
20: Disfunción miccional
Este capítulo durará aproximadamente 43 minutos para leer.
Introducción
Los síntomas del tracto urinario inferior (LUTS), la disfunción vesical e intestinal (BBD) o el síndrome de eliminación disfuncional son términos que describen el conjunto común de síntomas, que va desde el síndrome de vejiga hiperactiva (OAB), el aplazamiento de la micción, la incontinencia urinaria de esfuerzo y la incontinencia de la risa hasta la micción disfuncional, entre otros.1 El impacto de la incontinencia urinaria diurna en los niños puede ser bastante profundo—con efectos sociales, emocionales y conductuales en la vida diaria.2 A partir de nuestro conocimiento de la OAB, sabemos que si persiste durante un período prolongado, se observa un engrosamiento de la pared vesical, lo que puede tener un impacto de por vida. A medida que los pacientes envejecen, las consecuencias se vuelven más profundas y requieren un mayor esfuerzo para corregirlas.3,4
Desde la perspectiva de la urología pediátrica, el niño con OAB tiene probabilidades de convertirse en un adulto con problemas de OAB. Esta correlación se ha observado en dos informes publicados. En el primer estudio, Fitzgerald et al3 revelaron que la micción diurna frecuente en la infancia se correlacionaba con la urgencia en la edad adulta, y existía una correlación entre la nicturia infantil y la adulta. La incontinencia diurna en la infancia y la enuresis nocturna se asociaron con más del doble de asociación con la incontinencia de urgencia en la edad adulta. Además, los antecedentes de infección del tracto urinario (ITU) en la infancia se correlacionaron con ITU en la edad adulta. En otro estudio de Minassian et al que involucró a 170 mujeres adultas, encontraron que había una mayor prevalencia de disfunción miccional en la infancia en mujeres que presentaban frecuencia urinaria, urgencia y incontinencia de esfuerzo o de urgencia.4 También señalaron que las pacientes sintomáticas tenían mayor probabilidad de presentar un IMC más alto. La tendencia ha sido tranquilizar a los padres diciendo que estos problemas son autolimitados y se resolverán a medida que el niño madure. Parece que la resolución espontánea no siempre ocurre y que algunos niños, a medida que maduran, son mejores para compensar sus problemas y finalmente no continúan el seguimiento. Una mejor comprensión de las posibles causas de la OAB infantil puede prevenir problemas innecesarios en la edad adulta y hacer mucho más felices a muchos niños, padres y maestros.
Genética
Existe evidencia creciente de que los factores genéticos desempeñan un papel importante en la incontinencia urinaria. Los hijos de padres que tienen OAB y/o problemas psiquiátricos subyacentes tienden a ser más refractarios a los tratamientos convencionales de la OAB.3,5 Estos hallazgos han sido corroborados por Labrie et al, cuya investigación muestra que las madres de niños con OAB o micción disfuncional tienen más probabilidades de haber presentado síntomas similares en la infancia que las madres de niños sin síntomas de LUT (28.9% frente a 16.3%, p<0.02, respectivamente).5 Los padres de niños con síntomas de LUT tenían más probabilidades de haber tenido resolución tardía de su enuresis nocturna (6% y 6.5% en niños y niñas, respectivamente) y, además, los padres que presentaban incontinencia diurna tuvieron una tasa estadísticamente significativa de incontinencia durante la infancia de 9.25% frente a 4.6% (p<0.0001).5 Los datos de adultos pueden utilizarse como sustituto para los niños. Al examinar los datos disponibles, algunos estudios indican una predisposición genética a LUTS en algunos pacientes. Una metodología de uso común para determinar la importancia de la influencia genética es el uso de estudios con gemelos. Un estudio sueco que incluyó a más de 25000 gemelos reveló evidencia de un vínculo genético para la susceptibilidad a la incontinencia urinaria, la frecuencia urinaria y la nicturia en mujeres.6 No hubo datos suficientes en pacientes varones para sacar conclusiones. Por otro lado, en un estudio que examinó un metanálisis de polimorfismos/genes candidatos en hombres se identificaron cinco genes: ACE, ELAC2, GSTM1, TERT y VDR. La heterogeneidad fue alta en tres de estos metanálisis. La variante rs731236 del receptor de vitamina D tuvo un efecto protector para LUTS (odds ratio: 0.64; intervalo de confianza del 95%, 0.49–0.83) con heterogeneidad moderada (I2 = 27.2%).7
Al revisar la literatura psiquiátrica, hay un gran número de estudios que vinculan los trastornos psicológicos y los LUTS. La asociación entre la incontinencia urinaria y el bienestar psicológico en adultos también ha sido señalada por Botlero et al.8 La depresión mayor puede predecir el inicio de la incontinencia urinaria en mujeres en una muestra basada en la población en riesgo.9 Un estudio encontró tasas aumentadas de enuresis en el trastorno bipolar del adulto (18%).10 También se ha descrito una asociación con el trastorno de pánico y la cistitis intersticial.11 También se encontró que la incontinencia diurna era un marcador del desarrollo premórbido de la esquizofrenia (SCZ).12 Los autores encontraron que los pacientes con SCZ tenían tasas más altas de enuresis infantil (21%) en comparación con los hermanos (11%) o los pacientes control (7%), y el riesgo relativo de enuresis estaba aumentado en los hermanos. Los pacientes con enuresis rindieron peor en dos pruebas cognitivas del lóbulo frontal (fluidez por letras y fluidez por categorías) en comparación con los pacientes no enuréticos. Cabe destacar que las alteraciones cerebrales asociadas con estos trastornos tienden a agruparse alrededor de la corteza cingulada anterior (ACC) y la corteza prefrontal (PFC), exactamente donde se están observando alteraciones en pacientes con urgencia e incontinencia de urgencia en fMRI.13,14
Epidemiología
La prevalencia de la incontinencia diurna varía ampliamente de un estudio a otro. A los 7 años de edad, la tasa de incontinencia diurna oscila entre el 4,9 % y el 11,7 %.15,16 A los 11–12 años de edad, la prevalencia oscila entre el 0,8 % y el 12,5 %.17,18,19,20,21 Se realizó un metanálisis de estos 3 estudios, que arrojó una prevalencia global del 6,4 %. El estudio longitudinal inglés ALSPAC, el más importante en aportar evidencia de forma continua, encontró las siguientes trayectorias de la incontinencia diurna en el rango de edad de 4,5-9,5 años:22
i. Normativo (86.2%); continentes a los 4.5 años ii. Tardío (6.9%); probabilidad de incontinencia diurna que disminuye de forma constante del 80% a los 4.5 años de edad a < 10% a los 9.5 años de edad iii. Persistente (3.7%); probabilidad de incontinencia diurna > 80% hasta los 7.5 años de edad con reducción constante hasta 60% a los 9.5 años de edad iv. Recidivante (3.2%); probabilidad de incontinencia diurna <10% a los 5.5 años de edad que aumenta a 60% a los 6.5 años con descenso lento posteriormente.
No hubo diferencias por sexo en el grupo de inicio tardío, pero las niñas superaron en número a los niños en los grupos persistente y recidivante. Un estudio de Stone et al que evaluó a niños con incontinencia urinaria persistente sometidos a investigación urodinámica e imágenes de la columna vertebral reveló que, si se extrapolaba a los 18 años de edad, hasta el 33% de los niños que presentaban enuresis a los 10 años de edad probablemente persistirían con alguna forma de síntomas urinarios.23
Comorbilidad neuropsiquiátrica
Los niños con trastornos de la eliminación presentan una mayor tasa de trastornos conductuales y psicológicos coexistentes; aproximadamente el 20–40% de los niños con incontinencia urinaria diurna están afectados por trastornos conductuales.24,25,26 En un amplio estudio epidemiológico de 8213 niños de 7,5–9 años, los niños con incontinencia urinaria diurna presentaron tasas significativamente aumentadas de trastornos psicológicos, especialmente ansiedad por separación (11,4%), trastorno por déficit de atención e hiperactividad (TDAH) (24,8%), conducta oposicionista (10,9%) y problemas de conducta (11,8%).27 En la misma cohorte, se evaluó a 10,000 niños de 4–9 años; el retraso en el desarrollo, el temperamento difícil y la depresión/ansiedad materna se asociaron con la incontinencia urinaria diurna y el ensuciamiento.28 En otro estudio poblacional que incluyó a 2856 niños, la incidencia de incontinencia fue del 16,9% en los 6 meses previos.29 En un estudio retrospectivo de pacientes con TDAH, el 20,9% se mojaba por la noche y el 6,5% se mojaba durante el día. Los odds ratios fueron de 2,7 y 4,5, respectivamente, lo que demuestra una asociación inespecífica del TDAH con el mojado nocturno y diurno.30 Entre los posibles trastornos gastrointestinales de la eliminación, los niños con incontinencia fecal (o encopresis) presentaban las tasas más altas de trastornos conductuales comórbidos: el 30–50% de todos los niños tenían alteraciones conductuales clínicamente relevantes.24,25 En un estudio epidemiológico con más de 8242 niños, aquellos de 7 a 8 años de edad presentaron una amplia gama de trastornos coexistentes (DSM-IV), incluidos ansiedad por separación (4,3%), fobias sociales (1,7%), fobias específicas (4,3%), ansiedad generalizada (3,4%), trastornos depresivos (2,6%), TDAH (9,2%) y conducta negativista desafiante (11,9%). Un estudio previo encontró que los pacientes descritos como que presentaban psiconeuroticismo tenían menos probabilidades de responder al tratamiento de la inestabilidad del detrusor que aquellos que no presentaban ninguna forma de psiconeuroticismo. La mayoría de los buenos respondedores y un tercio de los no respondedores estaban libres de problemas psiquiátricos.31 Es importante destacar que el 25% de los pacientes de este estudio presentaba síntomas de síndrome del intestino irritable.
