
34: Otras anomalías del pene
Este capítulo durará aproximadamente 18 minutos para leer.
Introducción
Este capítulo tiene como objetivo analizar otras afecciones del pene que pueden encontrarse (aparte del hipospadias) y que potencialmente pueden requerir intervención o corrección quirúrgica. Estas incluyen curvatura peneana, torsión peneana, pene oculto y megaprepucio congénito.
La curvatura peniana y la torsión peniana pueden estar asociadas con hipospadias u otras afecciones urológicas; o pueden ser entidades aisladas. El término curvatura peniana congénita se ha utilizado de manera intercambiable como curvatura peniana sin hipospadias, uretra corta congénita y curvatura peniana congénita en la literatura. Snodgrass propuso que ‘curvatura peniana sin hipospadias’ fuese reemplazada por ‘curvatura peniana congénita’ y se hará referencia a ella como tal a lo largo de este capítulo.1 Existen distintos grados de curvatura peniana congénita. Esta puede ser ventral, dorsal y lateral o una combinación de las tres.
La torsión peneana es una rotación anormal del cuerpo del pene que ocurre con mayor frecuencia en sentido contrario a las agujas del reloj. También se ha informado que la curvatura peneana congénita y la torsión peneana ocurren simultáneamente.2
Existen presentaciones variadas del pene enterrado o del megaprepucio congénito. Estas entidades pueden variar en su espectro de presentación y se confunden con frecuencia con el micropene; sin embargo, el tamaño del pene suele ser normal. Uno de los motivos de consulta puede ser la dificultad miccional como resultado del acúmulo de orina en niños con megaprepucio congénito. Se han utilizado muchos términos y descriptores para referirse a la afección: oculto, encubierto, poco aparente, invisible, atrapado y pene enterrado, entre otros. Estos términos amplios y abarcadores se refieren a la apariencia del pene, pero pueden no definir la causa anatómica.3 Al igual que su nomenclatura, se han documentado múltiples abordajes para su corrección.
Embriología
Durante su crecimiento, los genitales externos se desarrollan rápidamente, lo que puede resultar en grandes variaciones morfológicas.4 Entre las semanas 4 y 7 de gestación, el tubérculo genital se forma por migración de mesénquima mesodérmico a la región craneal de la membrana cloacal. La región caudal de la membrana cloacal forma los pliegues urogenitales. La membrana cloacal es una estructura de doble capa, compuesta por endodermo y ectodermo. A partir de la semana 7 de gestación, ocurre la diferenciación de los genitales externos en el sexo masculino. Esto se completa para las 16–17 semanas de gestación. El gen SRY en el cromosoma Y induce el desarrollo de los cordones sexuales primitivos para formar los testículos. Las células de Leydig dentro de los testículos producen testosterona, que se convierte en dihidrotestosterona para promover el desarrollo de los genitales externos masculinos.5
En el varón, los andrógenos hacen que el mesodermo del tubérculo genital forme los cuerpos cavernosos y el glande del pene. La uretra peneana proximal es resultado de la tubularización del endodermo. Esto contrasta con la uretra peneana distal, que se forma como resultado de la recanalización.6 Durante la octava semana de gestación, el ectodermo da lugar a la piel del pene y al prepucio. Bellinger y Kaplan demostraron que la curvatura peneana es un estado normal del desarrollo, con resolución hacia la semana 16 de gestación,7,8
Curvatura congénita del pene
Historia
Nesbit describió por primera vez tres casos de curvatura congénita del pene en 1965. Sugirió que esta afección era secundaria a longitudes fasciales desproporcionadas que rodean los cuerpos cavernosos.9
La torsión peneana congénita fue descrita por primera vez por Verneuil en 1857. En ese momento, se desaconsejaba la intervención quirúrgica, ya que los intentos de movilizar la piel no lograban corregir la alineación en espiral de los cuerpos cavernosos. En 1947, Fevre describió una técnica para la reparación de la torsión peneana, en la que desinsertó los pilares del pubis y los reinsertó en una posición normal.10,11
Epidemiología
Los primeros estudios han señalado que la curvatura peneana congénita ocurre en el 4–10% de los varones.12,13 La incidencia de curvatura dorsal es baja en ausencia de hipospadias, con tasas de ~5% descritas.14
La incidencia de la torsión peneana congénita varía entre 1,5–27%.15,16 La torsión peneana significativa de más de 90 grados es menos frecuente, afectando al 0,7% de los varones recién nacidos.16
Patogénesis
En 1937, Young teorizó que la curvatura peneana era secundaria a una uretra congénitamente corta. Devine y Horton propusieron el desarrollo anómalo de la fascia periuretral como causa.17 Kramer propuso que la desproporción de los cuerpos cavernosos contribuía a la curvatura peneana.13 En su serie, Donnahoo señaló la curvatura peneana secundaria al anclaje de la piel y el dartos como la causa más común (65%), la desproporción de los cuerpos cavernosos (28%) y una uretra congénitamente acortada (7%). Este estudio registró tasas de curvatura ventral (84%), dorsal (11%) y lateral (5%).12 El estudio histopatológico de la placa uretral demostró la ausencia de fibrosis y displasia en muestras tomadas intraoperatoriamente.18 Esta evidencia, sin embargo, refuta la teoría de que las bandas fibrosas causan la curvatura peneana. También se ha propuesto como causa de la curvatura peneana persistente la detención del desarrollo peneano mientras el pene presenta una curva fisiológica.7
La curvatura dorsal adquirida puede ocurrir como resultado de la contracción cicatricial o de una cicatrización anómala tras una circuncisión.19
Se desconoce la etiología exacta de la torsión peneana congénita. Las teorías propuestas incluyen la inserción cutánea anómala, el desarrollo asimétrico de los cuerpos cavernosos y un defecto rotacional, ya sea de los cuerpos cavernosos o del glande.11,20
Evaluación y diagnóstico
En el varón con hipospadias, la presencia de curvatura peniana congénita y torsión se evalúa con frecuencia de forma intraoperatoria tras una prueba de erección artificial.
