
63: 小儿泌尿外科的质量改进
阅读本章大约需要 7 分钟。
引言
1999年,医学研究院在报告可预防错误每年导致近98,000人死亡时,强调了对医疗实践进行自我反思与改进的必要性。这一惊人的发现凸显了评估患者结局并制定策略以改进医疗流程、提供安全、有效且公平的医疗服务的重要性。1 过去几十年里,人们对质量改进(QI)和患者安全的重视不断增加,并已将其纳入医学教育和医院实践。尽管最初的采用进展缓慢,这些质量改进举措在小儿泌尿外科领域正日益普及。本章将简要概述小儿泌尿外科中的各类QI举措及QI方法学。需要注意的是,以下提到的各类QI举措并不全面,许多中心可能还有未在此列出的QI项目。
患者护理中的质量改进举措
睾丸扭转
睾丸扭转是一种儿科泌尿外科急症,每年每10万名男孩中估计有3.8例受影响。在41.9%的病例中,扭转的睾丸不可存活,需行睾丸切除术。2 导致需要行睾丸切除术的因素包括就诊、诊断、转运和手术干预的延误。许多机构已实施QI诊疗路径,以加快对因睾丸扭转就诊患者的评估,希望缩短干预时间。
2012年,达拉斯儿童医疗中心实施了直达手术室(STOR)路径,其中经超声诊断为扭转且由外院转入的病例将绕过急诊室(ER)(图1)。在值班小儿泌尿外科医师与急诊科医师进行医师间沟通后,这些患者被送至围手术期区域接受评估。一旦启动该路径,即动员手术室团队;若经小儿泌尿外科团队复评后提示需要手术,则完成知情同意,并在到院后1小时内将患者送入手术室。STOR路径将到院至切开时间的中位数显著缩短,从94分钟降至54分钟,但仅有46.8%的患者在症状起始后6小时内接受了手术干预。因此,与实施该路径前相比,睾丸丧失率并无显著差异。为实现睾丸保留,仍需进一步改进流程,以减少转运前的缺血时间。3
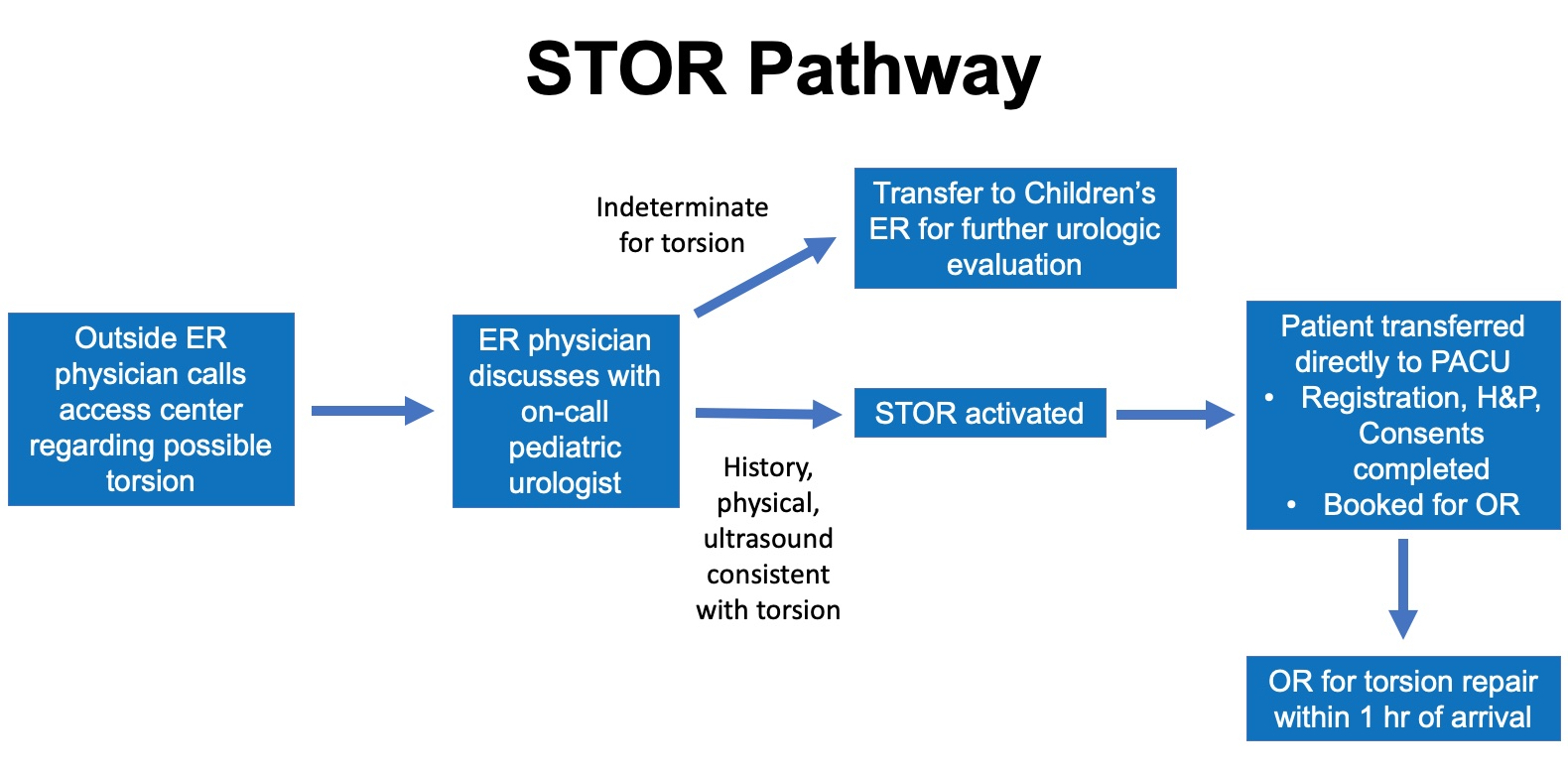
图1 STOR路径。 达拉斯儿童医疗中心用于扭转处理的直达手术室路径示意图。经超声确诊为扭转的病例将直接转运至围手术期区域,为手术干预做准备。通过该路径,将绕过急诊室(ER),以缩短到达手术室的时间。结论不明确的病例将转至急诊室(ER)以进行进一步的泌尿外科评估。 (急诊室 - ER; 麻醉后复苏室 – PACU; 病史与查体 – H&P; 手术室 – OR)