Evaluación
Historia
La evaluación del niño con DVI comienza con una anamnesis detallada y un examen físico. Una historia clínica clara ayuda a determinar la sintomatología predominante y cuándo tienden a presentarse los síntomas. En general, es mejor intentar obtener la historia pertinente del niño si este colabora. Cuando no es posible obtenerla del niño, puede no haber más opción que obtenerla de los padres. Signos de urgencia como cruzar las piernas, correr al baño, agarrarse el pene, frotarse el clítoris, ponerse en cuclillas y sentarse sobre los talones (reverencia de Vincent) son todos signos de urgencia. Es fundamental llevar un diario miccional. La frecuencia urinaria es otra manifestación de la VHA y cuantificar el volumen y el número de veces que el paciente micciona es útil para determinar si existe una frecuencia verdadera. La incontinencia urinaria de urgencia es un sello clásico de la vejiga hiperactiva. Debe documentarse el momento en que ocurre la incontinencia para ayudar a identificar cualquier asociación con el intestino. No es infrecuente que los niños con una gran carga fecal presenten urgencia e incontinencia de urgencia después de una comida. Esto probablemente se deba a la estimulación de las contracciones colónicas por el reflejo gastrocolónico. Está bien establecido que existe comunicación cruzada en la médula espinal entre el colon y la vejiga.32,33,34,35 Esto puede desencadenar contracciones vesicales o al menos provocar síntomas de urgencia. El goteo posmiccional es un signo de relajación incompleta de todo el complejo esfinteriano o del esfínter externo. Es común en niños con micción disfuncional. También se observa con frecuencia en pacientes con micción disfuncional la disuria o la uretrorragia no asociadas a infección, sino más bien debidas a micción disinérgica.33
La disinergia del esfínter interno se ha asociado con mareo y disfunción autonómica (hipotensión al ponerse de pie sin incremento concomitante de la frecuencia cardíaca) tanto en varones como en mujeres cuando se les pregunta si se marean al ponerse de pie.36
Se debe obtener directamente del propio paciente una anamnesis exhaustiva de sus hábitos intestinales. Muchos padres no son conscientes de la verdadera naturaleza de las deposiciones de sus hijos y muchos informarán que las deposiciones de sus hijos son normales, mientras que los niños los contradicen rotundamente. Se debe obtener documentación sobre el tamaño y la naturaleza de las deposiciones. El uso de un diagrama es muy beneficioso y facilita la comunicación con el niño.37 Es importante señalar si las deposiciones son dolorosas o se asocian con sangrado rectal. Las deposiciones muy grandes y voluminosas suelen ser un indicador de evacuaciones infrecuentes. El dolor o el sangrado rectal pueden asociarse con disinergia del esfínter anal externo. Los pacientes con diarrea o síntomas de colitis también pueden presentar problemas de vejiga hiperactiva. El dolor periumbilical crónico es otro signo de que existe un problema de estreñimiento o alteraciones de la homeostasis de la serotonina en el intestino. Muchos niños se quejan de este dolor y, una vez que se instaura un régimen intestinal, el dolor desaparece.
Debe utilizarse un cuestionario estandarizado para evaluar a los pacientes en la primera consulta y en el seguimiento. Hay 2 cuestionarios de uso común que han sido validados para niños; el primero es el DVSS y el otro es la Escala de Vancouver.38,39 Además, existe un cuestionario que evalúa el perfil psiquiátrico del niño y es muy útil para realizar un cribado rápido de problemas subyacentes de atención, hiperactividad, depresión y ansiedad en niños, que se asocian frecuentemente con los LUTS.40
Examen físico
El examen físico es útil en la evaluación y puede ser muy revelador. La exploración del abdomen es fundamental para determinar si hay heces palpables en el colon. La palpación desde el cuadrante inferior izquierdo hasta el cuadrante superior izquierdo suele evidenciar grandes cantidades de heces presentes en estos abdómenes. En muchos casos, los padres pueden negar problemas intestinales. La distensión gaseosa del colon es igual de problemática y debe registrarse, ya que puede conducir a los mismos problemas que el estreñimiento.
El examen de la espalda generalmente revelará una espalda de apariencia normal y pliegues anocutáneos. La rara presencia de aplanamiento de los glúteos o de pliegues anormales en la articulación sacroilíaca (SI) es indicativa de una anomalía sacra (Figura 1) y (Figura 2) Observar al niño al caminar también puede ayudar a identificar un posible problema neurológico si presenta marcha en puntillas. Los pies con arco alto son otra posible pista de alguna forma de afección neurológica. Los hoyuelos sacros bajos por lo general no son motivo de preocupación. Solo preocupan los hoyuelos que están asociados con un penacho piloso o que se encuentran más arriba en la espalda y deben evaluarse con una resonancia magnética de la columna lumbosacra.

Figura 1 Hendidura sacra anómala asociada con médula anclada.

Figura 2 Apéndice parasacro asociado con anclaje medular.
Pruebas diagnósticas
A continuación discutimos las pruebas diagnósticas que realizamos en el orden en que las efectuamos para optimizar nuestro manejo y minimizar las pruebas invasivas en los pacientes.
Análisis de orina
La primera y más importante prueba clínica que debe realizarse en todos los niños que se presentan con BBD es el análisis de orina. Un análisis de orina simple debería ayudar a determinar si los síntomas se deben a una infección o a BBD. No es raro observar microhematuria en pacientes que presentan micción disinérgica, la cual se asocia frecuentemente con BBD.
Residuo posmiccional
Debe realizarse un PVR en todos los pacientes evaluados por LUTS y DV. Esta es la información más importante con la que se cuenta en las etapas iniciales de la evaluación y puede brindarle de inmediato una mayor comprensión de los posibles problemas que deben abordarse. Los residuos elevados pueden asociarse con ITU recurrentes o con micción frecuente, mientras que un PVR bajo también puede asociarse con frecuencia miccional, pero la etiología subyacente de dicha frecuencia será diferente.
Se prefiere un dispositivo capaz de proporcionar una imagen real de la vejiga en lugar de un dispositivo que ofrece una imagen representativa. Esto es valioso, ya que también se puede medir el diámetro rectal. Los diámetros rectales superiores a 4 cm se asocian con BBD y los estudios han mostrado que la corrección de esta dilatación se asocia con mejoría de los síntomas.
Uroflujometría/EMG
La uroflujometría es una herramienta importante para ayudar a determinar si el niño micciona de forma anormal. El uso de las 5 curvas clásicas, campana, torre o hipervaciador, staccato, interrumpida y curva de meseta, está en proceso de ser reemplazado por un sistema modificado que se basa en si la curva es suave o fraccionada y en un índice de flujo. El índice de flujo es independiente del volumen, por lo tanto puede utilizarse para comparar flujos en todos los volúmenes y a través de múltiples edades.41,42,43 Además, los índices de flujo son una medida de la eficiencia miccional, que es una representación mucho más precisa del flujo que las descripciones de la forma.
El uso de la uroflujometría se ve aún más potenciado por el uso concomitante de una EMG de los músculos perineales. El uso de la EMG perineal nos permite determinar si el niño micciona con disinergia del esfínter externo (aumento de la actividad muscular perineal) y diagnosticar la disinergia del esfínter interno con base en el tiempo de latencia y la forma de la curva de flujo (típicamente meseta o índice de flujo <=0.7).44
Ecografía renal y vesical
La ecografía renovesical no es esencial para niños con LUTS no asociados a infección. Por otro lado, un paciente con infecciones recurrentes debe someterse a evaluación de las vías urinarias superiores para buscar discrepancias de tamaño e hidronefrosis, que podrían ser indicativas de reflujo o de sus consecuencias. En pacientes con incontinencia persistente, la ecografía es útil para descartar una duplicación renal asociada a un uréter ectópico. La dilatación de un uréter puede ser otro indicio que sugiera un uréter ectópico. En pacientes con micción obstructiva, la ecografía vesical ayuda a identificar la presencia de un ureterocele obstructivo. El engrosamiento de la pared vesical puede apreciarse en la ecografía y es un indicador útil de obstrucción o hiperactividad vesical.
KUB y AP y lateral de la columna vertebral
En algunos niños en los que el hábito corporal hace que la palpación de heces sea poco confiable, puede ser necesario considerar una KUB para evaluar la carga fecal colónica o para valorar el progreso con un régimen intestinal. Si se realiza una KUB, es razonable considerar una placa AP y lateral del sacro para confirmar que no haya anomalías sacras (Figura 3) En algunos niños, una KUB puede ser inadecuada para verificar que la columna vertebral sea normal debido a la superposición de heces que oculta el sacro.

Figura 3 La radiografía lateral de la columna vertebral muestra claramente segmentos sacros que no serían visibles debido a una gran carga fecal en este paciente.
Cistouretrografía miccional
Una VCUG bien realizada aporta una enorme cantidad de información sobre la dinámica de la micción, además de la presencia o ausencia de reflujo, uréteres ectópicos o válvulas. Se puede observar la apertura del cuello vesical y también se puede ver el esfínter externo cuando se abre y se cierra. La presencia de la uretra en trompo es un ejemplo clásico de disinergia del esfínter externo (Figura 4) Una VCUG no está indicada en todos los pacientes con LUTS. Se debe realizar una VCUG en los casos refractarios para definir con mayor detalle la dinámica de la micción y confirmar que no se pase por alto ningún problema anatómico.
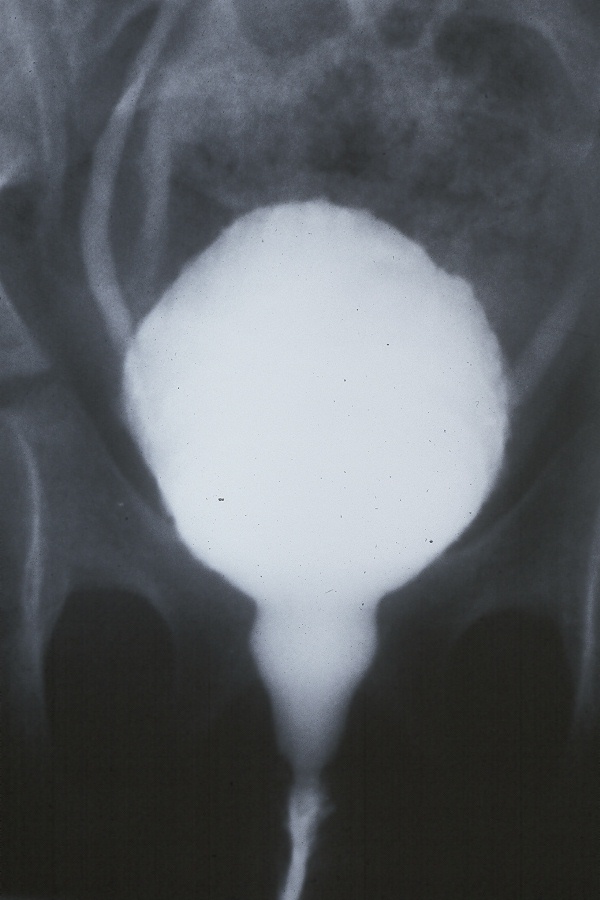
Figura 4 Uretra en peonza en paciente femenina con reflujo e infecciones urinarias recurrentes.
Resonancia magnética de la columna vertebral
Los estudios de imagen del sacro están indicados cuando el paciente presenta una lesión evidente en la espalda, como se mencionó previamente en la sección del examen físico. En pacientes en quienes han fracasado todos los intentos de tratamiento y la incontinencia persiste, también puede estar indicada una RM de la columna vertebral. Recomendamos realizar la RM antes de los estudios urodinámicos, ya que la hiperactividad del detrusor en los urodinámicos no es diagnóstica de disfunción vesical neurógena. Por lo tanto, el paciente necesitará una RM de la columna de todos modos y es mejor proceder primero con la prueba definitiva. La médula anclada oculta ocurre muy infrecuentemente cuando no hay estigmas cutáneos.45
Urodinámica
En pacientes con LUTS, el estudio urodinámico a menudo solo confirma lo que ya se desprende de una historia clínica exhaustiva: que existen contracciones no inhibidas (UIC). Bael et al justifican esta afirmación, ya que demostraron que no había beneficio en realizar un estudio urodinámico en niños con BBD.46 La presencia de UIC no permite confirmar ni excluir la existencia de una lesión neurológica. El único hallazgo de importancia es la ausencia de una contracción del detrusor, ya evidente en el estudio de uroflujometría que demuestra una curva de flujo deficiente. Esto no significa que no exista indicación para realizar UDS en niños. En algunas ocasiones, los estudios urodinámicos se realizan simultáneamente con la VCUG. En algunos casos, los UDS pueden ayudar a identificar la fuente del escape urinario, especialmente cuando se combinan con fluoroscopia.
