
26: Estenosis uretral congénita y traumática
Este capítulo durará aproximadamente 14 minutos para leer.
Introducción
Inicialmente se consideraba que las estenosis uretrales eran poco frecuentes en los niños.1 Informes posteriores sugirieron que no son tan raras.2 La impresión de una baja incidencia se debía principalmente al subregistro y a la escasez de literatura. Johanson fue el primero en observar la formación de estenosis en 1953 tras una disrupción uretral completa.1 Las estenosis uretrales se clasifican de forma general según su etiología en congénitas/idiopáticas, iatrogénicas, inflamatorias y traumáticas. No está claro si las estenosis sin una causa definida deben clasificarse como congénitas o como idiopáticas.
Harshman et al y Kaplan & Brock recomendaron evitar la designación de estenosis uretral congénita y describieron tales lesiones como estenosis de etiología desconocida.3,4 No está claro si las estenosis inducidas por catéter pueden clasificarse como iatrogénicas o inflamatorias. Dado que tal estenosis no habría ocurrido en primer lugar sin un catéter permanente, puede argumentarse que debería clasificarse como iatrogénica.2 Las causas iatrogénicas como la cateterización o la estenosis posterior a la reparación de hipospadias representan la mayoría de los casos de estenosis uretral anterior en la población pediátrica, especialmente en los grupos de menor edad. Sin embargo, a medida que el niño crece, se observa una preponderancia gradual de las estenosis uretrales traumáticas, incluidas las estenosis uretrales posteriores.
Estenosis congénitas e idiopáticas
Mori et al informaron que la estenosis/estrechez uretral congénita era una causa importante de infecciones del tracto urinario recurrentes, enuresis, polaquiuria o hematuria en niños.5 Se reconoce por un patrón de llenado lineal recto típico (Figura 1) También denominada Cobb’s collar o Moorman’s ring o membrana uretral posterior obstructiva congénita (COPUM), su etiología es desconocida. Se debate si esta entidad podría considerarse una estenosis.

Figura 1 Cistouretrografía miccional que muestra estenosis/ estrechez uretral idiopática/ congénita. Se observa un estrechamiento en anillo en la unión de la uretra anterior y posterior. A menudo las vías urinarias superiores no están dilatadas y se presentan con ITU o goteo
Esta lesión se observa como una estenosis en forma de anillo en la cistoscopia (Figura 2) justo distal al esfínter uretral externo.6 Por lo general, están ausentes características como la irregularidad vesical, el engrosamiento o los cambios del tracto urinario superior que se ven en las válvulas uretrales posteriores (PUV). El tratamiento más eficaz de esta lesión es la uretrotomía interna óptica (UIO) bajo visión directa. Esto se realiza en la posición de las 12 en punto utilizando un bisturí frío (flecha de (Figura 2) En niños con incontinencia urinaria diurna y una estenosis uretral bulbar congénita, los episodios de incontinencia mejoraron en 69.4% después de la UIO.5 Además, las infecciones del tracto urinario y el reflujo vesicoureteral se redujeron con el tratamiento precoz de esta patología.
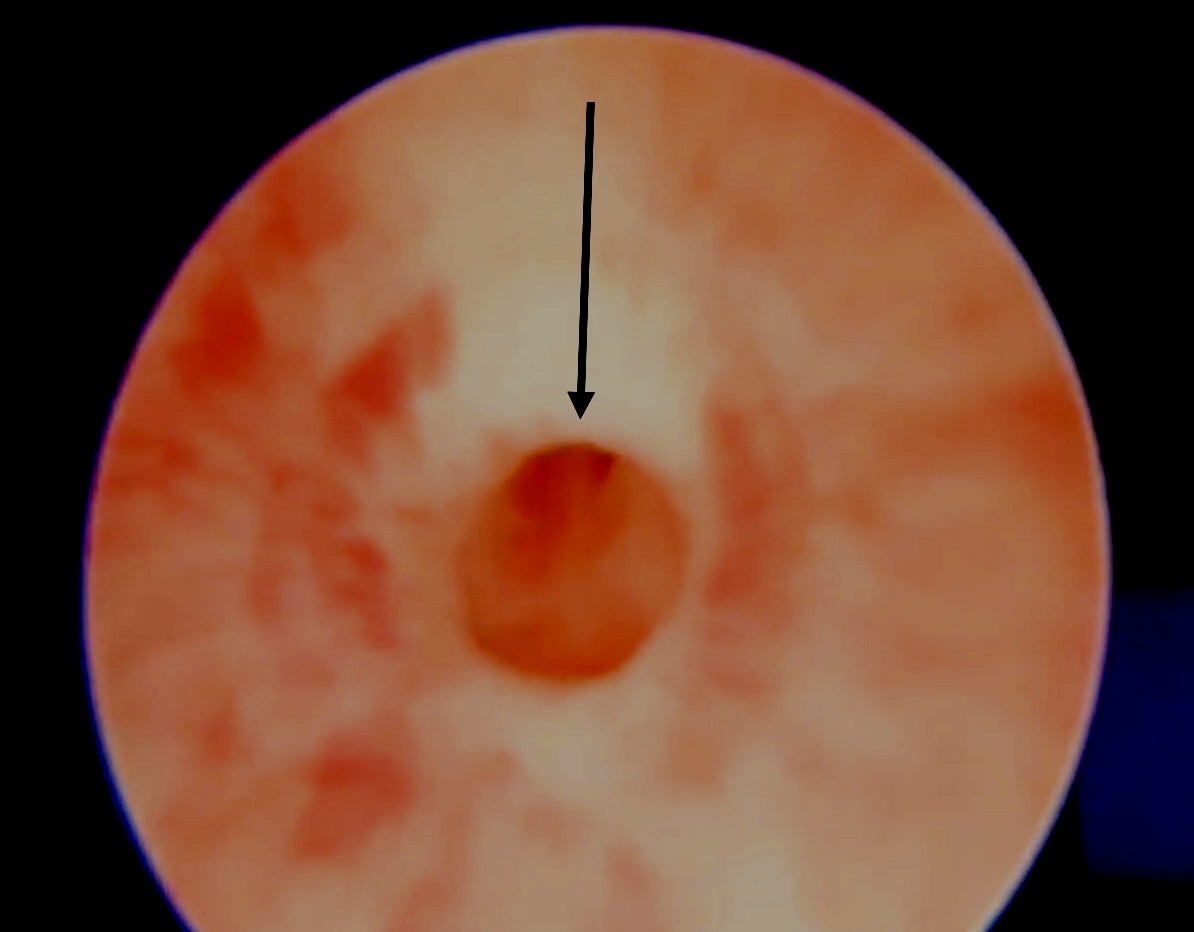
Figura 2 La uretrotomía interna óptica (OIU) para estrechamiento idiopático/congénito implica una incisión con bisturí frío a las 12 horas