En los niños sin hipospadias, a menudo es la observación por parte de los padres lo que genera la preocupación por la curvatura peneana. Durante la adolescencia, la curvatura peneana se hace evidente tras erecciones espontáneas. Otra circunstancia que puede conducir a la detección de estas afecciones es su hallazgo incidental durante un examen médico de rutina. Puede sospecharse torsión peneana si el rafe peneano se desvía de la línea media. La presencia de estas afecciones, sin embargo, es menos evidente en niños con fimosis fisiológica. La evaluación en la consulta también puede verse limitada por la escasa colaboración del paciente y la constitución física.19 La evaluación intraoperatoria de la curvatura peneana se realiza mediante una prueba de erección artificial.
Devine y Horton propusieron una clasificación quirúrgica de la curvatura peneana congénita en tres categorías. Grupo I, secundario a deficiencia del cuerpo esponjoso, fascia de Dartos y fascia de Buck; Grupo II debido a deficiencia de la fascia de Dartos y de la fascia de Buck; y Grupo III involucraba únicamente la fascia de Dartos.17 Este sistema de clasificación se amplió para incluir el Grupo IV, que representaba una desproporción de los cuerpos cavernosos.13 Un sistema de clasificación quirúrgica adicional de Donnahoo et al describió tres tipos de curvatura peneana congénita; Tipo I es una curvatura secundaria a anclaje cutáneo (Figura 1) y (Figura 2) Tipo II se debe a córdea fascial, y Tipo III es resultado de desproporción de los cuerpos cavernosos.12

Figura 1 Curvatura tipo 1 con prepucio en capucha y meato apical.
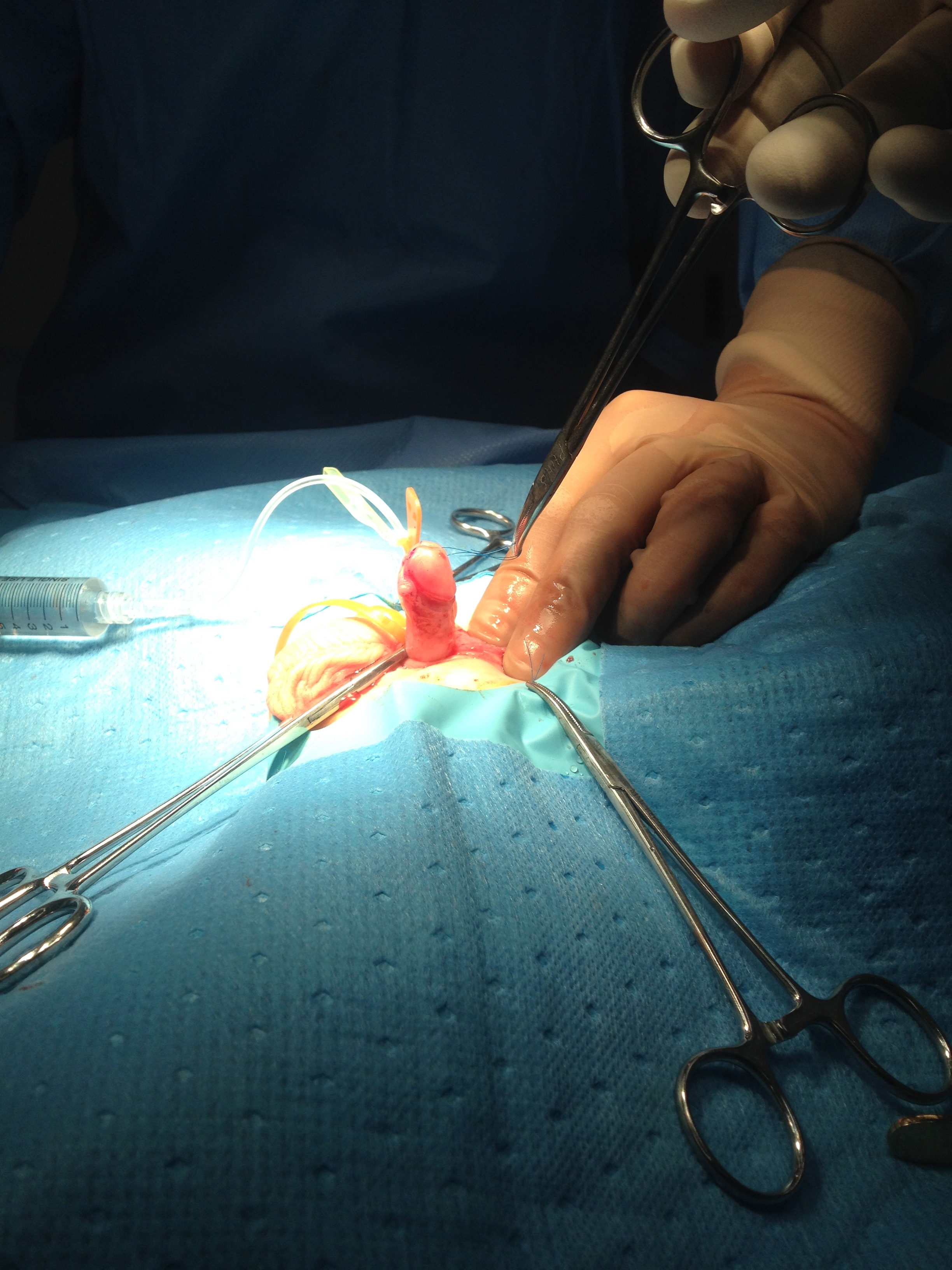
Figura 2 Prueba de erección después del despegamiento cutáneo mostrando la curvatura corregida.
