión ventral para crear el ángulo penoescrotal (j) Apariencia final.
Técnicas quirúrgicas utilizando la lámina interna del prepucio
El concepto de cubrir el eje del pene con el prepucio interno fue descrito por primera vez por Donahue y Keating en 1986. Las técnicas de desplegamiento facilitan la reconstrucción sin tensión utilizando el prepucio interno redundante, que adquirirá en el futuro una apariencia de prepucio.
En la publicación de Ruiz et al., se propuso un abordaje simplificado de esta malformación. Utilizando el concepto de la lámina interna del prepucio de Donahue, se fija la lámina externa del prepucio a la fascia de Buck y la lámina interna, desplegada y conformada, se utiliza para cubrir el cuerpo del pene.20
Por otro lado, Rod et al destacan la importancia de reducir la longitud y la circunferencia del prepucio interno para evitar una apariencia antiestética. También describieron la importancia de resecar el tejido subcutáneo del prepucio interno para reducir la probabilidad de linfedema local.21
La plastia en V ventral es una técnica combinada en la que se realiza una incisión en forma de V en la capa prepucial interna ventral. Esta capa prepucial se dejará en su lugar para interponerse y facilitar el cierre cutáneo en la porción ventral del cuerpo del pene (Figura 12).18

Figura 12 Plastia en V ventral en un paciente de mayor edad con una deficiencia cutánea ventral grave.
También se propuso un abordaje en dos tiempos, en el que se realiza en primer lugar una preputioplastia limitada para aliviar la obstrucción al flujo urinario. Este abordaje preserva la piel prepucial y permite la remodelación fisiológica a medida que el paciente crece. Si se requiere un segundo procedimiento, se programará después del control de esfínteres.
Pene palmeado
Es una afección congénita en la que la piel escrotal se extiende hasta la parte ventral del pene. También se denomina fusión penoescrotal. Es asintomática y produce una apariencia anormal de la superficie ventral del pene.
La corrección quirúrgica consiste en una incisión cutánea transversal sobre el pterigio penoescrotal, creando una separación entre el pene y el escroto, que se cierra en sentido vertical.1,18
[Video 1](#video-1){:.video-link}. Reparación quirúrgica del pene enterrado
Referencias
- L. P, J P. Management of abnormalities of the external genitalia in boys. 44: 871–904 10. DOI: 10.1016/b978-1-4160-6911-9.00131-6.
- Hoen LA ’t, Bogaert G, Radmayr C, Dogan HS, Nijman RJM, Quaedackers J, et al.. Update of the EAU/ESPU guidelines on urinary tract infections in children. Eur Urol 2021; 79: S446–s448. DOI: 10.1016/s0302-2838(21)00695-3.
- Sookpotarom P, Asawutmangkul C, Srinithiwat B, Leethochawalit S, Vejchapipat P. Is half strength of 0.05 % betamethasone valerate cream still effective in the treatment of phimosis in young children? Pediatr Surg Int 2013; 29 (4): 393–396. DOI: 10.1007/s00383-012-3253-9.
- AUA Practice Guidelines Committee. Management and Screening of Primary Vesicoureteral Reflux in Children. 2017.
- Holzman SA, Chamberlin JD, Davis-Dao CA, Le DT, Delgado VA, Macaraeg AM, et al.. Faculty Opinions recommendation of Retractable foreskin reduces urinary tract infections in infant boys with vesicoureteral reflux. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2021; 7 (2): 09 1–209 6. DOI: 10.3410/f.739509971.793583981.
- Celis S, Reed F, Murphy F, Adams S, Gillick J, Abdelhafeez AH, et al.. Faculty Opinions recommendation of Balanitis xerotica obliterans in children and adolescents: a literature review and clinical series. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2014; 0 (1): 4–9. DOI: 10.3410/f.718196548.793513188.