Estenosis iatrogénicas
Estenosis inducidas por catéter
La cateterización uretral es una importante causa iatrogénica (12,3% del total), y es la principal causa de estenosis uretral anterior multifocal y panuretral en un estudio de Ansari et al.2 Las estenosis iatrogénicas debidas a cateterización prolongada (a menudo colocada para monitorización del gasto urinario en UCIs neurológicas) se localizan con frecuencia en la región bulbomembranosa. Si bien algunas pueden deberse a sondas de calibre excesivo, otras pueden ser por inflación del balón en la uretra o por retirada traumática del catéter (a menudo se observa sangrado uretral en tal situación). La cateterización prolongada por sí sola causa inflamación uretral, isquemia y, en última instancia, estenosis uretral. A menudo se presentan con retención urinaria tras la retirada del catéter. En tal situación, el autor prefiere realizar la colocación de un catéter suprapúbico (SPC) bajo guía ecográfica. Esto ayuda en futuras pruebas de micción mediante el pinzado del SPC. Además, el SPC puede utilizarse para un cistouretrograma miccional (VCUG) a fin de valorar la extensión de la estenosis. Con frecuencia, estas estenosis son estrechamientos de segmento corto susceptibles de OIU bajo anestesia general. Tras la OIU, se necesitan repetir el VCUG y realizar una prueba de micción para asegurar la resolución de la estenosis. Indicaciones claras y bien definidas para la cateterización, inserción hábil del catéter uretral, y considerar el SPC cuando es probable una cateterización prolongada deberían disminuir la incidencia de estas estenosis iatrogénicas.
Estenosis posteriores a la válvula uretral posterior
La fulguración transuretral de las válvulas es otra causa importante de estenosis uretral pediátrica. Aunque faltan datos específicos sobre la contribución de la fulguración de las válvulas a las estenosis en pediatría, la incidencia varía del 0% al 25% en diversas series.7 En una serie más reciente, 11 de 62 pacientes (5.6% del total) presentaron una estenosis iatrogénica después de la fulguración de las válvulas.2 Si bien se han propuesto diversas causas en el desarrollo de estas estenosis, la más importante es la inserción traumática de un resectoscopio sobredimensionado en una luz uretral estrecha y la fuga de corriente monopolar por aislamiento insuficiente del resectoscopio o por uso excesivo del cauterio. Se considera que esta es una causa evitable de estenosis en los niños, que puede prevenirse mediante delicadeza en la técnica quirúrgica, utilizando instrumental pequeño del tamaño adecuado para la fulguración en una uretra infantil estrecha, disminuyendo el tiempo de contacto durante la fulguración para evitar cortes profundos y realizando la fulguración bajo visión directa solo en el área de las válvulas.8 Los autores prefieren utilizar la ablación con cuchillo frío en lugar de la fulguración por diatermia para la ablación de VUP a fin de prevenir la lesión térmica y reducir la formación de estenosis.9 A menudo, las estenosis tras la ablación de las válvulas son estenosis de segmento corto, tratables mediante UIO. Esto debe realizarse con cuidado, con la inserción previa de una guía.