Opciones de tratamiento
Si se diagnostica de forma precoz, la corrección quirúrgica de la curvatura peneana congénita debería idealmente realizarse durante el primer año de vida.21 Las opciones quirúrgicas para el manejo de la curvatura peneana dependen de la gravedad, preferiblemente intentando inicialmente la técnica menos invasiva.19 Una encuesta de urólogos pediátricos realizada por la AAP encontró que las curvaturas peneanas de hasta 10 grados con frecuencia se dejaban sin tratar. Una curvatura peneana de más de 20 a 30 grados requiere intervención, por lo tanto, esta gravedad se etiquetó como chordee significativa.22,23 La encuesta encontró que cualquier curvatura peneana menor de 50 grados a menudo se manejaba con plicatura dorsal, mientras que las curvaturas mayores de 50 grados comúnmente requerían un procedimiento de alargamiento ventral.22
En presencia de inclinación del glande, se recomienda como primer paso una liberación del frenillo. Se realiza un despegamiento circunferencial de la piel del pene hasta su base para corregir el anclaje cutáneo. Se realiza una prueba de erección artificial para evidenciar la persistencia de la curvatura peneana. Se sugiere la plicatura para la curvatura peneana residual de hasta 30 grados.1 La técnica de Nesbit fue uno de los primeros métodos para corregir la curvatura peneana. Esta consistía en la disección del paquete neurovascular dorsal separándolo de los cuerpos cavernosos, seguida de plicatura de la túnica albugínea para corregir la desproporción de longitud existente con el aspecto ventral. Posteriormente, tras observar recurrencias, esta técnica se modificó e incluyó la escisión de una cuña en forma de diamante en el sitio de máxima curvatura y la aposición transversal de los bordes de la túnica.9 Los estudios neuroanatómicos demostraron que las ramas nerviosas del pene se localizan a las 11 y a la 1 en punto y se distribuyen ventralmente.5 Por lo tanto, la plicatura en la línea media dorsal se realiza en la posición de las 12 en punto, evitando el paquete neurovascular. Esta área es también la región más gruesa y resistente de la túnica.21,24 La decisión de utilizar una sola sutura de plicatura o múltiples suturas de plicatura queda a criterio del cirujano.
Existen varias técnicas para manejar la curvatura peneana mayor de 30 grados, incluidas la transección de la placa uretral y la corporotomía ventral (con o sin injerto del defecto de los cuerpos cavernosos) y la uretroplastia por etapas.1,13 Esto proporciona un alargamiento ventral para abordar la desproporción de los cuerpos cavernosos. El injerto dérmico inicial fue descrito por Devine y Horton.17
Para evitar la transección de la placa uretral, Mollard y Castagnola propusieron la disección de la uretra de los cuerpos cavernosos subyacentes además de la plicatura dorsal.25 De manera similar, se realizó la disección de la uretra de los cuerpos cavernosos y se extendió hasta la uretra bulbar.26
La curvatura congénita del pene fue tratada por Donnahoo et al mediante movilización completa de la uretra con injerto dérmico ventral.12 Esto fue similar a la experiencia de Tang en hasta una cuarta parte de sus pacientes.23
Otras técnicas para manejar presentaciones complejas de curvatura peneana asociada con hipospadias o epispadias incluyen la disociación de los cuerpos cavernosos y el desmontaje peneano con injerto de submucosa de intestino delgado,27,28,29,30
La modificación de las técnicas Shaeer I y II anteriores consistió en la rotación de los cuerpos cavernosos con fijación mediante suturas sin corporotomía.31
La corrección de la torsión peneana se considera un procedimiento estético, ya que el pene permanece funcionalmente aceptable. Algunos autores han abogado por la reparación de la torsión peneana si el grado de torsión es superior a 45 grados. Existen múltiples opciones quirúrgicas para la corrección de la torsión peneana. Se ha propuesto un enfoque quirúrgico por etapas que incluye desenfundamiento peneano, colgajo de rotación amplio basado en el dartos, movilización de la placa uretral y del cuerpo esponjoso, movilización de la uretra proximal y movilización de la placa uretral/uretra hipoplásica con el cuerpo esponjoso hacia el glande.32,33 Un método adicional descrito es la sutura lateral de la túnica albugínea al periostio púbico.20 Algunos han descrito el desenfundamiento peneano y la refijación de la piel, sin embargo, estos resultados no siempre han sido exitosos.20
Complicaciones
Las complicaciones tras la corrección de la curvatura peneana varían del 5% hasta el 50% según la gravedad de la curvatura, con una tasa global del 8%, e incluyen dehiscencia del glande, fístula uretrocutánea, recurrencia de la curvatura y disfunción eréctil como las más frecuentes,23,12,34
Las complicaciones de la corrección de la torsión peneana incluyen hematoma, torsión peneana residual y disminución de la satisfacción de los padres o del paciente.35
Seguimiento sugerido y resultados
La revisión ambulatoria posoperatoria inicial puede variar de seis a doce semanas, según la preferencia del cirujano. Con respecto a la curvatura peneana, la evaluación se realiza mediante la observación por parte de los padres y/o del paciente de las erecciones naturales, además del examen físico en la consulta externa. Existen pocos estudios que se centran en la duración adecuada del seguimiento posoperatorio.23
Megaprepucio congénito
Historia
La primera descripción publicada del pene sepultado fue de Keyes en 1919, donde describió que la afección se debía a que el pene carecía de su ‘vaina cutánea’ adecuada y permanecía ‘sepultado por debajo del tegumento del abdomen, del muslo o del escroto’.36,37 Desde 1919, se han documentado varios informes de casos y debates sobre este tema, y sus primeros contribuyentes sentaron las bases para el mayor trabajo que se ha realizado en los últimos veinte a treinta años. Campbell, en 1951, describió “pene oculto” como “un órgano rudimentario oculto bajo la piel del escroto, periné, abdomen inferior o muslo, en los tejidos grasos que pueden ser inusualmente gruesos”, Glanz, en 1968, informó un caso en un adulto, Warkany, en 1971, describió un “micropene o pene oculto”. Williams, en 1974, lo describió e ilustró con un ejemplo. En 1977, además de describir sus seis casos, Crawford propuso la primera clasificación para el pene sepultado.38
Curiosamente, dos informes fundamentales tempranos incluyeron estudios radiológicos. En 1974, Gwinn y sus colegas describieron en su “caso radiológico del mes” a un niño de 18 meses a quien se le realizó una urografía intravenosa para la estadificación del linfoma de Hodgkin. Durante la fase miccional, observaron que “todo el contraste en su vejiga descendió hacia una llamativa distensión bulbosa del prepucio”.