Opciones de tratamiento
Uroterapia
La uroterapia es un término paraguas para todas las intervenciones no quirúrgicas y no farmacológicas para los problemas funcionales de la vejiga y del intestino en niños y adolescentes. Es el pilar del tratamiento para la incontinencia urinaria diurna, así como para la enuresis nocturna, el estreñimiento funcional y la incontinencia fecal.47,48
El objetivo de la uroterapia es normalizar el patrón miccional e intestinal y prevenir nuevas alteraciones funcionales. Se distingue entre uroterapia estándar y uroterapia específica. Deben cumplirse tres condiciones antes de iniciar la uroterapia. Primero, un diagnóstico claro de incontinencia funcional. Segundo, el niño debe estar listo para la escolarización; cuando el niño es demasiado inmaduro, puede no tener las habilidades cognitivas o las capacidades motoras para comprender y completar la uroterapia. Tercero, una buena anamnesis psicosocial, ya que los problemas psicosociales o conductuales también pueden influir en la eficacia de la terapia y pueden requerir evaluación psiquiátrica o terapia familiar.49,50
La uroterapia estándar consiste en educación y desmitificación, instrucciones de modificación del comportamiento, consejos sobre el estilo de vida respecto a la ingesta de líquidos, registro de la frecuencia de micción, de los volúmenes miccionales y de los episodios de incontinencia, y apoyo y estímulo a los niños y sus padres.51 La uroterapia comienza con una explicación de la función y disfunción de la vejiga y del intestino, explicando las causas de la incontinencia. Se deben dar instrucciones sobre la ingesta adecuada de líquidos y la micción regular durante el día. También se deben proporcionar instrucciones sobre la postura adecuada en el inodoro. Debe llevarse un diario miccional para el autoseguimiento y la motivación. El diario proporciona al niño y a los padres información sobre el progreso del tratamiento. Tras la explicación y las instrucciones, el niño practica en casa durante un máximo de tres meses. Durante este periodo, se debe proporcionar asesoramiento frecuente y el progreso debe evaluarse con frecuencia. Estas evaluaciones intermedias pueden realizarse por telemedicina y/o mediante visitas regulares a la clínica.
El estreñimiento o las infecciones del tracto urinario (ITU) deben abordarse antes de la uroterapia.47,48 Como la disfunción intestinal y vesical se afectan mutuamente, la uroterapia es menos eficaz si la función intestinal y/o las ITU no se abordan durante el tratamiento.51,52
El éxito del tratamiento se determina por el grado en que el niño y sus padres están satisfechos con los resultados. La satisfacción y la mejora de la calidad de vida pueden ser un motivo para finalizar el tratamiento en lugar de esforzarse por alcanzar los mejores resultados posibles. Cuando el tratamiento no tiene éxito, es importante identificar la causa.
Cuando los resultados de la uroterapia estándar son insatisfactorios, se recomienda la uroterapia específica. Esta terapia combina intervenciones especializadas como el biofeedback del suelo pélvico, la terapia cognitivo-conductual, la psicoterapia, la neuroestimulación o el cateterismo intermitente limpio.47,48,51,53 La uroterapia específica se adapta al tipo específico de disfunción vesical-intestinal y se compone de programas específicos para niños con síntomas refractarios al tratamiento. Estos programas ayudan a los niños a aprender cómo miccionar, cuándo miccionar y con qué frecuencia miccionar. La práctica repetida es necesaria para habituar el nuevo comportamiento miccional.50
Los niños con problemas de conducta requieren un plan adaptado a las necesidades únicas de cada niño.54 En presencia de comorbilidades y de sobreactividad vesical grave, puede ser necesario el tratamiento farmacológico.47
La uroterapia es un tratamiento eficaz que logra la continencia en el 56% de los niños en el plazo de un año, mientras que la tasa de curación espontánea de la incontinencia es del 15% por año. La uroterapia aborda todos los aspectos de la incontinencia, lo que conduce al mejor resultado clínico. Esto incluye los problemas somáticos, psicosociales y conductuales, así como la calidad de vida.55
Manejo intestinal
El estreñimiento agudo y simple o la distensión colónica, en muchos casos, pueden abordarse simplemente aumentando la hidratación y/o añadiendo jugos ricos en sorbitol, como los de ciruela pasa, pera y manzana, junto con frutas y verduras hechas puré, a la dieta normal del niño. El extracto de malta de cebada o el jarabe de maíz también pueden utilizarse para ablandar las heces. Otros cambios dietéticos incluyen reducir la ingesta excesiva de leche, ya que el calcio saponifica las heces y conduce a su endurecimiento. Además, actualmente no existe evidencia que respalde el uso de suplementos dietéticos prebióticos y/o probióticos como tratamiento del estreñimiento.56 Tras el fracaso de las intervenciones dietéticas, otras opciones de tratamiento incluyen laxantes osmóticos como el polietilenglicol (0.7 g/kg de peso corporal por día) lactulosa, sorbitol o leche de magnesia (dosis: 1–3 mL/kg de peso corporal por día). No existe evidencia de que la suplementación con fibra dietética o el biofeedback por sí solos sean intervenciones efectivas para el estreñimiento que requiere tratamiento médico.56 Muchos pacientes requieren terapia de mantenimiento para manejar sus síntomas persistentes de estreñimiento. En nuestra experiencia, los agentes osmóticos no son tan eficaces por sí solos como cuando se usan en combinación con laxantes de sen o bisacodilo. La preocupación de que los alcaloides del sen creen hábito o perjudiquen la motilidad colónica es un ‘mito popular’ y debe ignorarse: en algunos niños está justificado el uso agresivo de dichos medicamentos.57
El uso de agentes osmóticos por sí solos ha sido corroborado por Bush et al cuya investigación mostró que el polietilenglicol 350 no fue superior al placebo durante un ensayo de 1 mes.58 El manejo del estreñimiento puede resultar en una resolución de los síntomas de vaciamiento de hasta un 50% o más.59
Farmacológico
Anticolinérgicos
Los anticolinérgicos, (también conocidos como antimuscarínicos) se utilizan típicamente como tratamientos de primera línea de la OAB en niños cuyos síntomas han persistido tras la uroterapia. Actualmente, solo tres antimuscarínicos (oxybutynin [FDA y EMA] , Solfenacin [FDA y EMA] y tolterodine [EMA]) han recibido formalmente la aprobación para su uso en niños. Los ensayos clínicos que se han realizado en niños (estudios con oxybutynin, solifenacin, darifenacin) han incluido por lo general a pacientes con problemas miccionales neurogénicos demostrados y no han investigado los efectos de los antimuscarínicos en pacientes con síntomas LUT no neurogénicos o idiopáticos. Los datos publicados en 2006 sugieren que los efectos terapéuticos de los antimuscarínicos en pacientes considerados sin déficits neurológicos están mediados predominantemente por interacciones con la rama sensorial/aferente del arco reflejo más que con el lado eferente/motor.60 Los receptores muscarínicos se encuentran en células uroteliales, células suburoteliales de Cajal y en nervios aferentes.61 Los antimuscarínicos están activos durante la fase de llenado/almacenamiento de la micción cuando los nervios colinérgicos (eferentes o motores) no están activos. La acetilcolina puede generarse y liberarse desde el urotelio como respuesta al llenado de la vejiga/aumentos de tensión y también podría ‘fugarse’ desde las terminales nerviosas colinérgicas durante el llenado vesical62 seguido de la unión a los receptores M2 y M3 y podría ser un mecanismo de sobreactividad en pacientes con enfermedades vesicales..63
Se han identificado cinco subtipos distintos de receptores muscarínicos colinérgicos (M1–M5), y el músculo liso vesical expresa predominantemente dos de estos subtipos: M2 (70–80%) y M3 (20–30%). Se ha demostrado que la activación de los receptores M3 provoca la contracción del músculo liso, que es el estímulo principal para la contracción vesical. Se ha postulado que los receptores M2 y M3 están implicados no solo en la activación de la contracción del músculo liso por los nervios eferentes, sino también en la activación de los nervios sensitivos/aferentes.61 La activación de los receptores M2 en el urotelio podría revertir la relajación del músculo liso mediada por el sistema simpático que permite la fase de llenado o almacenamiento del ciclo miccional; aunque la activación de los receptores M2 podría provocar la contracción del músculo liso a través de otros mecanismos poco comprendidos.64
Los receptores M1 se encuentran en el cerebro, las glándulas (como las salivales) y los ganglios simpáticos. La activación de estos receptores explica la mayoría de los efectos adversos de los fármacos antimuscarínicos. La sequedad bucal es el síntoma más frecuente. También pueden presentarse estreñimiento, reflujo gastroesofágico, visión borrosa, retención urinaria y efectos secundarios cognitivos; estos síntomas suelen ser menos molestos en los niños. El potencial de efectos cognitivos adversos y de delirio también existe en los niños, pero por lo general se limita a situaciones de sobredosis.65,66,67 En ensayos clínicos en adultos, los datos electroencefalográficos cuantitativos sugieren que la oxibutinina tiene más efectos sobre el SNC que el trospio o la tolterodina.68,69
Alfa-bloqueadores
El uso de los alfa-bloqueadores (también conocidos como antagonistas de los adrenorreceptores α) en la disfunción miccional no neuropática fue popularizado por Austin et al para tratar la disfunción miccional en niños.70 Estos medicamentos se han utilizado en el manejo de pacientes con disfunción del cuello vesical y retención urinaria; estos agentes también son útiles para mejorar los síntomas de urgencia e incontinencia de urgencia en algunos niños.71 Los estudios en adultos indican que los alfa-bloqueadores son eficaces para el manejo de los síntomas irritativos debidos a stents y en hombres mayores con hiperplasia prostática benigna.72,73 Existe cierta evidencia de que la alfuzosina redujo la presión anal en reposo y durante la evacuación simulada en mujeres sanas y con estreñimiento en comparación con placebo, pero no mejoró los síntomas intestinales en mujeres con estreñimiento.74 En muchos pacientes, la terazosina, un alfa-bloqueador no selectivo, es el fármaco de primera línea para el tratamiento de la urgencia y el aumento de la frecuencia urinaria, debido a las propiedades no selectivas de este agente y a su potencial para atravesar la barrera hematoencefálica; sin embargo, los bloqueadores más selectivos del receptor α1, como la tamsulosina o la alfuzosina, son más adecuados para el manejo de la disfunción del cuello vesical que puede conducir a hipertrofia e inestabilidad del detrusor. Los alfa-bloqueadores no selectivos pueden causar hipotensión ortostática. Por lo tanto, estos agentes deben utilizarse con cuidado y se requiere una titulación gradual de la dosis. En pacientes con antecedentes familiares de desmayos fáciles o de hipotensión ortostática, la titulación de la dosis es esencial incluso con el uso de alfa-bloqueadores más selectivos. En su mayoría, los niños toleran bien los alfa-bloqueadores.75
Agonistas beta-3
Los agonistas del receptor adrenérgico β3, como el mirabegrón, pueden aumentar la capacidad vesical sin incrementar la presión miccional ni el volumen residual posmiccional.76 El tratamiento con estos agentes conduce a la relajación del músculo liso y el mecanismo de relajación generalmente aceptado es mediante la activación aguas abajo de la adenilato ciclasa con la producción subsiguiente de monofosfato de adenosina cíclico (AMPc), seguida de la inhibición de la vía de la Rho‑quinasa.77,78 Sin embargo, la evidencia indica además que el AMPc elevado también activa la proteína quinasa A, que a su vez activa canales de K+ de gran conductancia dependientes de calcio (BK). La activación de estos canales BK lleva a la hiperpolarización del músculo liso vesical y a una mayor estabilidad del detrusor.79 El mirabegrón está aprobado para el tratamiento de la vejiga hiperactiva (VHA) en adultos y niños en Estados Unidos y Europa.