Estenosis en hipospadias
Las estenosis tras la reparación de hipospadias representan una buena proporción de las estenosis uretrales anteriores en adolescentes y adultos jóvenes. Pueden presentarse de forma temprana con chorro débil y goteo o tardíamente con infecciones del tracto urinario recurrentes (ITU) y cambios en el tracto urinario superior. Su presentación es muy variable y pueden diagnosticarse tarde, especialmente en la adultez temprana después de una reparación supuestamente ‘exitosa’ en la infancia sin fístulas. Ansari enfatizó la necesidad de advertir a los padres que los niños sometidos a reparación de hipospadias podrían desarrollar estenosis en el futuro y deberían ser vigilados durante la adolescencia para la formación de estenosis.2 A menudo la uroflujometría muestra una curva plana con un gran residuo posmiccional. Las estenosis por hipospadias tras la reparación uretral distal (placa incisa tubularizada- TIP) suelen ser estenosis de segmento largo debido a un lumen uretral deficiente. Estas se presentan precozmente con esfuerzo miccional y goteo. A menudo necesitan dejarse abiertas en placa hasta alcanzar una uretra de calibre normal. Pueden requerir injerto de piel prepucial local/ injerto de mucosa oral (OMG) o injerto de mucosa bucal (BMG) como inlay mientras se mantiene abierta en placa. Después de un periodo de 6 meses, estas pueden tubularizarse para proporcionar una uretra de mayor calibre. La estenosis por hipospadias tras la reparación de la uretra proximal (después de una reparación tubularizada en un solo tiempo – Duckett) a menudo se debe a un estrechamiento en la unión de la uretra nativa y la neouretra revestida de piel. Se necesita una uretrografía ascendente (AUG) para demostrar la localización exacta y la extensión del estrechamiento (Figura 3) Si se encuentra una estenosis anular estrecha en la unión de la neouretra con la uretra nativa, una OIU sola puede ser suficiente. Por otro lado, una estenosis densa de segmento largo puede requerir una reparación por etapas con OMG/BMG.10 (Figura 4) representa un diagrama de flujo en el manejo de las estenosis uretrales anteriores por hipospadias (HAUS). Se reseca todo el segmento estrecho cicatricial y el OMG se fija con puntos de acolchado en su lugar. Tras un periodo de 6 meses a 1 año, se realiza la tubularización. Barbagli informó que la longitud de la estenosis, pero no el número de operaciones previas necesarias para la reparación primaria del hipospadias, estaba asociada con el riesgo de fracaso.11 Algunos cirujanos prefieren una reparación en un solo tiempo con inlay dorsal de OMG para estas situaciones, mientras que el autor prefiere un abordaje en dos tiempos.12,13
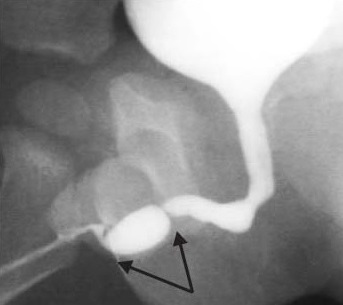
Figura 3 Estenosis uretral anterior tras la reparación de hipospadias, a menudo observada en la unión entre la uretra nativa y la neouretra. Los estrechamientos múltiples con aspecto de pliegues son tratables con OIU, mientras que las estenosis uretrales anteriores largas requieren injerto de mucosa oral con reparación en dos tiempos.

Figura 4 Un diagrama de flujo para el manejo de las estenosis uretrales anteriores asociadas al hipospadias (HAUS).
Estenosis inflamatorias
A diferencia de las series en adultos, las estenosis debidas a liquen escleroso (LS) o a causas infecciosas son poco frecuentes en niños.14 Aunque a menudo se considera que el LS es una enfermedad de la edad adulta, la balanitis xerótica obliterante (BXO), similar al LS, es una causa importante de estenosis uretrales, especialmente en niños mayores. Informes recientes muestran que no son tan infrecuentes como se pensaba antes.15 Estas estenosis son más difíciles de tratar y requieren múltiples intervenciones, ya que representan un proceso inflamatorio crónico y tienden a recurrir.2 Los urólogos pediátricos que operan estas estenosis deben explicar a los cuidadores la naturaleza de la afección y la necesidad de un seguimiento prolongado para identificar recurrencias.
Uretroplastia de sustitución con injerto de mucosa bucal y oral
Las estenosis uretrales anteriores que no son susceptibles de una anastomosis término-terminal requieren uretroplastia de sustitución. Esto puede lograrse mediante el uso de colgajos de piel peneana o injertos libres de piel de espesor total, mucosa oral vesical (OMG) o mucosa bucal (BMG). La uretroplastia de sustitución con OMG/ BMG está emergiendo rápidamente como la técnica más preferible para las estenosis panuretrales que involucran la uretra distal.16 En quienes presentan estenosis de la uretra pendulosa se utiliza una incisión circuncoronal, mientras que para estenosis más proximales se utiliza una incisión perineal en la línea media. Luego, el cuerpo esponjoso se separa dorsalmente de los cuerpos cavernosos y se realiza una uretrotomía en la posición de las 12 en punto. En pacientes con estenosis inflamatorias o traumáticas este abordaje es más sencillo, mientras que en aquellos con estenosis por hipospadias el esponjoso suele estar cicatrizado/ausente, lo que hace factible únicamente una apertura ventral tipo onlay a las 6 en punto. En tales casos, un procedimiento en dos etapas implica la exéresis completa del tejido fibrótico y el acolchado de BMG en la primera etapa. La uretra se reconstruye en la segunda etapa, 4–6 meses después de la primera.