Aunque no se menciona específicamente, su informe probablemente proporciona la primera descripción de un megaprepucio.39,40 Veinte años después, en 1994, O’Brien et al comunicaron un caso de un niño de once meses de edad en quien se observó una “gran tumefacción esferoidal, de aproximadamente el tamaño de una naranja” y cómo su madre “demostró cómo la tumefacción podía desinflarse fácilmente mediante compresión manual”. Durante la uretroscopia, no lograron encontrar el meato debido al prepucio redundante. Se colocó un catéter suprapúbico y se realizó una cistografía miccional. Además de demostrar una vejiga y uretra normales, se observó que el contraste fluía hacia una gran vejiga prepucial con una capacidad tan grande como la de su vejiga urinaria”. Acuñaron el término megaprepucio congénito para describir esto, lo que constituyó el primer uso documentado,40,41
Epidemiología
Se desconoce la incidencia exacta del pene inconspicuo. Sin embargo, se ha propuesto que se trata de una condición emergente.42 En una revisión reciente de la literatura, el número de casos osciló entre 1 y 134 pacientes, con edades de 2 meses a 33 años. En promedio, la cirugía se realizó antes de los 24 meses de edad.43
Patogénesis
El pene inconspicuo puede desarrollarse como resultado de múltiples factores en lugar de uno solo. Estos pueden incluir deficiencia de piel del pene, fijación anómala de la piel del cuerpo del pene en la base del pene, que la piel del pene esté anclada hacia adelante debido a un dartos disgenésico y una almohadilla grasa prepubiana prominente. Las causas secundarias resultan de complicaciones de la cicatrización cicatricial tras la circuncisión o de una hernia o hidrocele voluminosos.44
Se desconoce la etiología exacta del megaprepucio congénito, pero la teoría ampliamente propuesta es que resulta de los efectos de tracción del dartos anómalo sobre el eje del pene. Esto se sustenta en los enfoques iniciales para la corrección del pene enterrado, los cuales observaron que la corrección del defecto se lograba con éxito mediante la resección del tejido del dartos. Un estudio prospectivo que analizó la histología del dartos observó que casi el 80% de los pacientes presentaban tejido del dartos anómalo que tenía fibras de músculo liso poco desarrolladas o distribuidas al azar. Curiosamente, los pacientes con pene enterrado presentaban con mayor probabilidad un dartos anómalo en comparación con el grupo con hipospadias (78% frente a 70%).45 El aumento de la producción de volumen urinario tras el periodo neonatal y un chorro miccional anómalo debido a un orificio prepucial estrecho son los que contribuyen al efecto de balonización de la afección.46
Evaluación y diagnóstico
Es importante distinguir entre un pene de tamaño normal que está oculto frente a un micropene. Esta es la primera evaluación necesaria, ya que el enfoque de manejo es bastante diferente en ambos casos. El primero requeriría atención continua y, con mayor probabilidad, intervención quirúrgica con el urólogo, mientras que el segundo requeriría una evaluación adicional y atención conjunta con el equipo de Endocrinología y Genética. Este capítulo no abordará el manejo del micropene.
Crawford clasificó por primera vez el pene enterrado en oculto, enterrado y pterigio penoescrotal.38 Maizels et al describieron las diferentes etiologías como: enterrado, con pterigio, atrapado o micro/ diminuto. Esta clasificación ha sido la más utilizada, ya que abarca los grupos en los que el niño puede clasificarse según el examen clínico.47 Al describir su abordaje quirúrgico (V-plastia ventral) para la corrección del megaprepucio congénito, Alexander y colaboradores propusieron una clasificación con una descripción anatómica más precisa y la posible causa subyacente (Figura 3), (Figura 4), (Figura 5), (Figura 6), y (Figura 7)3
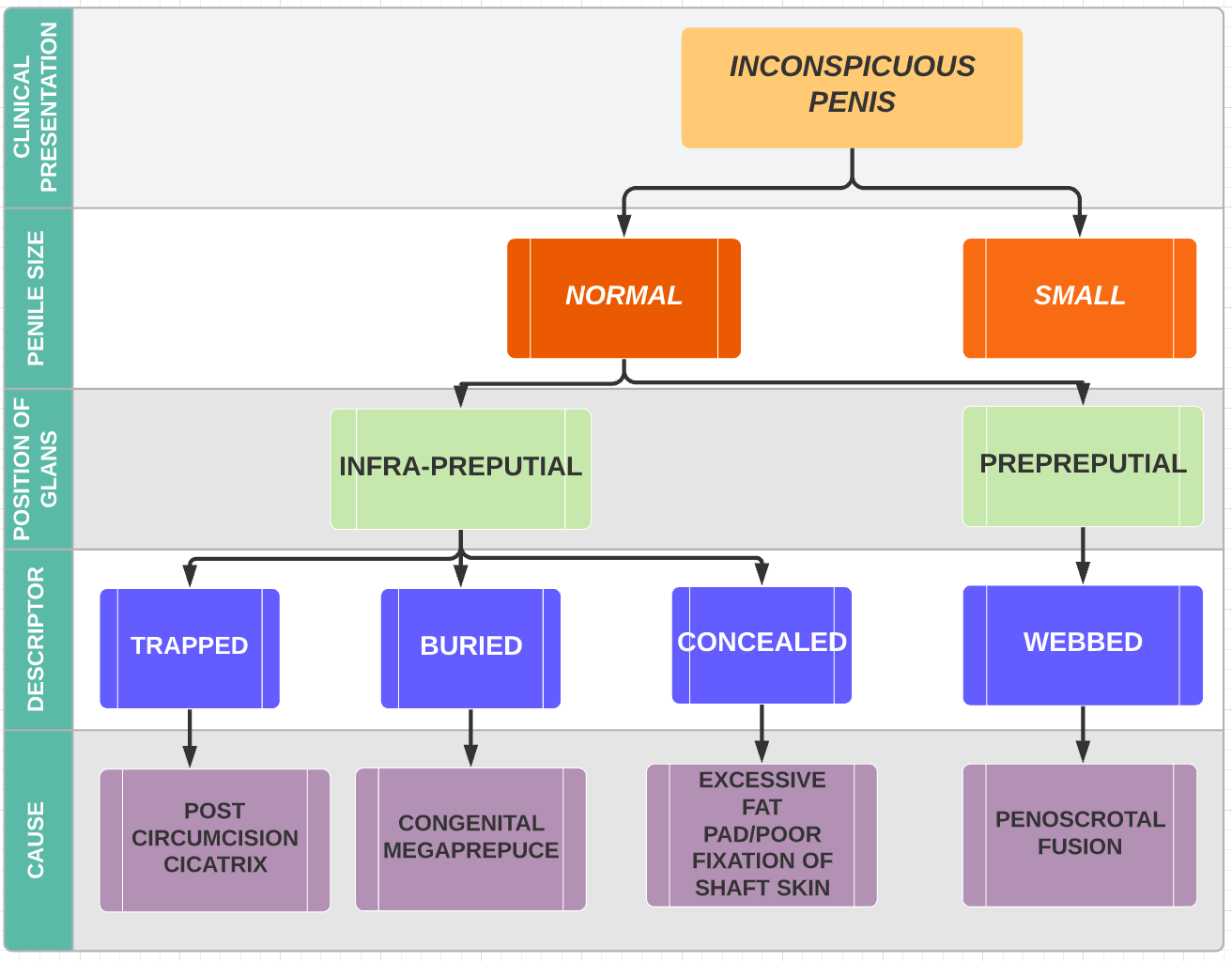
Figura 3 Clasificación de las causas de un pene poco aparente (Alexander et al).