- Aziz Filho AM, Azevedo LMS de, Rochael MC, Jesus LE de. Frequency of lichen sclerosus in children presenting with phimosis: A systematic histological study. J Pediatr Urol 2022; 18 (4): 529.e1–529.e6. DOI: 10.1016/j.jpurol.2022.06.030.
- Jayakumar S, Antao B, Bevington O, Furness P, Ninan GK. Balanitis xerotica obliterans in children and its incidence under the age of 5 years. J Pediatr Urol 2012; 8 (3): 272–275. DOI: 10.1016/j.jpurol.2011.05.001.
- Folaranmi SE, Corbett HJ, Losty PD. Does application of topical steroids for lichen sclerosus (balanitis xerotica obliterans) affect the rate of circumcision? A systematic review. J Pediatr Surg 2018; 53 (11): 2225–2227. DOI: 10.1016/j.jpedsurg.2017.12.021.
- Chapple C, Osman N. Faculty Opinions recommendation of Foreskin preputioplasty and intralesional triamcinolone: a valid alternative to circumcision for balanitis xerotica obliterans. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2012; 7 (4): 56–59. DOI: 10.3410/f.724694941.793513186.
- Green PA, Bethell GS, Wilkinson DJ, Kenny SE, Corbett HJ. Surgical management of genitourinary lichen sclerosus et atrophicus in boys in England: A 10-year review of practices and outcomes. J Pediatr Urol 2019; 15 (1): 45.e1–45.e5. DOI: 10.1016/j.jpurol.2018.02.027.
- Burstein B, Paquin R. Comparison of outcomes for pediatric paraphimosis reduction using topical anesthetic versus intravenous procedural sedation. Am J Emerg Med 2017; 35 (10): 1391–1395. DOI: 10.1016/j.ajem.2017.04.015.
- Pohlman GD, Phillips JM, Wilcox DT. Simple method of paraphimosis reduction revisited: Point of technique and review of the literature. J Pediatr Urol 2013; 9 (1): 104–107. DOI: 10.1016/j.jpurol.2012.06.012.
- Barberan Parraga C, Peng Y, Cen E, Dove D, Fassassi C, Davis A, et al.. Paraphimosis Pain Treatment with Nebulized Ketamine in the Emergency Department. J Emerg Med 2022; 62 (3): e57–e59. DOI: 10.1016/j.jemermed.2021.12.011.
- Little B, White M. Treatment options for paraphimosis. Int J Clin Pract 2005; 59 (5): 591–593. DOI: 10.1111/j.1742-1241.2004.00356.x.
- Anand A, Kapoor S. Mannitol for Paraphimosis Reduction. Urol Int 2013; 90 (1): 106–108. DOI: 10.1159/000343737.
- DeVries CR, Miller AK, Packer MG. Reduction of paraphimosis with hyaluronidase. Urology 1996; 48 (3): 464–465. DOI: 10.1016/s0090-4295(96)00198-7.
- Shalaby M, Cascio S. Megaprepuce: a systematic review of a rare condition with a controversial surgical management. Pediatr Surg Int 2021; 37 (6): 815–825. DOI: 10.1007/s00383-021-04883-5.
- Smeulders N, Wilcox DT, Cuckow PM. The buried penis - an anatomical approach. BJU Int 2000; 86 (4): 523–526. DOI: 10.1046/j.1464-410x.2000.00752.x.
- Ruiz E, Vagni R, Apostolo C, Moldes J, Rodríguez H, Ormaechea M, et al.. Simplified Surgical Approach to Congenital Megaprepuce: Fixing, Unfurling and Tailoring Revisited. J Urol 2011; 185 (6s): 2487–2490. DOI: 10.1016/j.juro.2011.01.015.
- Rod J, Desmonts A, Petit T, Ravasse P. Congenital megaprepuce: A 12-year experience (52 cases) of this specific form of buried penis. J Pediatr Urol 2013; 9 (6): 784–788. DOI: 10.1016/j.jpurol.2012.10.010.
Última actualización: 2025-09-21 13:35