En una reparación en un solo tiempo con onlay dorsal, para estenosis inflamatorias o traumáticas, el BMG/OMG se fija a los cuerpos cavernosos con suturas de poliglactina 6–0 en puntos separados y, posteriormente, se sutura a los bordes seccionados de la uretra con suturas continuas. Barbagli et al han descrito los pasos operatorios detallados (Figura 5)17 Para la reconstrucción del meato, el BMG más distal se fija con suturas de poliglactina 5–0 en puntos separados a los márgenes del meato seccionados dorsalmente. El paciente es dado de alta 3–5 días después de la cirugía con un catéter uretral a permanencia y un catéter suprapúbico. Los catéteres se retiran 3 semanas después, tras una cistouretrografía miccional. Si bien algunos autores favorecen la técnica de onlay dorsal, otros han informado resultados excelentes a largo plazo con técnicas de onlay ventral,5,18,19
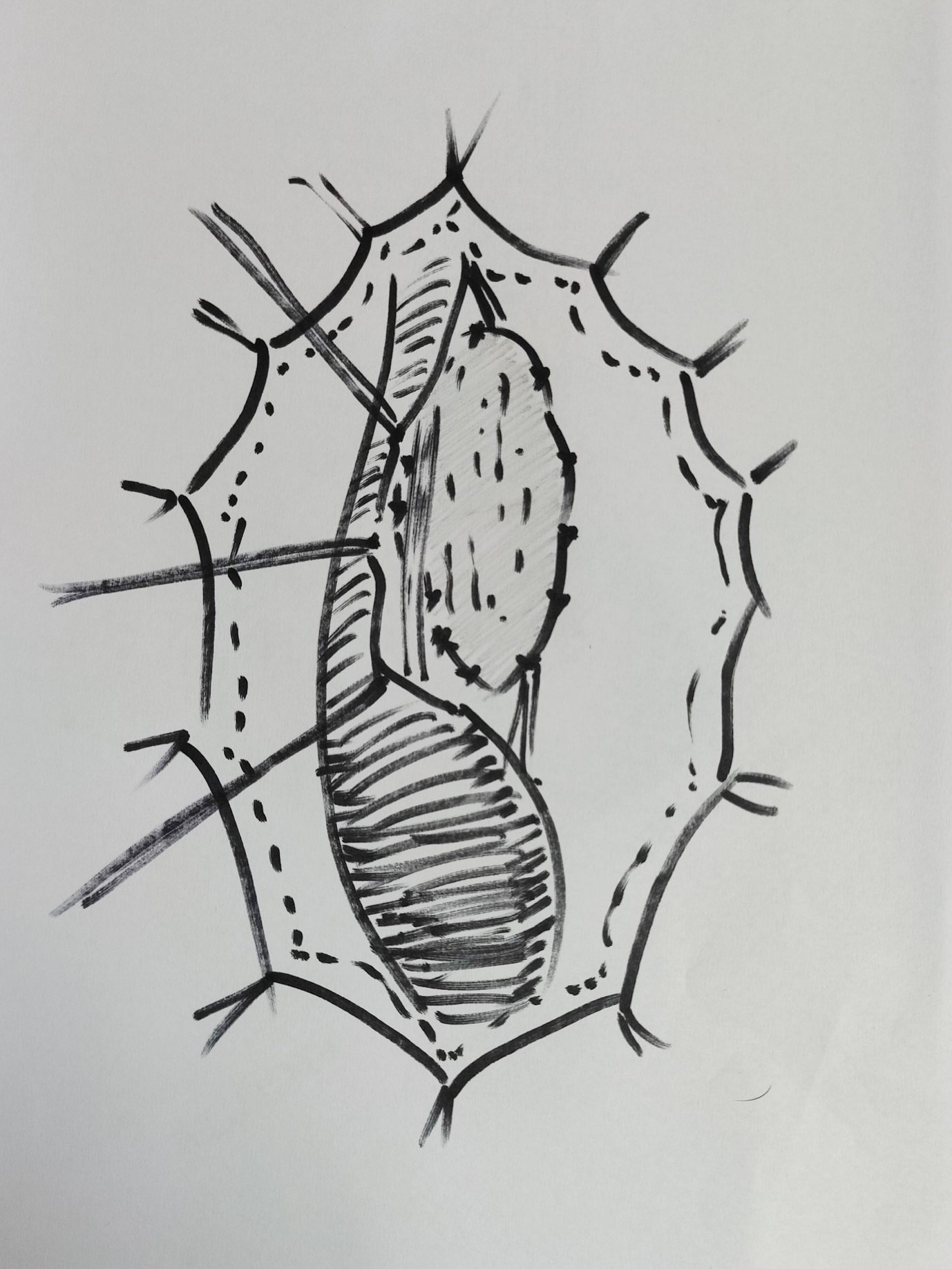
Figura 5 Uretroplastia de sustitución con onlay dorsal de BMG; la uretra ha sido movilizada; abierta en la posición de las 12 en punto dorsalmente; BMG fijado con puntos de acolchado en el dorso y se está anastomosando a los bordes.