Otros medicamentos
La imipramina es un antidepresivo tricíclico que afecta tanto a los receptores muscarínicos como a los α-adrenorreceptores con un posible efecto central sobre los reflejos miccionales.80 Cuando se introdujo la imipramina para tratar la depresión se observó que tenía efectos notables sobre la incontinencia urinaria de los pacientes. Hemos encontrado que la imipramina es un fármaco eficaz para controlar la incontinencia de urgencia en algunos niños que previamente se consideraron refractarios a la terapia antimuscarínica.81 Los efectos de la imipramina sobre la incontinencia urinaria podrían ser el resultado de un efecto en las áreas frontales del cerebro, que están implicadas en las funciones ejecutivas, incluido el control de la urgencia miccional. Alternativamente, los efectos urológicos de la imipramina podrían reflejar un efecto sobre los niveles de dopamina en el estriado, afectando así los niveles de ácido ɣ-aminobutírico (GABA) en la PAG. El aumento de los niveles de GABA en la PAG provoca la supresión del reflejo miccional.82,83
También se ha encontrado que la imipramina es útil para tratar a nuestros pacientes con incontinencia por risa. La imipramina puede causar hipotensión postural y también puede ser peligrosa en pacientes con alteraciones de la conducción cardíaca y debe usarse con precaución.
ISRS e IRNS
Los inhibidores selectivos de la recaptación de serotonina (ISRS) han demostrado funcionar a nivel del núcleo de Onuf modulando los reflejos de micción y de almacenamiento, los cuales dependen del glutamato. En presencia de glutamato, los ISRS potencian los efectos de las señales aferentes relacionadas con el almacenamiento vesical y también aumentan la salida eferente hacia el esfínter uretral externo, manteniendo así la contracción de dicho esfínter. En ausencia de glutamato, los ISRS no tienen efecto sobre la señalización y la activación parasimpática normal da lugar a la contracción de la vejiga y la relajación del esfínter.84 Este efecto de los ISRS en el componente de almacenamiento del arco reflejo podría explicar cómo la hiperactividad vesical de algunos pacientes mejora tras el tratamiento con ISRS. Estos agentes también podrían estar actuando en regiones cerebrales asociadas con el procesamiento de las señales de urgencia, como la ACG y la PFC.
Estimulación eléctrica
Neuroestimulación sacra
La neuroestimulación sacra (también conocida como neuromodulación sacra) implica la colocación de un electrodo en los forámenes S3 y a lo largo del nervio sacro, con la implantación subcutánea de un estimulador para proporcionar estimulación continua de baja intensidad del nervio. La estimulación de la médula espinal se utiliza con frecuencia en pacientes adultos y el interés en el uso de este enfoque en niños está en aumento. En una serie de 20 pacientes monitorizados prospectivamente con síndrome de eliminación disfuncional, descritos por Roth et al, la desaparición de los síntomas o una mejoría “>50%” de los síntomas se produjo en el 88% de los niños, de los cuales el 63% presentaba enuresis nocturna, el 89% aumento de la frecuencia urinaria diurna y el 59% estreñimiento. Este grupo ahora tiene experiencia con la neuroestimulación sacra en 187 pacientes, con resultados consistentes.85,86
Estimulación parasacra con estimulación nerviosa eléctrica transcutánea
La estimulación parasacra implica el uso de un dispositivo TENS y parches conductores parasacros, que se colocan de manera parasacra en la región S2–3 mientras que los electrodos se conectan en la superficie a un generador de corriente. Los estudios han utilizado estimulación a diversas frecuencias, que van de 10–80 Hz y frecuencias de tratamiento que van de semanal a diaria. Las duraciones de la estimulación también han variado de 20 minutos hasta 1 hora diaria. Walsh et al describieron por primera vez el uso de TENS en adultos en 1999, seguido por Hoebeke et al en 2001, quienes describieron su uso en niños.87,88 En estudios posteriores, la resolución completa de los síntomas ha oscilado entre 47–61.9% de los niños tratados con esta modalidad.89,90,91 Esta modalidad también se ha encontrado útil para estimular la motilidad intestinal mediante corriente interferencial cruzada.92
Estimulación periférica del nervio tibial
La estimulación eléctrica percutánea del nervio tibial (PTNS) se basa en la práctica china tradicional de utilizar puntos de acupuntura sobre los nervios peroneo común y tibial posterior para inhibir la actividad vesical.87,88 Una técnica consiste en utilizar una aguja de acero inoxidable de calibre 34, que se inserta aproximadamente 5 cm cefálicos al maléolo medial, justo posterior al borde de la tibia. Se coloca un electrodo adhesivo en la superficie medial del calcáneo. Este enfoque se ha evaluado en ensayos clínicos con resultados variables. Hoebeke et al informaron que 17 de 28 niños cuyos síntomas de OAB eran refractarios al tratamiento médico presentaron resolución o mejoría de sus síntomas en respuesta a sesiones semanales de PTNS de 30 minutos.91 DeGennaro et al informaron tras un seguimiento a largo plazo que 12 de 14 niños con OAB y 14 de 14 con micción disfuncional estaban asintomáticos tras dos años.88 Los autores sí señalaron que se requirió un uso ‘crónico’ persistente a largo plazo de la PTNS en el 50% y el 29% de los niños con OAB y micción disfuncional, respectivamente, para mantener estos resultados. En un estudio que comparó la eficacia de la TENS administrada en la región parasacra con la de la PTNS en niños con OAB, se observaron resultados significativamente mejores con el uso de TENS en comparación con PTNS (resolución completa observada en el 70% frente al 9% de los pacientes, respectivamente; P = 0.02).93 Figura 5 muestra un dispositivo de este tipo.
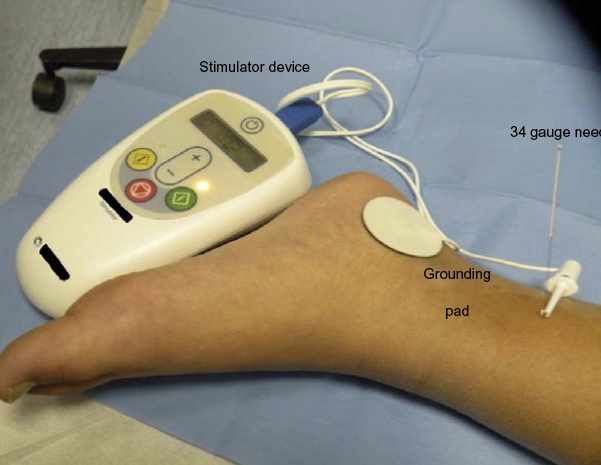
Figura 5 Estimulación PTNS en un niño.
Otra forma de estimulación del nervio tibial es aplicar parches sobre el nervio y estimular el nervio como la TENS parasacra. En un estudio que comparó la estimulación tibial posterior transcutánea y la estimulación simulada en 40 niños, las puntuaciones de QoL y las puntuaciones globales y diurnas de DVISS disminuyeron significativamente en ambos grupos, simulado y de prueba (p < 0.05). Además, la frecuencia de los episodios de incontinencia y de urgencia también se redujo significativamente (p < 0.05) en el grupo de tratamiento con PTNS. Este efecto en el grupo de prueba seguía vigente 2 años después de la intervención.94
Opciones quirúrgicas
Toxina botulínica A
Las inyecciones intravesicales de toxina botulínica A (BoNT-A) en el detrusor han sido aprobadas para su uso en adultos con vejiga hiperactiva (VH). Un estudio reciente publicado por Austin et al en pacientes neurogénicos ha demostrado la seguridad de la BoNT-A en niños y dio lugar a la aprobación por la FDA en niños con NDO.95 En adultos, las inyecciones de BoNT-A han demostrado ser un tratamiento útil para pacientes con VH refractaria y ofrecen una alternativa para los pacientes que no toleran la terapia anticolinérgica. Hay pocos estudios publicados sobre el uso de BoNT-A en niños, que consisten principalmente en cohortes clínicas seleccionadas no aleatorizadas de niños neurológicamente sanos con VH refractaria al tratamiento e incontinencia de urgencia.96,97,98 La dosis de BoNT-A es variable en estos estudios y oscila entre 50–200 unidades.96,97,98 Los datos de seguimiento de estos tres estudios, con un total de 55 pacientes, revelan que se logró una respuesta completa, definida como continencia total, en 38–70% de estos niños tras una sola, o repetidas, inyecciones. Se notificaron pocos eventos adversos clínicamente significativos; un paciente presentó una ITU y un paciente presentó retención urinaria transitoria.96,97
Biorretroalimentación
El biofeedback es el proceso de adquirir una mayor conciencia de la acción de los músculos del suelo pélvico y del esfínter utilizando instrumentos externos que proporcionan información sobre la acción de estos músculos, con el objetivo de aumentar la conciencia y el control voluntario por parte del niño.
En la uroterapia específica, el enfoque suele centrarse en la rehabilitación del suelo pélvico mediante entrenamiento con biorretroalimentación. El beneficio teórico de la biorretroalimentación es que los niños pueden visualizar directamente la actividad de sus músculos del suelo pélvico mediante EMG o la curva de uroflujometría.99 Esto facilita la defecación y ayuda al niño a tomar conciencia del músculo del suelo pélvico (contracción vs relajación). En la micción disfuncional debida a disinergia del esfínter externo, el objetivo es lograr una micción relajada, no obstructiva, y un vaciamiento vesical completo. La retroalimentación puede proporcionarse de forma inmediata sobre el desempeño, como con la EMG o la ecografía, o como conocimiento de resultados, como con la uroflujometría y la medición del residuo posmiccional.100
La retroalimentación de la EMG puede emplearse para enseñar al niño a contraer y relajar a voluntad los músculos del suelo pélvico.99 El uso de la uroflujometría en tiempo real ayuda al niño a observar la curva de flujo durante la micción. Se puede enseñar a los niños a orinar con los músculos del suelo pélvico relajados y un volumen de orina normal al lograr una curva de flujo continua con forma de campana. Puede utilizarse la ecografía para comprobar si la vejiga está vacía después de la micción e informárselo al niño.