Figura 4 Pene atrapado tras la circuncisión
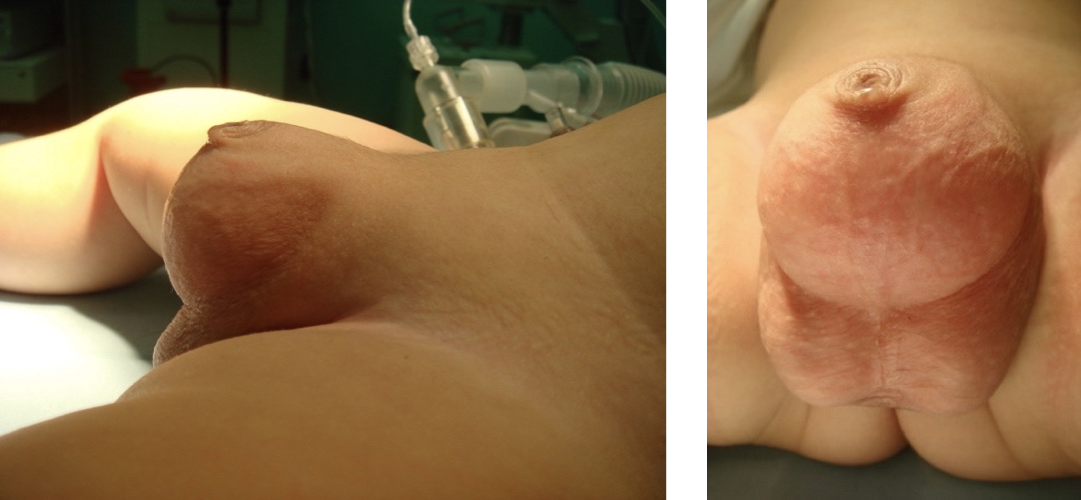
Figura 5 Megaprepucio congénito

Figura 6 Pene oculto

Figura 7 Fusión peneoescrotal
Hadidi propuso dividir a los pacientes con pene enterrado en tres grupos según sus hallazgos intraoperatorios. Grado 1 – pacientes con un prepucio interno anormalmente largo (LIP), Grado 2 – LIP y inserciones distales anómalas de los ligamentos fundiforme y suspensorio en el tercio medio del cuerpo del pene, Grado 3 – Grados 1 y 2 más exceso de grasa suprapúbica.37
Opciones de tratamiento
Se han descrito múltiples abordajes quirúrgicos para la exteriorización y corrección de este grupo de afecciones. El momento exacto de la cirugía ha sido un tema controvertido y está esencialmente influido por la causa subyacente. Los defensores de la intervención temprana aducen razones similares a las del momento de la reparación del hipospadias – la intervención temprana (6-12 meses de edad) es aconsejable para evitar consecuencias psicológicas.44,48 Quienes presentan síntomas (retención urinaria, balanitis recurrente, infecciones del tracto urinario) se beneficiarán de una cirugía más temprana. Otros autores recomiendan la corrección quirúrgica tan pronto como se realiza el diagnóstico para resolver tanto los aspectos urinarios como los estéticos,49,50 Por otro lado, la corrección de un pene oculto resultante de una almohadilla grasa prepubiana prominente puede diferirse, ya que puede mejorar espontáneamente con el tiempo, y Donahoe y Keating describieron que con las erecciones se observaba una cobertura cutánea adecuada del eje del pene.51
Existe un conjunto de publicaciones y técnicas que describen la corrección del megaprepucio congénito.3,42,43,46,52 Los pasos quirúrgicos principales se enumeran a continuación, con variaciones en cómo se realiza cada paso, lo que conduce a la diversidad de técnicas. Estas pueden clasificarse predominantemente en un enfoque de una sola etapa (la mayoría de las técnicas) o en uno de dos etapas. En este último, inicialmente se realiza una preputioplastia, con una reevaluación posterior de la anatomía después del entrenamiento para el control de esfínteres.
Los pasos quirúrgicos son:
- Resección del anillo estenótico o fimótico
- Despliegue del prepucio
- Resección o reducción del prepucio interno redundante
- Escisión del músculo dartos displásico
- Recreación del ángulo penopúbico y penoescrotal mediante la fijación de la dermis del cuerpo del pene a la fascia de Buck a las 4 y 8 en punto
- Cobertura del cuerpo del pene–la mayoría de las técnicas difieren en el tejido utilizado para cubrir el cuerpo del pene. Esto puede lograrse utilizando piel del pene, el prepucio interno redundante o una combinación de ambos.