Estenosis traumáticas
La etiología traumática adquiere mayor relevancia como causa de la enfermedad por estenosis uretral con el avance de la edad. En una serie de Ansari, el 36,9% del total de las estenosis se debieron a etiología traumática.2 Si bien el 18% de las estenosis en niños menores de 10 años fueron secundarias a traumatismo, el 45% de las estenosis en pacientes mayores de 10 años fueron de origen traumático. La fractura pélvica, una causa importante de estenosis uretral en adolescentes, suele deberse a una caída desde altura, a accidentes de tráfico o a traumatismo perineal por lesión en horcajadas.
Turner Warwick introdujo el término “complejo” defecto de distracción uretral posterior por fractura pélvica (PFPUDD) cuando están presentes una o más de las siguientes características: (a) el defecto de distracción es largo (≥3 cm) y está rodeado por fibrosis pélvica extensa y (b) se acompaña de divertículos parauretrales, falsas vías, o lesión simultánea del cuello vesical.20 La mayoría de los defectos de distracción uretral complejos requieren una exposición quirúrgica más amplia para restablecer la continuidad uretral.21
Aunque la patogénesis de la PFPUDD en los niños tiende a seguir un patrón similar al de los adultos, deben considerarse varios elementos clave. La localización de la lesión uretral traumática en los niños suele ser impredecible debido a la posición abdominal de la vejiga y a la inmadurez de la próstata.22 Otros factores que deben considerarse en los niños son: (a) los defectos de distracción uretral tienden a ser más largos que en los adultos debido al marcado desplazamiento hacia arriba de la vejiga y la próstata, (b) las lesiones dobles en el cuello vesical y la uretra membranosa se observan con mayor frecuencia en los niños y (c) el tamaño prepuberal del periné puede dificultar alcanzar un extremo uretral proximal situado alto.23
Colapinto y McCallum24 clasificaron las lesiones traumáticas de la uretra posterior en tres categorías según el aspecto radiológico. En el tipo 1 se produce un desplazamiento de la próstata o del diafragma urogenital, pero la uretra membranosa está simplemente estirada y no seccionada. En el tipo 2 la uretra membranosa está rota por encima del diafragma urogenital, a nivel del vértice de la próstata. En el tipo 3 la uretra membranosa está rota por encima y por debajo del diafragma urogenital Recientemente, se propuso una nueva clasificación de la lesión uretral posterior en pacientes con fractura de pelvis.25 El nuevo esquema de clasificación permite comparar distintas estrategias terapéuticas y sus resultados (Tabla 1)
Tabla 1 Clasificación anatómica y mecánica unificada de las estenosis uretrales traumáticas.
| Clase | Definición |
|---|---|
| I | Uretra posterior distendida pero intacta |
| II | Rotura de la uretra prostato-membranosa por encima del diafragma urogenital |
| III | Rotura parcial o completa de la uretra anterior y de la uretra posterior con interrupción del diafragma urogenital |
| IV | Lesión vesical que se extiende a la uretra |
| IVa | Lesión de la base vesical con extravasación periuretral que simula lesión de la uretra posterior |
| V | Lesión pura de la uretra anterior, parcial o completa |
Sigue existiendo debate entre los urólogos pediátricos sobre el enfoque superior: realineación uretral precoz con o sin reconstrucción primaria de la uretra seccionada frente a SPC primaria y reparación diferida de la uretra. Nerli et al.26 informaron que la mitad de los niños sometidos a realineación primaria necesitaron uretrotomías endoscópicas adicionales, mientras que algunos requirieron uretroplastia para tratar una estenosis resultante. El autor prefiere la SPC primaria para superar la fase aguda de retención tras el traumatismo. También preferimos evitar la instrumentación uretral que puede agravar el daño uretral o una exploración pélvica arriesgada que puede alterar un hematoma e impedir una adecuada aproximación. Tras un período de 6-8 meses, cuando se retira la estabilización ortopédica, se realiza un uretrograma enfrentado para evaluar la localización y la longitud de la estenosis (Figura 6) Se han propuesto varios procedimientos quirúrgicos para la reparación diferida de los PFPUDDs. Estos incluyen dilatación uretral, técnicas endoscópicas como la OIU, procedimientos de sustitución y reparación anastomótica sin tensión diferida.