El impacto del biofeedback en pacientes con micción disfuncional que presentan reflujo es significativo, ya que observamos una resolución espontánea del reflujo del 60% en niños de 6 años o más tratados con biofeedback.101 Algunos han afirmado que el biofeedback también es eficaz para la urgencia; su mecanismo podría ser la reducción de la resistencia de la salida vesical durante la micción, lo que conduce a hipertrofia del detrusor y, por ende, a inestabilidad del detrusor. Por otro lado, existen estudios en adultos que indican que puede ser eficaz en pacientes con vejiga hiperactiva (VHA) debido a la terapia continua individual (uno a uno) que recibe el paciente y a la mejora del bienestar mental del paciente.102
La terapia de biofeedback está limitada por la capacidad del niño para cooperar con el profesional de la salud que dirige la sesión. Los niños menores de cinco años de edad generalmente son incapaces de realizar biofeedback de forma regular. Los niños con discapacidades de aprendizaje significativas, problemas de conducta y otros problemas neurológicos no son candidatos ideales para el biofeedback. Estudios adicionales revelan que la terapia de biofeedback es útil en la eliminación del reflujo en niños que presentan evidencia de disinergia del esfínter externo.103,104
Es un malentendido pensar que el biofeedback por sí solo es suficiente para lograr la continencia. En la práctica, los profesionales combinan inadvertidamente el biofeedback con educación e instrucciones. Al hacerlo, también proporcionan modificación conductual mientras piensan que solo ofrecen entrenamiento con biofeedback. En la uroterapia, el biofeedback es solo uno de los elementos del tratamiento; el tipo de biofeedback no es un factor decisivo en el resultado del tratamiento.51
Trastornos
Vejiga hiperactiva
Evaluación y diagnóstico
La característica distintiva de la vejiga hiperactiva (OAB) es la urgencia y, por definición, puede decirse que los niños con este síntoma presentan OAB. La incontinencia y el aumento de la frecuencia miccional suelen estar presentes. La incontinencia de urgencia simplemente significa incontinencia en presencia de urgencia y es aplicable a muchos niños con OAB. Existe evidencia creciente de que la OAB es un problema sensorial; si se localiza en el sistema nervioso central (SNC) o a nivel vesical es objeto de debate. Los niños con incontinencia no asociada a una urgencia miccional súbita o que tardan en reconocer la urgencia tienen más probabilidades de presentar un problema neurológico o una alteración del procesamiento del lóbulo frontal, como el TDAH.
Opciones de tratamiento y escollos
- Uroterapia, programa intestinal
- Evitar la diarrea o los accidentes fecales por el uso mal controlado o excesivamente agresivo de agentes osmóticos y catárticos
- Evitar el exceso de gas por sobrecarga de fibra; el gas es tan perjudicial como el estreñimiento y produce distensión del intestino
- La suplementación con fibra sin agua lleva a un empeoramiento del estreñimiento
- Anticolinérgicos o terazosina o doxazosina
- La sequedad de boca o los problemas de memoria pueden deberse a medicamentos anticolinérgicos. Vigilar el empeoramiento del estreñimiento con los anticolinérgicos
- El mareo y la fatiga debidos a los bloqueadores alfa pueden prevenirse asegurando que los pacientes se hidraten y aumenten la ingesta de sal.
- Evaluar la presencia de problemas neuropsiquiátricos y tratarlos en consecuencia
- Los ISRS pueden asociarse con irritabilidad e ideas suicidas
- Los simpaticomiméticos para el TDAH pueden provocar estrechamiento del cuello vesical y posibles efectos negativos en las tasas de flujo e incluso disuria. La pérdida de peso y el estreñimiento se asocian a los simpaticomiméticos.
- Considerar PTNS o TENS
- Algunos niños tienen miedo a las agujas y la PTNS no es factible
- Algunos niños pueden sobrerreaccionar a la sensación y no tolerar la terapia
- Si es resistente, se puede considerar imipramina si han fracasado los tratamientos
- Puede asociarse con irritabilidad e ideas suicidas
- Puede desenmascarar un trastorno bipolar, especialmente si existe antecedente familiar
- No administrar el medicamento a pacientes con antecedente familiar de defectos de conducción o muerte súbita cardíaca
- El medicamento debe estar bajo el control de un adulto en todo momento
- Si no hay evidencia de residuos posmiccionales elevados, se pueden considerar inyecciones de toxina botulínica A en el detrusor
- Los pacientes con índices de flujo por debajo de 0.3 o residuos elevados >150 cc no deben recibir inyecciones de toxina botulínica A debido a la posibilidad de retención/CIC
- Si todo lo demás falla, se puede considerar la neuromodulación sacra
- Complicaciones por desplazamiento del electrodo
Micción disfuncional
Evaluación y diagnóstico
El niño con disfunción miccional contrae habitualmente el esfínter uretral durante la micción. La uroflujometría con EMG es necesaria para confirmar la presencia de contracción del esfínter durante la micción. Tenga en cuenta que el término describe disfunción únicamente durante la fase de vaciamiento. El término disfunción miccional es independiente de la fase de almacenamiento. Es completamente posible que un niño presente disfunción miccional y síntomas de almacenamiento como incontinencia, urgencia o frecuencia, presentando así dos problemas que requieren corrección.
Opciones de tratamiento y sus escollos
- Uroterapia, programa intestinal
- Evitar la diarrea o los accidentes fecales por un uso mal controlado o excesivamente agresivo de agentes osmóticos y catárticos
- Evitar el gas excesivo por sobrecarga de fibra; el gas es tan perjudicial como el estreñimiento y produce distensión del intestino
- La suplementación con fibra sin agua empeora el estreñimiento
- Problemas de conducta, como TDAH y ASS
- Incluso si el niño parece colaborador, puede persistir una actitud de evitación hacia la conducta miccional correcta, sin realizar el esfuerzo real necesario para lograr el resultado.
- Infecciones del tracto urinario
- Repetir uroflujometría y confirmar si el problema persiste
- Si la etiología es disinergia del esfínter externo (ESS)
- Biofeedback
- Micción programada para prevenir la micción infrecuente
- Manejar la sobreactividad del detrusor si está presente. Si la sobreactividad no se controla adecuadamente, los pacientes continuarán con urgencia, lo que anulará el biofeedback realizado.
- Si la etiología es disinergia del esfínter interno (ISS)
- Bloqueadores alfa
- El mareo y la fatiga debidos a los bloqueadores alfa pueden prevenirse asegurando una buena hidratación y aumentando la ingesta de sal.
- Si hay evidencia de ESS, tratar con biofeedback
- Continuar el régimen intestinal
- Manejar la sobreactividad del detrusor si está presente
- Anticolinérgicos o terazosina o doxazosina
- Los problemas de sequedad bucal o de memoria pueden deberse a los medicamentos anticolinérgicos. Vigilar que el estreñimiento no empeore con los anticolinérgicos.
- El mareo y la fatiga debidos a los bloqueadores alfa pueden prevenirse asegurando una buena hidratación y aumentando la ingesta de sal.
- Anticolinérgicos o terazosina o doxazosina
- Bloqueadores alfa
Uretritis bulbar/Uretrorragia
Evaluación y diagnóstico
El dolor asociado a la micción se observa comúnmente en pacientes con alguna forma de micción disinérgica. En pacientes con uretritis bulbar (síndrome de disuria/uretrorragia), el dolor en la punta o a lo largo del cuerpo del pene es más probable que se deba a micción disinérgica. La corrección del patrón miccional eliminó los síntomas.33 En niñas, el dolor vaginal o uretral también puede indicar un patrón anormal.
Vejiga hipoactiva
Evaluación y diagnóstico
La antigua entidad “vejiga perezosa” ha sido reemplazada por el término neutral vejiga hipoactiva y se reserva para los niños con baja frecuencia miccional y necesidad de aumentar la presión intraabdominal para iniciar, mantener o completar la micción (es decir, pujar). Los niños a menudo presentan un patrón interrumpido en la uroflujometría. El diagnóstico formal se confirma mediante estudios urodinámicos que demuestran presiones miccionales bajas. Desafortunadamente, no existen definiciones formales de las presiones miccionales normales en niños, por lo que tendemos a usar las presiones de los adultos.
Opciones de tratamiento y escollos
- Las evaluaciones incluirán una uroflujometría con EMG del suelo pélvico y, si es posible, un segundo EMG de los músculos abdominales.
- Si el pujo abdominal es evidente con un flujo débil e ineficiente (índice de flujo <0.7) y residuo posmiccional elevado, considere el diagnóstico de UAB.
- Confirme con urodinamia
- Inicie uroterapia
- Considere bloqueadores alfa para ayudar a abrir el cuello vesical y mejorar el vaciamiento
- Hasta el 50% de los pacientes también presentan OAB y necesitan tratamiento de la OAB para prevenir la incontinencia o las ITU recurrentes
- ISS se observa comúnmente en pacientes con UAB y el tratamiento con bloqueadores alfa es necesario en estos pacientes.
- Considere CIC si los pacientes tienen PVR elevado y/o ITU recurrentes; algunos han utilizado la neuromodulación sacra pero con éxito limitado
Polaquiuria
Evaluación y diagnóstico
Este término se aplica a los niños que miccionan con frecuencia y con volúmenes pequeños únicamente durante el día. La frecuencia miccional diurna es de al menos una vez por hora y los volúmenes miccionales promedio son inferiores al 50% de la capacidad vesical estimada (EBC), por lo general mucho menores. La incontinencia no es un componente habitual ni necesario de esta afección y el comportamiento vesical nocturno es normal para la edad del niño. El término es aplicable a partir de la edad de control vesical diurno o a partir de los 3 años.
Opciones de tratamiento y escollos
- Evaluar el entorno, se observa comúnmente cuando ha ocurrido un acontecimiento vital reciente o hay un evento próximo como el inicio de la escuela, un campamento o unas vacaciones
- Asegurarse de que no haya estreñimiento nuevo ni cambios en la dieta
- Iniciar uroterapia, programa intestinal
- Evitar la diarrea o los accidentes fecales por uso mal controlado o excesivamente agresivo de agentes osmóticos y catárticos
- Evitar el gas excesivo por sobrecarga de fibra; el gas es tan perjudicial como el estreñimiento y produce distensión del intestino
- La suplementación con fibra sin agua conduce al empeoramiento del estreñimiento
- Considerar anticolinérgicos o terazosina o doxazosina
- La boca seca o los problemas de memoria pueden deberse a los fármacos anticolinérgicos. Vigilar que el estreñimiento no empeore con los anticolinérgicos
- El mareo y la fatiga debidos a los alfabloqueantes pueden prevenirse asegurando que los pacientes se hidraten bien y aumenten la ingesta de sal.
- Evaluar problemas neuropsiquiátricos; si están presentes, considerar tratarlos en consecuencia
- Los ISRS pueden asociarse con irritabilidad e ideas suicidas
- Los simpaticomiméticos para el TDAH pueden provocar un aumento del tono del cuello vesical con posibles efectos negativos en las tasas de flujo e incluso disuria. La pérdida de peso y el estreñimiento se asocian con los simpaticomiméticos.