Es nuestra preferencia utilizar el abordaje anatómico, ya que hemos tenido buenos resultados en nuestra experiencia (Figura 8),52,53
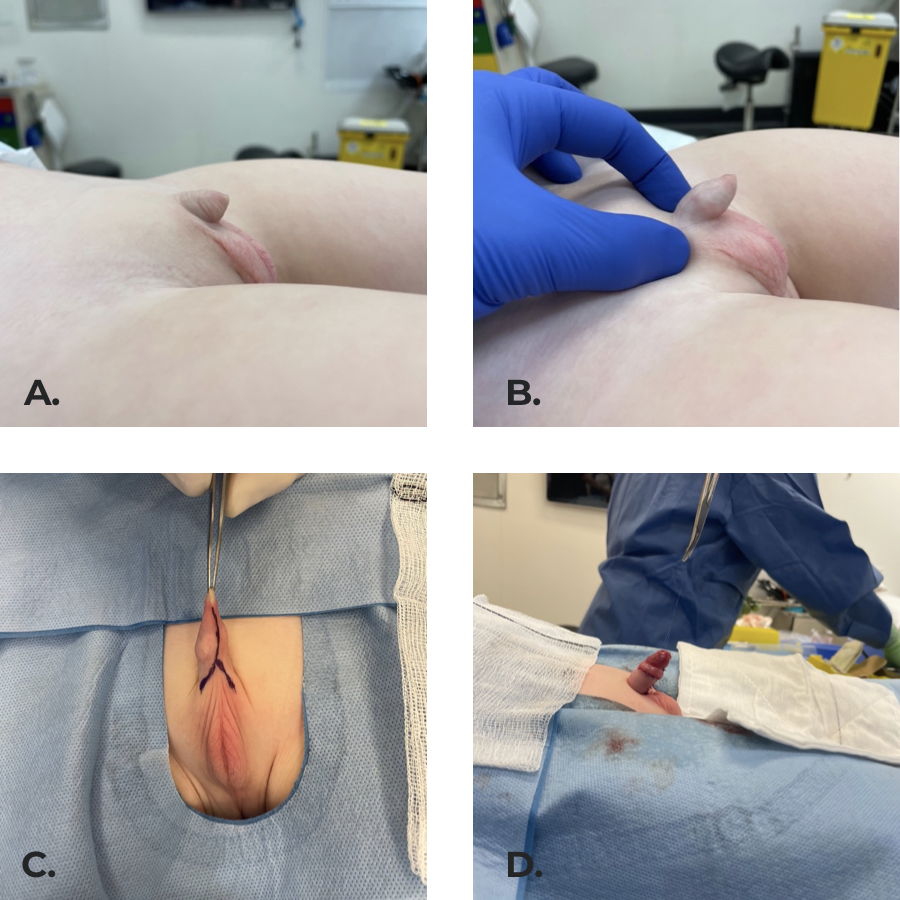 Figura 8 Pene poco aparente secundario a fusión penoescrotal y ángulo penopúbico poco definido. (b) pene expuesto en la exploración. (c) Incisiones quirúrgicas marcadas. (d) Resultado final con el cuerpo del pene cubierto por piel, con los ángulos púbico y escrotal creados fijando la dermis a la fascia de Buck a las 4 y a las 8 horas.
Figura 8 Pene poco aparente secundario a fusión penoescrotal y ángulo penopúbico poco definido. (b) pene expuesto en la exploración. (c) Incisiones quirúrgicas marcadas. (d) Resultado final con el cuerpo del pene cubierto por piel, con los ángulos púbico y escrotal creados fijando la dermis a la fascia de Buck a las 4 y a las 8 horas.
Complicaciones
Las complicaciones postoperatorias a corto plazo son hematoma, dehiscencia de la herida y edema peniano / escrotal. Las complicaciones a medio y largo plazo incluyen la necesidad de reintervención debido a linfedema que conduce a exceso de piel prepucial interna, estenosis meatal y retracción del pene,3,42,46,52,54
Seguimiento y resultados sugeridos
Dado que algunas de las complicaciones se han descrito en etapas posteriores de la vida, se recomienda un seguimiento a largo plazo para estos pacientes. Shalaby y Cascio informaron una mediana de seguimiento de 17 a 61 meses.40
Conclusiones
Las afecciones congénitas del pene son poco frecuentes; por lo tanto, se recomienda la derivación a un urólogo pediatra para un diagnóstico y manejo adecuados.
Puntos clave
- Se recomienda la corrección quirúrgica de la curvatura peneana congénita mayor de 20 grados
- Se prefiere un enfoque por etapas con protección de las estructuras neurovasculares y preservación de la placa uretral al reparar la curvatura peneana (sin hipospadias)
- Considere la corrección de la torsión peneana mayor de 45 grados
- La escisión del dartos displásico y la fijación cutánea a la fascia de Buck son pasos clave al corregir un megaprepucio congénito
- Limite la escisión cutánea hasta que se garantice una cobertura adecuada del eje peneano
- Se prefiere el manejo inicial no quirúrgico para el pene oculto
Lecturas recomendadas
- Mingin G, Baskin LS. Management of chordee in children and young adults. Urol Clin North Am 2002; 29 (2): 277–284, DOI: 10.1016/s0094-0143(02)00044-7.
- Smeulders N, Wilcox DT, Cuckow PM. The buried penis-an anatomical approach. BJU Int 2000; 86 (4): 523–526, DOI: 10.1046/j.1464-410x.2000.00752.x.
- Alexander A, Lorenzo AJ, Salle JLP, Rode H. The Ventral V-plasty: a simple procedure for the reconstruction of a congenital megaprepuce. J Pediatr Surg 2010; 45 (8): 1741–1747, DOI: 10.1016/j.jpedsurg.2010.03.033.
- Shalaby M, Cascio S. Megaprepuce: a systematic review of a rare condition with a controversial surgical management. Pediatr Surg Int 2021; 37 (6): 815–825, DOI: 10.1007/s00383-021-04883-5.
Referencias
- Snodgrass WT. Management of penile curvature in children. Curr Opin Urol 2008; 18 (4): 431–435, DOI: 10.1097/mou.0b013e32830056d0.
- Slawin KM, Nagler HM. Treatment of congenital penile curvature with penile torsion: a new twist. J Urol 1992; 147 (1): 152–154, DOI: 10.1016/s0022-5347(17)37169-0.