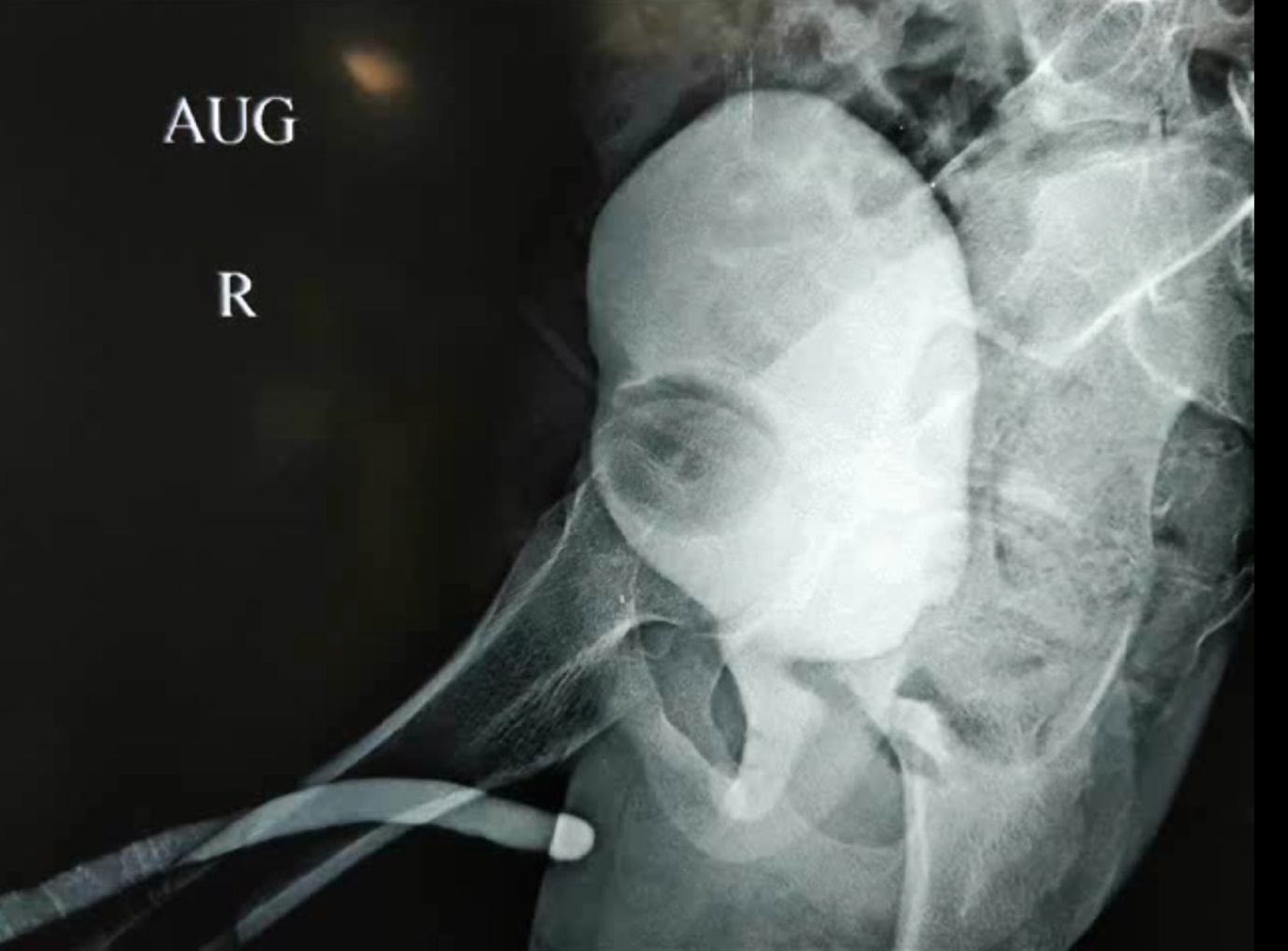
Figura 6 La uretrografía en oposición es un paso esencial para evaluar la extensión de los defectos de distracción uretral postraumáticos. Suele realizarse inyectando contraste desde la SPC para llenar la uretra posterior, mientras se inyecta a través del meato para llenar la uretra anterior.
La OIU puede ser ventajosa tanto para el manejo de estenosis anulares de la uretra membranosa tras lesiones uretrales parciales como para estenosis cortas no obliterativas después del fracaso de una reparación anastomótica primaria postraumática.27 El consenso actual es que la dilatación uretral y la OIU para PFPUDD no son aceptables en niños; ya que los resultados reportados han sido pobres, y los pacientes sometidos a estos procedimientos a menudo necesitan operaciones quirúrgicas adicionales.23,28
Uretroplastia anastomótica
La uretroplastia anastomótica es actualmente el enfoque preferido para el restablecimiento de la continuidad uretral en niños y adultos con PFPUDDs. El éxito de la uretroplastia anastomótica suele depender de una adecuada exposición quirúrgica, la exéresis de todo el tejido fibroso que ocupa el defecto de distracción, la movilización de la uretra bulbar normal, la fijación de mucosa sana en los bordes de los extremos uretrales bulbar y prostático y la realización de una anastomosis espatulada sin tensión (Figura 7), (Figura 8), cuando existe un aporte sanguíneo adecuado a través de la uretra. La reparación anastomótica puede intentarse mediante varios abordajes: (a) abordaje perineal, (b) acceso perineal elaborado en 1 tiempo, (c) abordaje transpúbico (parcial o total), (d) abordaje perineoabdominal progresivo (transpúbico), y (e) acceso sagital posterior.