- Puede resolverse espontáneamente
Incontinencia por la risa
Evaluación y diagnóstico
La incontinencia por risa se asocia con una micción completa que ocurre específicamente durante o inmediatamente después de reír. La función vesical es normal cuando el niño no se ríe. La incontinencia por risa es claramente diferente de la incontinencia de esfuerzo, en la que la micción puede prevenirse o detenerse de forma voluntaria.
Opciones terapéuticas y escollos
- Confirmar el diagnóstico con una buena historia clínica
- Se observa comúnmente en niños con trastornos neuropsiquiátricos subyacentes
- Uroterapia y régimen intestinal para asegurarse de que esto no sea OAB simple
- Si no hay respuesta, entonces iniciar terapia
- Imipramina: Iniciar la dosificación en 10 mg e incrementar hasta un máximo de 75 mg
- Atomoxetina: Iniciar la dosificación en 10 mg e incrementar según corresponda
- Simpaticomiméticos: la dosificación depende del medicamento elegido, debe ser una versión de acción prolongada, de lo contrario, el paciente corre riesgo de accidentes cuando el efecto del medicamento desaparece
- ISRS: la dosificación depende del medicamento, elija la dosis más baja y escale gradualmente.
- Todos los anteriores conllevan los mismos problemas
- pueden asociarse con irritabilidad e ideas suicidas
- pueden desenmascarar un trastorno bipolar si hay antecedentes familiares
- no administrar el medicamento a pacientes con antecedentes familiares de trastornos de la conducción o muerte súbita cardíaca
- El medicamento debe estar bajo el control de un adulto en todo momento
Micción vaginal
Evaluación y diagnóstico
Las niñas prepuberales con control de esfínteres que mojan su ropa interior dentro de los 10 minutos posteriores a la micción probablemente estén experimentando reflujo vaginal si no es evidente ningún mecanismo subyacente distinto del atrapamiento vaginal de orina. La micción vaginal no se asocia con otros síntomas del tracto urinario inferior. Es esencial diferenciar la micción vaginal del goteo posmiccional, ya que el tratamiento es bastante diferente.
Opciones de tratamiento y escollos
- Confirmar el diagnóstico y diferenciarlo del goteo posmiccional, la incontinencia de esfuerzo y la incontinencia de urgencia
- Comúnmente se observa en niñas pequeñas que no se bajan la ropa por debajo de la rodilla
- Comúnmente se observa en niñas que tienen grasa labial prominente
- Comúnmente se observa en niñas que son obesas
- Recomiende que las pacientes se sienten en el inodoro con las piernas separadas y los muslos separados, o que se sienten mirando hacia la pared detrás del inodoro, lo que obliga a mantener las piernas separadas
- Con frecuencia se asocia con secreción vaginal y vaginitis
- Puede asociarse con liquen escleroso de los labios
Incontinencia de esfuerzo
Evaluación y diagnóstico
La incontinencia urinaria de esfuerzo es la pérdida de pequeñas cantidades de orina con el esfuerzo o con el aumento de la presión intraabdominal, típicamente asociada con la maniobra de Valsalva. Es rara en los niños neurológicamente normales. Existe una mayor asociación con niñas hiperflexibles involucradas en la gimnasia y la danza.105
Opciones de tratamiento y escollos
- Confirmar el diagnóstico y diferenciarlo del goteo posmiccional, la incontinencia de esfuerzo y de urgencia
- Corrección quirúrgica con Burch abierta o laparoscópica106,107
Puntos clave
Conclusiones
asdf
Referencias
- Ruarte AC, E Q. Urodynamic Evaluation in Normal Children. J Urol 1987; 127 (4): 831–831. DOI: 10.1016/s0022-5347(17)54062-8.
- Landgraf JM, Abidari J, Cilento BG, Cooper CS, Schulman SL, Ortenberg J. Coping, Commitment, and Attitude: Quantifying the Everyday Burden of Enuresis on Children and Their Families. Pediatrics 2004; 113 (2): 334–344. DOI: 10.1542/peds.113.2.334.
- Rovner ES. Childhood Urinary Symptoms Predict Adult Overactive Bladder Symptoms. Yearbook of Urology 2006; 2007: 65–66. DOI: 10.1016/s0084-4071(08)70046-0.
- Minassian VA, Lovatsis D, Pascali D, Alarab M, Drutz HP. The Effect of Childhood Dysfunctional Voiding on Urinary Incontinence in Adult Women. Obstet Gynecol 2006; 107 (Supplement): 47s. DOI: 10.1097/00006250-200604001-00112.
- Labrie J, Jong TPVM de, Nieuwhof-Leppink A, Deure J van der, Vijverberg MAW, Vaart CH van der. The Relationship Between Children With Voiding Problems and Their Parents. J Urol 2010; 183 (5): 1887–1891. DOI: 10.1016/j.juro.2010.01.004.
- Wennberg A-L, Altman D, Lundholm C, Klint Å, Iliadou A, Peeker R, et al.. Genetic Influences Are Important for Most But Not All Lower Urinary Tract Symptoms: A Population-Based Survey in a Cohort of Adult Swedish Twins. Eur Urol 2011; 59 (6): 1032–1038. DOI: 10.1016/j.eururo.2011.03.007.
- Kaplan SA. Re: Systematic Review and Meta-Analysis of Candidate Gene Association Studies of Lower Urinary Tract Symptoms in Men. J Urol 2014; 195 (6): 1839–1840. DOI: 10.1016/j.juro.2016.03.051.
- Botlero R, Bell RJ, Urquhart DM, Davis SR. Urinary incontinence is associated with lower psychological general well-being in community-dwelling women. Menopause 2010; 17 (2): 332–337. DOI: 10.1097/gme.0b013e3181ba571a.
- Melville JL, Fan M-Y, Rau H, Nygaard IE, Katon WJ. Major depression and urinary incontinence in women: temporal associations in an epidemiologic sample. Am J Obstet Gynecol 2009; 201 (5): 490.e1–490.e7. DOI: 10.1016/j.ajog.2009.05.047.
- Henin A, Biederman J, Mick E, Hirshfeld-Becker DR, Sachs GS, Wu Y, et al.. Childhood antecedent disorders to bipolar disorder in adults: A controlled study. J Affect Disord 2007; 99 (1-3): 51–57. DOI: 10.1016/j.jad.2006.09.001.
- Weissman MM, Gross R, Fyer A, Heiman GA, Gameroff MJ, Hodge SE, et al.. Interstitial Cystitis and Panic Disorder. Arch Gen Psychiatry 2004; 61 (3): 273. DOI: 10.1001/archpsyc.61.3.273.
- Stockman JA. Enuresis as a premorbid developmental marker of schizophrenia. Yearbook of Pediatrics 2008; 2010: 396–398. DOI: 10.1016/s0084-3954(09)79524-7.
- Fowler CJ, Griffiths DJ. A decade of functional brain imaging applied to bladder control. Neurourol Urodyn 2010; 29 (1): 49–55. DOI: 10.1002/nau.20740.
- Fowler CJ, Griffiths D, Groat WC de. The neural control of micturition. Nat Rev Neurosci 2008; 9 (6): 453–466. DOI: 10.1038/nrn2401.
- Hansen A, Hansen B, Dahm TL. Urinary tract infection, day wetting and other voiding symptoms in seven-to eight-year-old Danish children. Acta Paediatr 1997; 86 (12): 1345–1349. DOI: 10.1111/j.1651-2227.1997.tb14911.x.
- Hellström A-L, Hanson E, Hansson S, Hjälmås K, Jodal U. Micturition habits and incontinence in 7-year-old Swedish school entrants. Eur J Pediatr 1990; 149 (6): 434–437. DOI: 10.1007/bf02009667.
- Lee SD, Sohn DW, Lee JZ, Park NC, Chung MK. An epidemiological study of enuresis in Korean children. BJU Int 2000; 85 (7): 869–873. DOI: 10.1046/j.1464-410x.2000.00617.x.
- Safarinejad MR. Prevalence of nocturnal enuresis, risk factors, associated familial factors and urinary pathology among school children in Iran. J Pediatr Urol 2007; 3 (6): 443–452. DOI: 10.1016/j.jpurol.2007.06.001.
- Wekke J Spee-van der, Hirasing RA, Meulmeester JF, Radder JJ. Childhood Nocturnal Enuresis in the Netherlands. Urology 1998; 51 (6): 1022–1026. DOI: 10.1016/s0090-4295(98)00106-x.
- Swithinbank LV, Brookes ST, Shepherd AM, Abrams P. The natural history of urinary symptoms during adolescence. BJU Int 1998; 81 (s3): 90–93. DOI: 10.1046/j.1464-410x.1998.00016.x.
- Deshpande AV, Craig JC, Smith GHH, Caldwell PHY. Management of daytime urinary incontinence and lower urinary tract symptoms in children. J Paediatr Child Health 2003; 48 (2): E44–e52. DOI: 10.1111/j.1440-1754.2011.02216.x.
- Heron J, Joinson C, Croudace T, Gontard A von. Trajectories of Daytime Wetting and Soiling in a United Kingdom 4 to 9-Year-Old Population Birth Cohort Study. J Urol 2008; 179 (5): 1970–1975. DOI: 10.1016/j.juro.2008.01.060.
- Stone JJ, Rozzelle CJ, Greenfield SP. Intractable Voiding Dysfunction in Children With Normal Spinal Imaging: Predictors of Failed Conservative Management. Urology 2010; 75 (1): 161–165. DOI: 10.1016/j.urology.2009.06.100.
- Tekgul S, R. N, Hoebeke P, Canning D, Bower W, Gontard A. Incontinence. 2009: 701–792.
- Gontard A, Nevéus T. Management of disorders of bladder and bowel control in childhood. 2006. DOI: 10.1136/adc.2006.110023.
- Gontard A, Hussong J, Yang SS, Chase J, Franco I, Wright A. Neurodevelopmental disorders and incontinence in children and adolescents: Attention-deficit/hyperactivity disorder, autism spectrum disorder, and intellectual disability–A consensus document of the International Children’s Continence Society. Neurourol Urodyn 2021; 41 (1): 102–114. DOI: 10.1002/nau.24798.
- Joinson C, Heron J, Butler U, Gontard A von, Parents the Avon Longitudinal Study of, Team CS. Psychological Differences Between Children With and Without Soiling Problems. Pediatrics 2006; 117 (5): 1575–1584. DOI: 10.1542/peds.2005-1773.
- Joinson C, Heron J, Gontard A von, Butler U, Golding J, Emond A. Early Childhood Risk Factors Associated with Daytime Wetting and Soiling in School-age Children. J Pediatr Psychol 2008; 33 (7): 739–750. DOI: 10.1093/jpepsy/jsn008.
- Sureshkumar P, Jones M, Cumming R, Craig J. A Population Based Study of 2,856 School-Age Children With Urinary Incontinence. J Urol 2009; 181 (2): 808–816. DOI: 10.1016/j.juro.2008.10.044.
- ROBSON WMLANEM, JACKSON HAROLDP, BLACKHURST DAWN, LEUNG ALEXANDERk. C. Enuresis in Children With Attention–Deficit Hyperactivity Disorder. South Med J 1997; 90 (5): 503–505. DOI: 10.1097/00007611-199705000-00007.