- Alexander A, Lorenzo AJ, Salle JLP, Rode H. The Ventral V-plasty: a simple procedure for the reconstruction of a congenital megaprepuce. J Pediatr Surg 2010; 45 (8): 1741–1747, DOI: 10.1016/j.jpedsurg.2010.03.033.
- Gredler ML. Evolution of external genitalia: insights from reptilian development. Sex Dev 2014; 8 (5): 311–326, DOI: 10.1159/000365771.
- Yiee JH, Baskin LS. Penile embryology and anatomy. ScientificWorldJournal 2010; 10: 1174–1179, DOI: 10.1100/tsw.2010.112.
- Baskin L. Development of the human penis and clitoris. Differentiation 2018; 103: 74–85, DOI: 10.1016/j.diff.2018.08.001.
- Kaplan GW, Lamm DL. Embryogenesis of chordee. J Urol 1975; 114 (5): 769–772, DOI: 10.1016/s0022-5347(17)67140-4.
- Bellinger MF. Embryology of the Male External Genitalia. Urologic Clinics of North America 1981; 8 (3): 375–382, DOI: 10.1016/s0094-0143(21)01293-3.
- Nesbit RM. CONGENITAL CURVATURE OF THE PHALLUS: REPORT OF THREE CASES WITH DESCRIPTION OF CORRECTIVE OPERATION. J Urol 1965; 93: 230–232, DOI: 10.1016/s0022-5347(17)63751-0.
- Fevre. Treatment of bends and twists of the penis. Sem Hop 1947; 23 (14): 895,.
- Azmy A, Eckstein HB. Surgical correction of torsion of the penis. Br J Urol 1981; 53 (4): 378–379, DOI: 10.1111/j.1464-410x.1981.tb03202.x.
- Donnahoo KK. Etiology, management and surgical complications of congenital chordee without hypospadias. J Urol 1998; 160 (3 Pt 2): 1120–1122, DOI: 10.1016/s0022-5347(01)62713-7.
- Kramer SA, Aydin G, Kelalis PP. Chordee without hypospadias in children. J Urol 1982; 128 (3): 559–561, DOI: 10.1016/s0022-3468(83)80141-9.
- Kelâmi A. Classification of Congenital and Acquired Penile Deviation. Urologia Internationalis 1983; 38 (4): 229–233, DOI: 10.1159/000280897.
- Sarkis PE, Sadasivam M. Incidence and predictive factors of isolated neonatal penile glanular torsion. J Pediatr Urol 2007; 3 (6): 495–499, DOI: 10.1016/j.jpurol.2007.03.002.
- Ben-Ari J, Merlob P, Mimouni F, Reisner SH. Characteristics of the male genitalia in the newborn: penis. J Urol 1985; 134 (3): 521–522, DOI: 10.1016/s0022-5347(17)47272-7.
- Devine CJ Jr, Horton CE. Chordee without hypospadias. J Urol 1973; 110 (2): 264–271, DOI: 10.1016/s0022-5347(17)60183-6.
- Snodgrass W, Patterson K, Plaire JC, Grady R, Mitchell ME. Histology of the urethral plate: implications for hypospadias repair. J Urol 2000; 164 (3 Pt 2): 988–989 989–990, DOI: 10.1097/00005392-200009020-00017.
- Montag S, Palmer LS. Abnormalities of penile curvature: chordee and penile torsion. ScientificWorldJournal 2011; 11: 1470–1478, DOI: 10.1100/tsw.2011.136.
- Zhou L, Mei H, Hwang AH, Xie H-W, Hardy BE. Penile torsion repair by suturing tunica albuginea to the pubic periosteum. J Pediatr Surg 2006; 41 (1): 7–9, DOI: 10.1016/j.jpedsurg.2005.10.065.
- Mingin G, Baskin LS. Management of chordee in children and young adults. Urol Clin North Am 2002; 29 (2): 277–284, DOI: 10.1016/s0094-0143(02)00044-7.
- Bologna RA, Noah TA, Nasrallah PF, McMahon DR. Chordee: varied opinions and treatments as documented in a survey of the American Academy of Pediatrics, Section of Urology. Urology 1999; 53 (3): 608–612, DOI: 10.1016/s0090-4295(98)00656-6.
- Tang Y-M, Chen S-J, Huang L-G, Wang M-H. Chordee without hypospadias: report of 79 Chinese prepubertal patients. J Androl 2007; 28 (4): 630–633, DOI: 10.2164/jandrol.106.002436.
- Baskin LS, Erol A, Li YW, Cunha GR. Anatomical studies of hypospadias. J Urol 1998; 160 (3 Pt 2): 1108–1115. DOI: 10.1016/s0022-5347(01)62711-3.
- Mollard P, Castagnola C. Hypospadias: the release of chordee without dividing the urethral plate and onlay island flap (92 cases. J Urol 1994; 152 (4): 1238–1240, DOI: 10.1016/s0022-5347(17)32557-0.
- Bhat A. Extended urethral mobilization in incised plate urethroplasty for severe hypospadias: a variation in technique to improve chordee correction. J Urol 2007; 178 (3 Pt 1): 1031–1035, DOI: 10.1016/j.juro.2007.05.074.
- Koff SA, Eakins M. The treatment of penile chordee using corporeal rotation. J Urol 1984; 131 (5): 931–932, DOI: 10.1016/s0022-5347(17)50716-8.
- Perovic SV, Djordjevic ML. A new approach in hypospadias repair. World J Urol 1998; 16 (3): 195–199, DOI: 10.1007/s003450050052.
- Ballesteros N. Use of small intestinal submucosa for corporal body grafting in cases of epispadias and epispadias/exstrophy complex. J Pediatr Urol 2019; 15 (4): 406 1–406 6, DOI: 10.1016/j.jpurol.2019.05.024.
- Castellan M, Gosalbez R, Devendra J, Bar-Yosef Y, Labbie A. Ventral corporal body grafting for correcting severe penile curvature associated with single or two-stage hypospadias repair. J Pediatr Urol 2011; 7 (3): 289–293, DOI: 10.1016/j.jpurol.2011.03.008.