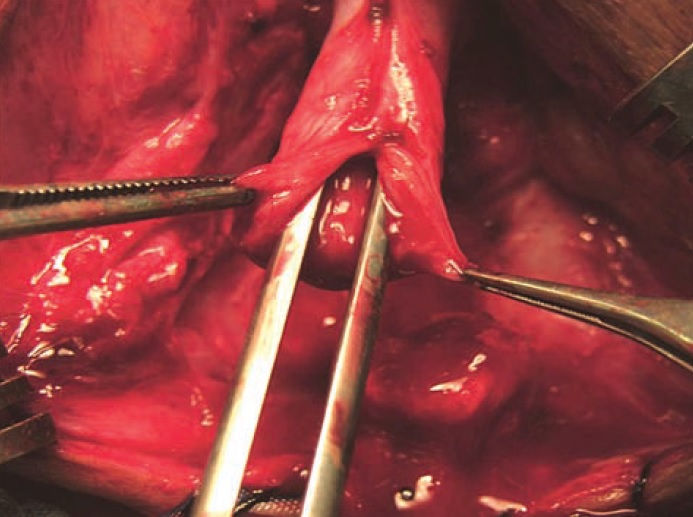
Figura 7 La movilización adecuada de la uretra bulbar y una anastomosis amplia tras la espatulación son pasos cruciales

Figura 8 La movilización de los pilares y el tallado de la rama púbica inferior ayudan a un trayecto más corto y a una mejor alineación
El abordaje perineo-abdominal (transpúbico) permite progresar de un acceso perineal a uno perineo-abdominal, con o sin pubectomía parcial, de acuerdo con las características anatómicas intraoperatorias del defecto de distracción uretral, y permite el reencauzamiento supracrural de la uretra movilizada si es necesario. El acceso perineal en un tiempo, cuidadosamente elaborado, proporciona maniobras escalonadas para lograr una anastomosis sin tensión: (a) movilización adecuada de la uretra bulbar, (b) separación de los cuerpos cavernosos proximales, (c) resección del margen inferior del arco púbico y (d) la posibilidad de reencauzar la uretra anterior alrededor de uno de los cuerpos cavernosos para acortar el trayecto de la uretra movilizada
Se informa una tasa de éxito global del 75-85% para la uretroplastia anastomótica.29 El fracaso de la uretroplastia perineal se atribuyó a una selección inadecuada de pacientes: defectos de distracción de al menos 3 cm de longitud con desplazamiento cefálico significativo de la próstata. En los niños con PFPUDD, la reparación quirúrgica debe iniciarse mediante una exposición perineal y, cuando no sea posible una anastomosis sin tensión, se requiere un abordaje abdominal (pubectomía parcial) para la corrección del defecto de distracción.21
Conclusiones
Las causas iatrogénicas (cateterización, PUV, reparación de hipospadias) representan la mayoría de las estenosis uretrales anteriores en el grupo etario más joven; mientras que, a medida que el niño crece, las estenosis uretrales traumáticas y posteriores pasan a predominar. El tratamiento inicial de las lesiones traumáticas de uretra posterior asociadas a fracturas pélvicas debe orientarse a estabilizar al paciente, SPC y tratar las lesiones asociadas que amenazan la vida. La evaluación preoperatoria del defecto de distracción uretral establecido incluye uretrografía en oposición y cistoscopia para definir la extensión anatómica del defecto de distracción uretral. Cuando hay una uretra anterior sana, la uretroplastia anastomótica es ideal para tratar los PFPUDDs. Las uretroplastias de sustitución con injerto BMG/OMG en inlay están indicadas principalmente para las estenosis panuretrales.
Referencias
- Herle K, Jehangir S, Thomas RJ. Stricture Urethra in Children: An Indian Perspective. J Indian Assoc Pediatr Surg 2018; 23 (4): 192–197, DOI: 10.4103/jiaps.JIAPS_146_17.
- Ansari MS, Yadav P, Srivastava A, Kapoor R, Shekar PA. Etiology and characteristics of pediatric urethral strictures in a developing country in the 21st century. J Pediatr Urol 2019; 15 (4): 403 1–403 8, DOI: 10.1016/j.jpurol.2019.05.020.
- Harshman MW, Cromie WJ, Wein AJ, Duckett JW. Urethral Stricture Disease in Children. J Urol 1981; 126 (5): 650–654, DOI: 10.1016/S0022-5347(17)54675-3.
- Kaplan GW, Brock WA. Urethral Strictures in Children. J Urol 1983; 129 (6): 1200–1203, DOI: 10.1016/S0022-5347(17)52641-5.
- Mori Y. Treatment of congenital urethral stenosis (urethral ring) in children. Optic internal urethrotomy in the congenital bulbar urethral stenosis in boys. Nihon Hinyokika Gakkai Zasshi 1989; 80 (5): 704–710, DOI: 10.5980/jpnjurol1989.80.704.
- Gobbi D, Leon FF, Gnech M, Midrio P, Gamba P, Castagnetti M. Management of Congenital Urethral Strictures In Infants. Case Series. Urol J 2019; 16 (1): 67–71, DOI: 10.22037/uj.v0i0.4045.
- Lal R, Bhatnagar V, Mitra DK. Urethral strictures after fulguration of posterior urethral valves. J Pediatr Surg 1998; 33 (3): 518–519, DOI: 10.1016/S0022-3468(98)90102-6.
- Myers DA, Walker RD. Prevention of Urethral Strictures in the Management of Posterior Urethral Valves. J Urol 1981; 126 (5): 655–656, DOI: 10.1016/S0022-5347(17)54676-5.