- MOORE KATEH, SUTHERST JR. Response to Treatment of Detrusor Instability in Relation to Psychoneurotic Status. Br J Urol 1990; 66 (5): 486–490. DOI: 10.1111/j.1464-410x.1990.tb14993.x.
- WARNE STEPHANIEA, GODLEY MARGARETL, WILCOX DUNCANT. Surgical Reconstruction Of Cloacal Malformation Can Alter Bladder Function: A Comparative Study With Anorectal Anomalies. J Urol 2381; 172 (6 Part 1): 2377–2381. DOI: 10.1097/01.ju.0000145201.94571.67.
- Coplen DE. Dysfunctional Elimination Syndrome as an Etiology of Idiopathic Urethritis in Childhood. Yearbook of Urology 2005; 2006: 257–258. DOI: 10.1016/s0084-4071(08)70411-1.
- Pezzone MA, Liang R, Fraser MO. A Model of Neural Cross-Talk and Irritation in the Pelvis: Implications for the Overlap of Chronic Pelvic Pain Disorders. Gastroenterology 2005; 128 (7): 1953–1964. DOI: 10.1053/j.gastro.2005.03.008.
- Ustinova EE, Fraser MO, Pezzone MA. Colonic irritation in the rat sensitizes urinary bladder afferents to mechanical and chemical stimuli: an afferent origin of pelvic organ cross-sensitization. Am J Physiol Renal Physiol 2006; 290 (6): F1478–f1487. DOI: 10.1152/ajprenal.00395.2005.
- Franco I, Grantham EC, Cubillos J, Franco J, Collett-Gardere T, Zelkovic P. Can a simple question predict prolonged uroflow lag times in children? J Pediatr Urol 2016; 12 (3): 157.e1–157.e8. DOI: 10.1016/j.jpurol.2015.12.009.
- Lewis SJ, Heaton KW. Stool Form Scale as a Useful Guide to Intestinal Transit Time. Scand J Gastroenterol 1997; 32 (9): 920–924. DOI: 10.3109/00365529709011203.
- FARHAT WALID, B??GLI DARIUSJ, CAPOLICCHIO GIANPAOLO, O???REILLY SHEILA, MERGUERIAN PAULA, KHOURY ANTOINE, et al.. The Dysfunctional Voiding Scoring System: Quantitative Standardization Of Dysfunctional Voiding Symptoms In Children. J Urol 2000; 164: 1011–1015. DOI: 10.1097/00005392-200009020-00023.
- Afshar K, Mirbagheri A, Scott H, MacNeily AE. Development of a Symptom Score for Dysfunctional Elimination Syndrome. J Urol 2009; 182 (4s): 1939–1944. DOI: 10.1016/j.juro.2009.03.009.
- Van Hoecke E, Baeyens D, Vanden Bossche H, Hoebeke P, Vande Walle J. Early Detection of Psychological Problems in a Population of Children With Enuresis: Construction and Validation of the Short Screening Instrument for Psychological Problems in Enuresis. J Urol 2007; 178 (6): 2611–2615. DOI: 10.1016/j.juro.2007.08.025.
- Franco I, Shei-Dei Yang S, Chang S-J, Nussenblatt B, Franco JA. A quantitative approach to the interpretation of uroflowmetry in children. Neurourol Urodyn 2016; 35 (7): 836–846. DOI: 10.1002/nau.22813.
- Franco I, Franco JA, Nussenblatt B. Can the idealized voider derived flow indexes be a measure of voiding efficiency and how accurate are they? Neurourol Urodyn 2018; 37 (6): 1913–1924. DOI: 10.1002/nau.23585.
- Franco I, Franco J, Lee YS, Choi EK, Han SW. Can a quantitative means be used to predict flow patterns: Agreement between visual inspection vs. flow index derived flow patterns. J Pediatr Urol 2016; 12 (4): 218.e1–218.e8. DOI: 10.1016/j.jpurol.2016.05.026.
- COMBS ANDREWJ, GRAFSTEIN NEIL, HOROWITZ MARK, GLASSBERG KENNETHI. Primary Bladder Neck Dysfunction In Children And Adolescents I: Pelvic Floor Electromyography Lag Time–a New Noninvasive Method To Screen For And Monitor Therapeutic Response. J Urol 2005; 173 (1): 207–211. DOI: 10.1097/01.ju.0000147269.93699.5a.
- Tuite GF, Thompson DNP, Austin PF, Bauer SB. Evaluation and management of tethered cord syndrome in occult spinal dysraphism: Recommendations from the international children’s continence society. Neurourol Urodyn 2018; 37 (3): 890–903. DOI: 10.1002/nau.23382.
- Coplen DE. The Relevance of Urodynamic Studies for Urge Syndrome and Dysfunctional Voiding: A Multicenter Controlled Trial in Children. Yearbook of Urology 2008; 2009: 83–84. DOI: 10.1016/s0084-4071(09)79276-0.
- Birder LA. Faculty Opinions recommendation of Treatment of daytime urinary incontinence: A standardization document from the International Children’s Continence Society. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2017; 36: 43–50, DOI: 10.3410/f.725854188.793540473.
- Yang S, Chua ME, Bauer S, Wright A, Brandström P, Hoebeke P, et al.. Diagnosis and management of bladder bowel dysfunction in children with urinary tract infections: a position statement from the International Children’s Continence Society. Pediatr Nephrol 2018; 33 (12): 2207–2219. DOI: 10.1007/s00467-017-3799-9.
- Gontard A von, Kuwertz-Bröking E. The Diagnosis and Treatment of Enuresis and Functional Daytime Urinary Incontinence. Dtsch Arztebl Int 2019; 116: 279–285, DOI: 10.3238/arztebl.2019.0279.
- MacNeily AE. Should Psychological Assessment be a Part of Incontinence Management in Children and Adolescents? J Urol 2016; 195 (5): 1327–1328. DOI: 10.1016/j.juro.2016.02.071.
- Nieuwhof-Leppink AJ, Hussong J, Chase J, Larsson J, Renson C, Hoebeke P, et al.. Definitions, indications and practice of urotherapy in children and adolescents: - A standardization document of the International Children’s Continence Society (ICCS). J Pediatr Urol 2021; 17 (2): 172–181. DOI: 10.1016/j.jpurol.2020.11.006.
- Borch L, Hagstroem S, Bower WF, Siggaard Rittig C, Rittig S. Bladder and bowel dysfunction and the resolution of urinary incontinence with successful management of bowel symptoms in children. Acta Paediatr 2013; 102 (5): e215–e220. DOI: 10.1111/apa.12158.
- Hagstroem S, Mahler B, Madsen B, Djurhuus JC, Rittig S. Transcutaneous Electrical Nerve Stimulation for Refractory Daytime Urinary Urge Incontinence. J Urol 2009; 182 (4s): 2072–2078. DOI: 10.1016/j.juro.2009.05.101.
- Niemczyk J, Equit M, Hoffmann L, Gontard A von. Incontinence in children with treated attention-deficit/hyperactivity disorder. J Pediatr Urol 2015; 11 (3): 141.e1–141.e6. DOI: 10.1016/j.jpurol.2015.02.009.
- Schäfer SK, Niemczyk J, Gontard A von, Pospeschill M, Becker N, Equit M. Standard urotherapy as first-line intervention for daytime incontinence: a meta-analysis. Eur Child Adolesc Psychiatry 2018; 27 (8): 949–964. DOI: 10.1007/s00787-017-1051-6.
- Medina-Centeno R. Medications for constipation in 2020. Curr Opin Pediatr 2020; 32 (5): 668–673. DOI: 10.1097/mop.0000000000000938.
- Wald A. Constipation. Jama 2016; 315 (2): 185. DOI: 10.1001/jama.2015.16994.
- Cruz F. Faculty of 1000 evaluation for Randomized, double-blind, placebo-controlled trial of polyethylene glycol (MiraLAX(®)) for urinary urge symptoms. F1000 - Post-Publication Peer Review of the Biomedical Literature 2013; 9: 597–604, DOI: 10.3410/f.717964565.793474432.
- Loening-Baucke V. Urinary Incontinence and Urinary Tract Infection and Their Resolution With Treatment of Chronic Constipation of Childhood. Pediatrics 1997; 100 (2): 228–232. DOI: 10.1542/peds.100.2.228.
- Finney SM, Andersson KE, Gillespie JI, Stewart LH. Faculty Opinions recommendation of Antimuscarinic drugs in detrusor overactivity and the overactive bladder syndrome: motor or sensory actions? Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2006; 98: 503–507, DOI: 10.3410/f.1040721.489750.
- Andersson K-E. Antimuscarinic Mechanisms and the Overactive Detrusor: An Update. Eur Urol 2011; 59 (3): 377–386. DOI: 10.1016/j.eururo.2010.11.040.
- Wein AJ, Rackley RR. Overactive Bladder: A Better Understanding of Pathophysiology, Diagnosis and Management. J Urol 2006; 175 (3s): 5–10, DOI: 10.1016/s0022-5347(05)00313-7.
- Kullmann FA, Artim DE, Birder LA, Groat WC de. Activation of Muscarinic Receptors in Rat Bladder Sensory Pathways Alters Reflex Bladder Activity. J Neurosci 2008; 28 (8): 1977–1987. DOI: 10.1523/jneurosci.4694-07.2008.
- Andersson K. Step-by-Step Guide to Treatment of Overactive Bladder (OAB)/Detrusor Overactivity. Urogynecology: Evidence-Based Clinical Practice 2004; 2: 77–91. DOI: 10.1007/1-84628-165-2_7.
- Ferrara P, D’Aleo CM, Tarquini E, Salvatore S, Salvaggio E. Side-effects of oral or intravesical oxybutynin chloride in children with spina bifida. BJU Int 2001; 87 (7): 674–678. DOI: 10.1046/j.1464-410x.2001.02152.x.
- SOMMER BARBARAR, O’HARA RUTH, ASKARI NUSHA, KRAEMER HELENAC, KENNEDY WILLIAMA. The Effect Of Oxybutynin Treatment On Cognition In Children With Diurnal Incontinence. J Urol 2AD; 173 (6): 2125–2127. DOI: 10.1097/01.ju.0000157685.83573.79.
- Giramonti KM, Kogan BA, Halpern LF. The effects of anticholinergic drugs on attention span and short-term memory skills in children. Neurourol Urodyn 2008; 27 (4): 315–318. DOI: 10.1002/nau.20507.
- Todorova A, Vonderheid-Guth B, Dimpfel W. Effects of Tolterodine, Trospium Chloride, and Oxybutynin on the Central Nervous System. J Clin Pharmacol 2001; 41 (6): 636–644. DOI: 10.1177/00912700122010528.
- GUPTA S, SATHYAN G, LINDEMULDER E, HO P, SHEINER L, AARONS L. Quantitative characterization of therapeutic index: Application of mixed-effects modeling to evaluate oxybutynin dose–efficacy and dose–side effect relationships. Clin Pharmacol Ther 1999; 65 (6): 672–684. DOI: 10.1016/s0009-9236(99)90089-9.
- AUSTIN PAULF, HOMSY YVESL, MASEL JONATHANL, CAIN MARKP, CASALE ANTHONYJ, RINK RICHARDC. alpha-ADRENERGIC BLOCKADE IN CHILDREN WITH NEUROPATHIC AND NONNEUROPATHIC VOIDING DYSFUNCTION. J Urol 1999; 162: 1064–1067. DOI: 10.1097/00005392-199909000-00029.