- Shaeer O, Shaeer K. Shaeer’s Corporal Rotation III: Shortening-Free Correction of Congenital Penile Curvature-The Noncorporotomy Technique. Eur Urol 2016; 69 (1): 129–134, DOI: 10.1016/j.eururo.2015.08.004.
- Bhat A, Bhat MP, Saxena G. Correction of penile torsion by mobilization of urethral plate and urethra. J Pediatr Urol 2009; 5 (6): 451–457, DOI: 10.1016/j.jpurol.2009.05.013.
- Fisher PC, Park JM. Penile torsion repair using dorsal dartos flap rotation. J Urol 2004; 171 (5): 1903–1904, DOI: 10.1097/01.ju.0000120148.79867.5c.
- Badawy H, Morsi H. Long-term followup of dermal grafts for repair of severe penile curvature. J Urol 2008; 180 (4 Suppl): 1842–1845, DOI: 10.1016/j.juro.2008.04.082.
- Bar-Yosef Y, Binyamini J, Matzkin H, Ben-Chaim J. Degloving and realignment-simple repair of isolated penile torsion. Urology 2007; 69 (2): 369–371, DOI: 10.1016/j.urology.2007.01.014.
- Keyes EL, Others. Phimosis, paraphimosis, tumors of the penis. Urology 1919; 67: 649,.
- Hadidi AT. Buried penis: classification surgical approach. J Pediatr Surg 2014; 49 (2): 374–379, DOI: 10.1016/j.jpedsurg.2013.09.066.
- Crawford BS. Buried penis. Br J Plast Surg 1977; 30 (1): 96–99, DOI: 10.1016/s0007-1226(77)90046-7.
- Gwinn JL, Lee FA, Haber K. Radiological case of the month. Unusual presentation of phimosis. Am J Dis Child 1974; 128 (6): 835–836,.
- Shalaby M, Cascio S. Megaprepuce: a systematic review of a rare condition with a controversial surgical management. Pediatr Surg Int 2021; 37 (6): 815–825, DOI: 10.1007/s00383-021-04883-5.
- O’Brien A, Shapiro AM, Frank JD. Phimosis or congenital megaprepuce? Br J Urol 1994; 73 (6): 719–720, DOI: 10.1111/j.1464-410x.1995.tb07856.x.
- Summerton DJ, McNally J, Denny AJ, Malone PS. Congenital megaprepuce: an emerging condition-how to recognize and treat it. BJU Int 2000; 86 (4): 519–522, DOI: 10.1111/j.1464-410x.2001.0003c.x.
- Werner Z, Hajiran A, Al-Omar O. Congenital Megaprepuce: Literature Review and Surgical Correction. .
- Park NC, Kim SW, Moon DG. Penile Augmentation. Berlin, Heidelberg: Springer; 2016, DOI: 10.1007/978-3-662-46753-4.
- Spinoit A-F, Praet C, Groen L-A, Laecke E, Praet M, Hoebeke P. Congenital penile pathology is associated with abnormal development of the dartos muscle: a prospective study of primary penile surgery at a tertiary referral center. J Urol 2015; 193 (5): 1620–1624, DOI: 10.1016/j.juro.2014.10.090.
- Ruiz E. Simplified surgical approach to congenital megaprepuce: fixing, unfurling and tailoring revisited. J Urol 2011; 185 (6 Suppl): 2487–2490, DOI: 10.1016/j.juro.2011.01.015.
- Maizels M, Zaontz M, Donovan J, Bushnick PN, Firlit CF. Surgical correction of the buried penis: description of a classification system and a technique to correct the disorder. J Urol 1986; 136 (1 Pt 2): 268–271, DOI: 10.1016/s0022-5347(17)44837-3.
- Shapiro SR. Surgical treatment of the ’buried’ penis. Urology 1987; 30 (6): 554–559, DOI: 10.1016/0090-4295(87)90435-3.
- Ferro F, Spagnoli A, Spyridakis I, Atzori P, Martini L, Borsellino A. Surgical approach to the congenital megaprepuce. J Plast Reconstr Aesthet Surg 2006; 59 (12): 1453–1457, DOI: 10.1016/j.bjps.2005.12.033.
- Philip I, Nicholas JL. Congenital giant prepucial sac: case reports. J Pediatr Surg 1999; 34 (3): 507–508, DOI: 10.1016/s0022-3468(99)90515-8.
- Donahoe PK, Keating MA. Preputial unfurling to correct the buried penis. J Pediatr Surg 1986; 21 (12): 1055–1057, DOI: 10.1016/0022-3468(86)90007-2.
- Betancor CEL, Cherian A, Smeulders N, Mushtaq I, Cuckow P. Mid- to long-term outcomes of the ’anatomical approach’ to congenital megaprepuce repair. J Pediatr Urol 2019; 15 (3): 243 1–243 6, DOI: 10.1016/j.jpurol.2019.02.007.
- Hirsch K, Schwaiger B, Kraske S, Wullich B. Megaprepuce: presentation of a modified surgical technique with excellent cosmetic and functional results. J Pediatr Urol 2019; 15 (4): 401 1–401 6, DOI: 10.1016/j.jpurol.2019.05.018.
- Rod J, Desmonts A, Petit T, Ravasse P. Congenital megaprepuce: a 12-year experience (52 cases) of this specific form of buried penis. J Pediatr Urol 2013; 9 (6 Pt A): 784–788, DOI: 10.1016/j.jpurol.2012.10.010.
- Callewaert PRH, Rahnama’i MS, Guimarães MNC, Vrijens DMJ, Kerrebroeck PEVA. DOuble LOngitudinal Megapreputium Incision TEchnique: the DOLOMITE. Urology 2014; 83 (5): 1149–1154, DOI: 10.1016/j.urology.2013.12.014.
- Lin H-W. An arc incision surgical approach in congenital megaprepuce. Chin Med J 2015; 128 (4): 555–557, DOI: 10.4103/0366-6999.151117.
- Smeulders N, Wilcox DT, Cuckow PM. The buried penis-an anatomical approach. BJU Int 2000; 86 (4): 523–526, DOI: 10.1046/j.1464-410x.2000.00752.x.
Última actualización: 2025-09-21 13:35