- Babu R, Kumar R. Early outcome following diathermy versus cold knife ablation of posterior urethral valves. J Pediatr Urol 2013; 9 (1). DOI: 10.1016/j.jpurol.2012.02.014.
- Payne CE, Sumfest JM, Deshon GEJ. Buccal mucosal graft for hypospadias repairs. Tech Urol 1998; 4 (4): 173–176.
- Barbagli G. Correlation Between Primary Hypospadias Repair and Subsequent Urethral Strictures in a Series of 408 Adult Patients. Eur Urol Focus 2017; 3 (2–3): 287–292, DOI: 10.1016/j.euf.2017.02.005.
- Ye W-J, Ping P, Liu Y-D, Li Z, Huang Y-R. Single stage dorsal inlay buccal mucosal graft with tubularized incised urethral plate technique for hypospadias reoperations. Asian J Androl 2008; 10 (4): 682–686, DOI: 10.1111/j.1745-7262.2008.00398.x.
- Schwentner C. Interim outcome of the single stage dorsal inlay skin graft for complex hypospadias reoperations. J Urol 2006; 175 (5): 1872–1877, DOI: 10.1016/S0022-5347(05)01016-5.
- Palminteri E, Berdondini E, Verze P, Nunzio C, Vitarelli A, Carmignani L. Contemporary urethral stricture characteristics in the developed world. Urology 2013; 81 (1): 191–196, DOI: 10.1016/j.urology.2012.08.062.
- Celis S. Balanitis xerotica obliterans in children and adolescents: A literature review and clinical series. J Pediatr Urol 2014; 10 (1): 34–39, DOI: 10.1016/j.jpurol.2013.09.027.
- Dubey D, Kumar A, Mandhani A, Srivastava A, Kapoor R, Bhandari M. Buccal mucosal urethroplasty: a versatile technique for all urethral segments. BJU Int 2005; 95 (4): 625–629, DOI: 10.1111/j.1464-410X.2005.05352.x.
- Barbagli G, Sansalone S, Kulkarni SB, Romano G, Lazzeri M. Dorsal onlay oral mucosal graft bulbar urethroplasty. BJU Int 2012; 109 (11): 1728–1741, DOI: 10.1111/j.1464-410X.2012.11006.x.
- Dubey D. Substitution urethroplasty for anterior urethral strictures: a critical appraisal of various techniques. BJU Int 2003; 91 (3): 215–218, DOI: 10.1046/j.1464-410x.2003.03064.x.
- Heinke T, Gerharz EW, Bonfig R, Riedmiller H. Ventral onlay urethroplasty using buccal mucosa for complex stricture repair. Urology 2003; 61 (5): 1004–1007, DOI: 10.1016/s0090-4295(02)02523-2.
- Turner-Warwick R. Prevention of complications resulting from pelvic fracture urethral injuries–and from their surgical management. Urol Clin North Am 1989; 16 (2): 335–358. DOI: 10.1016/s0094-0143(21)01515-9.
- Podesta M, Podesta MJ. Traumatic Posterior Urethral Strictures in Children and Adolescents. Front Pediatr 2019; 7: 24, DOI: 10.3389/fped.2019.00024.
- Hagedorn JC, Voelzke BB. Pelvic-fracture urethral injury in children. Arab J Urol 2015; 13 (1): 37–42, DOI: 10.1016/j.aju.2014.11.007.
- Koraitim MM. Posttraumatic posterior urethral strictures in children: a 20-year experience. J Urol 1997; 157 (2): 641–645. DOI: 10.1016/s0022-5347(01)65239-x.
- Colapinto V, McCallum RW. Injury to the male posterior urethra in fractured pelvis: a new classification. J Urol 1977; 118 (4): 575–580, DOI: 10.1016/s0022-5347(17)58110-0.
- Goldman SM, Sandler CM, Corriere JNJ, McGuire EJ. Blunt urethral trauma: a unified, anatomical mechanical classification. J Urol 1997; 157 (1): 85–89, DOI: 10.1016/s0022-5347(01)65291-1.
- Nerli RB, Koura AC, Ravish IR, Amarkhed SS, Prabha V, Alur SB. Posterior urethral injury in male children: long-term follow up. J Pediatr Urol 2008; 4 (2): 154–159, DOI: 10.1016/j.jpurol.2007.11.002.
- Helmy TE, Hafez AT. Internal urethrotomy for recurrence after perineal anastomotic urethroplasty for posttraumatic pediatric posterior urethral stricture: could it be sufficient? J Endourol 2013; 27 (6): 693–696, DOI: 10.1089/end.2012.0592.
- Hsiao KC. Direct vision internal urethrotomy for the treatment of pediatric urethral strictures: analysis of 50 patients. J Urol 2003; 170 (3): 952–955, DOI: 10.1097/01.ju.0000082321.98172.4e.
- Singla M. Posttraumatic Posterior Urethral Strictures in Children—Management and Intermediate-term Follow-up in Tertiary Care Center. Urology 2008; 72 (3): 540–543, DOI: 10.1016/j.urology.2008.02.078.
Última actualización: 2025-09-21 13:35