- Franco I, S. C, Collett T, Reda E. Unknown. American Academy of Pediatrics Meeting. San Francisco, CA: 2007.
- Dellis AE, Keeley FX, Manolas V, Skolarikos AA. Role of \ensuremathα-blockers in the Treatment of Stent-related Symptoms: A Prospective Randomized Control Study. Urology 2014; 83 (1): 56–62. DOI: 10.1016/j.urology.2013.08.067.
- Lepor H, Kaplan SA, Klimberg I, Mobley DF, Fawzy A, Gaffney M, et al.. Doxazosin for Benign Prostatic Hyperplasia: Long-term Efficacy and Safety in Hypertensive and Normotensive Patients. J Urol 1997; 157 (2): 525–530. DOI: 10.1016/s0022-5347(01)65193-0.
- Chakraborty S, Feuerhak K, Muthyala A, Harmsen WS, Bailey KR, Bharucha AE. Effects of Alfuzosin, an \ensuremathα1-Adrenergic Antagonist, on Anal Pressures and Bowel Habits in Women With and Without Defecatory Disorders. Clin Gastroenterol Hepatol 2019; 17 (6): 1138–1147.e3. DOI: 10.1016/j.cgh.2018.08.036.
- VanderBrink BA, Gitlin J, Toro S, Palmer LS. Effect of Tamsulosin on Systemic Blood Pressure and Nonneurogenic Dysfunctional Voiding in Children. J Urol 2009; 181 (2): 817–822. DOI: 10.1016/j.juro.2008.10.045.
- Andersson K. Ch. 8. Incontinence 2009.
- Uchida H, Shishido K, Nomiya M, Yamaguchi O. Involvement of cyclic AMP-dependent and -independent mechanisms in the relaxation of rat detrusor muscle via \ensuremathβ-adrenoceptors. Eur J Pharmacol 2005; 518 (2-3): 195–202. DOI: 10.1016/j.ejphar.2005.06.029.
- Frazier EP, Mathy M-J, Peters SLM, Michel MC. Does Cyclic AMP Mediate Rat Urinary Bladder Relaxation by Isoproterenol? J Pharmacol Exp Ther 2005; 313 (1): 260–267. DOI: 10.1124/jpet.104.077768.
- Kobayashi H, Adachi-Akahane S, Nagao T. Involvement of BKCa channels in the relaxation of detrusor muscle via \ensuremathβ-adrenoceptors. Eur J Pharmacol 2000; 404 (1-2): 231–238. DOI: 10.1016/s0014-2999(00)00606-3.
- Hunsballe JM, Djurhuus JC. Clinical options for imipramine in the management of urinary incontinence. Urol Res 2001; 29 (2): 118–125. DOI: 10.1007/s002400100175.
- Franco I, Arlen AM, Collett-Gardere T, Zelkovic PF. Imipramine for refractory daytime incontinence in the pediatric population. J Pediatr Urol 2018; 14 (1): 58.e1–58.e5. DOI: 10.1016/j.jpurol.2017.08.016.
- Groat WC de, Griffiths D, Yoshimura N. Neural Control of the Lower Urinary Tract. Compr Physiol 2015; 5: 327–396. DOI: 10.1002/cphy.c130056.
- Numata A, Iwata T, Iuchi H, Taniguchi N, Kita M, Wada N, et al.. Micturition-suppressing region in the periaqueductal gray of the mesencephalon of the cat. Am J Physiol Regul Integr Comp Physiol 2008; 294 (6): R1996–r2000. DOI: 10.1152/ajpregu.00393.2006.
- Schuessler B. What do we know about duloxetine’s mode of action? Evidence from animals to humans. Bjog 2006; 113: 5–9. DOI: 10.1111/j.1471-0528.2006.00877.x.
- Roth TJ, Vandersteen DR, Hollatz P, Inman BA, Reinberg YE. Sacral Neuromodulation for the Dysfunctional Elimination Syndrome: A 10-Year Single-center Experience With 105 Consecutive Children. Urology 2008; 84 (4): 911–918. DOI: 10.1016/j.urology.2014.03.059.
- Boswell TC, Hollatz P, Hutcheson JC, Vandersteen DR, Reinberg YE. Device outcomes in pediatric sacral neuromodulation: A single center series of 187 patients. J Pediatr Urol 2021; 17 (1): 72.e1–72.e7. DOI: 10.1016/j.jpurol.2020.10.010.
- BOWER WF, MOORE KH, ADAMS RD. A Pilot Study Of The Home Application Of Transcutaneous Neuromodulation In Children With Urgency Or Urge Incontinence. J Urol 2001; 166: 2420–2422. DOI: 10.1097/00005392-200112000-00112.
- Lordelo P, Teles A, Veiga ML, Correia LC, Barroso U Jr. Faculty Opinions recommendation of Transcutaneous electrical nerve stimulation in children with overactive bladder: a randomized clinical trial. Faculty Opinions – Post-Publication Peer Review of the Biomedical Literature 2010; 184: 683–689, DOI: 10.3410/f.4324972.4410069.
- HOEBEKE P, RENSON C, PETILLON L, WALLE JVANDE, DE PAEPE H. Percutaneous Electrical Nerve Stimulation in Children With Therapy Resistant Nonneuropathic Bladder Sphincter Dysfunction: A Pilot Study. J Urol 2002; 168: 2605–2608. DOI: 10.1097/00005392-200212000-00085.
- CHASE JANET, ROBERTSON VALJ, SOUTHWELL BRIDGET, HUTSON JOHN, GIBB SUSIE. Pilot study using transcutaneous electrical stimulation (interferential current) to treat chronic treatment-resistant constipation and soiling in children. J Gastroenterol Hepatol 2005; 20 (7): 1054–1061. DOI: 10.1111/j.1440-1746.2005.03863.x.
- BALKEN MICHAELR van, VERGUNST HENK, BEMELMANS BARTLH. The Use Of Electrical Devices For The Treatment Of Bladder Dysfunction: A Review Of Methods. J Urol 2004; 172 (3): 846–851. DOI: 10.1097/01.ju.0000134418.21959.98.
- Capitanucci ML, Camanni D, Demelas F, Mosiello G, Zaccara A, De Gennaro M. Long-Term Efficacy of Percutaneous Tibial Nerve Stimulation for Different Types of Lower Urinary Tract Dysfunction in Children. J Urol 2009; 182 (4s): 2056–2061. DOI: 10.1016/j.juro.2009.03.007.
- Barroso U, Viterbo W, Bittencourt J, Farias T, Lordêlo P. Posterior Tibial Nerve Stimulation vs Parasacral Transcutaneous Neuromodulation for Overactive Bladder in Children. J Urol 2013; 190 (2): 673–677. DOI: 10.1016/j.juro.2013.02.034.
- Jafarov R, Ceyhan E, Kahraman O, Ceylan T, Dikmen ZG, Tekgul S, et al.. Efficacy of transcutaneous posterior tibial nerve stimulation in children with functional voiding disorders. Neurourol Urodyn 2021; 40 (1): 404–411. DOI: 10.1002/nau.24575.
- Austin PF, Franco I, Dobremez E, Kroll P, Titanji W, Geib T, et al.. OnabotulinumtoxinA for the treatment of neurogenic detrusor overactivity in children. Neurourol Urodyn 2021; 40 (1): 493–501. DOI: 10.1002/nau.24588.
- Hoebeke P, De Caestecker K, Vande Walle J, Dehoorne J, Raes A, Verleyen P, et al.. The Effect of Botulinum-A Toxin in Incontinent Children With Therapy Resistant Overactive Detrusor. J Urol 2006; 176 (1): 328–331. DOI: 10.1016/s0022-5347(06)00301-6.
- Lahdes-Vasama TT, Anttila A, Wahl E, Taskinen S. Urodynamic assessment of children treated with botulinum toxin A injections for urge incontinence: a pilot study. Scand J Urol Nephrol 2011; 45 (6): 397–400. DOI: 10.3109/00365599.2011.590997.
- Marte A, Borrelli M, Sabatino MD, Balzo BD, Prezioso M, Pintozzi L, et al.. Effectiveness of Botulinum-A Toxin for the Treatment of Refractory Overactive Bladder in Children. Eur J Pediatr Surg 2010; 20 (03): 153–157. DOI: 10.1055/s-0029-1246193.
- Chase J, Austin P, Hoebeke P, McKenna P, International Children’s Continence S. The Management of Dysfunctional Voiding in Children: A Report From the Standardisation Committee of the International Children’s Continence Society. J Urol 2010; 183 (4): 1296–1302. DOI: 10.1016/j.juro.2009.12.059.
- Clothier JC, Wright AJ. Dysfunctional voiding: the importance of non-invasive urodynamics in diagnosis and treatment. Pediatr Nephrol 2018; 33 (3): 381–394. DOI: 10.1007/s00467-017-3679-3.
- PALMER LANES, FRANCO ISRAEL, ROTARIO PAUL, REDA EDWARDF, FRIEDMAN STEVENC, KOLLIGIAN MARKE, et al.. Biofeedback Therapy Expedites the Resolution of Reflux In Older Children. J Urol 2002; 168: 1699–1703. DOI: 10.1097/00005392-200210020-00010.
- Resnick NM, Perera S, Tadic S, Organist L, Riley MA, Schaefer W, et al.. What Predicts and what Mediates the response of urge urinary incontinence to biofeedback? Neurourol Urodyn 2013; 32 (5): 408–415. DOI: 10.1002/nau.22347.
- Kibar Y, Demir E, Irkilata C, Ors O, Gok F, Dayanc M. Effect of Biofeedback Treatment on Spinning Top Urethra in Children with Voiding Dysfunction. Urology 2007; 70 (4): 781–784. DOI: 10.1016/j.urology.2007.04.054.
- Kibar Y, Ors O, Demir E, Kalman S, Sakallioglu O, Dayanc M. Results of Biofeedback Treatment on Reflux Resolution Rates in Children with Dysfunctional Voiding and Vesicoureteral Reflux. Urology 2007; 70 (3): 563–566. DOI: 10.1016/j.urology.2007.03.085.
- Bauer SB, Vasquez E, Cendron M, Wakamatsu MM, Chow JS. Pelvic floor laxity: A not so rare but unrecognized form of daytime urinary incontinence in peripubertal and adolescent girls. J Pediatr Urol 2018; 14 (6): 544.e1–544.e7. DOI: 10.1016/j.jpurol.2018.04.030.
- Dobrowolska-Glazar BA, Groen LA, Nieuwhof-Leppink AJ, Klijn AJ, Jong TPVM de, Chrzan R. Open and Laparoscopic Colposuspension in Girls with Refractory Urinary Incontinence. Front Pediatr 2017; 5: 284, DOI: 10.3389/fped.2017.00284.
- Colposuspension in girls: clinical and urodynamic aspects. J Pediatr Urol 2005; 1 (2): 69–74. DOI: 10.1016/j.jpurol.2004.11.011.
Última actualización: 2025-09-21 13:35