Zee 等人 报告了他们在儿童国家医疗中心急诊室为就诊的睾丸扭转患儿建立加速睾丸扭转救治路径 (ACT) 的经验,以缩短至手术干预的时间。该路径将从急诊分诊到进入手术室的时间中位数由196分钟缩短至127分钟。然而,睾丸切除率并未改变,提示尽管从急诊到手术室的时间缩短,仍需进一步努力以减少睾丸的总缺血时间。4
包括费城儿童医院、科罗拉多儿童医院等在内的许多机构,已为其急诊科医务人员制定了诊疗路径,以指导对以急性阴囊就诊的男孩进行诊断评估。这些路径有助于加快睾丸扭转的诊断。然而,仍需加强公众对睾丸扭转体征和症状的认识,以缩短从症状出现到就医的时间。
术后加速康复
加速康复外科路径提倡对术后护理采取标准化、循证的方法,旨在改善患者在大型手术后的康复过程。这些路径已在成人外科护理中被广泛采用,并已被证明可减少术后住院时间、并发症发生率和成本。5,6 相比之下,ERAS在小儿外科的实施较为缓慢,因为其在儿童中的疗效尚未得到充分研究。人们认为对于总体发病率和死亡率较低的小儿手术,ERAS带来的获益有限,这一看法也减缓了标准化小儿ERAS方案的制定与采用。7 在过去十年里,这种观点正在改变,ERAS在儿童中的实施有所增加,人们希望藉此改善其在大型手术后的术后康复。8,9 一项针对小儿泌尿外科医师的ERAS调查显示,54%的人报告在术后护理中实施了不同的ERAS要素,但仅有20%的人表示其所在机构有既定方案。10
在小儿泌尿外科中,多个机构已实施 ERAS 路径,以改善接受膀胱重建(包括膀胱扩大术、膀胱颈重建术或建立可导尿通道)的儿童的术后恢复。Rove 等 报告了他们在 Children’s Hospital Colorado 实施 ERAS 的经验,指出相比历史非 ERAS 队列,术后住院时长从 8 天降至 5.7 天;他们还报告 ERAS 组并发症风险降低 30%(OR 0.71,95% CI 0.51–0.97)。11 类似地,Chu 等 也指出,在 Lurie Children’s Hospital 实施 ERAS 后,接受膀胱重建的儿童住院时长的中位数由 9 天降至 4 天,但并未观察到并发症发生率的显著变化。12 这些研究提示,ERAS 可能有益于接受重大膀胱重建的儿童。一项涉及全美 8 个以上中心的多中心试验(P儿科 U泌尿学 R康复 后 Su手术 E项目)正在进行,旨在评估 ERAS 在接受膀胱重建的儿童中的疗效。该试验的结果将有助于确定哪些具体 ERAS 要素至关重要,并帮助为该患儿人群完善未来的 ERAS 路径。13 ERAS 要素列表见图2。
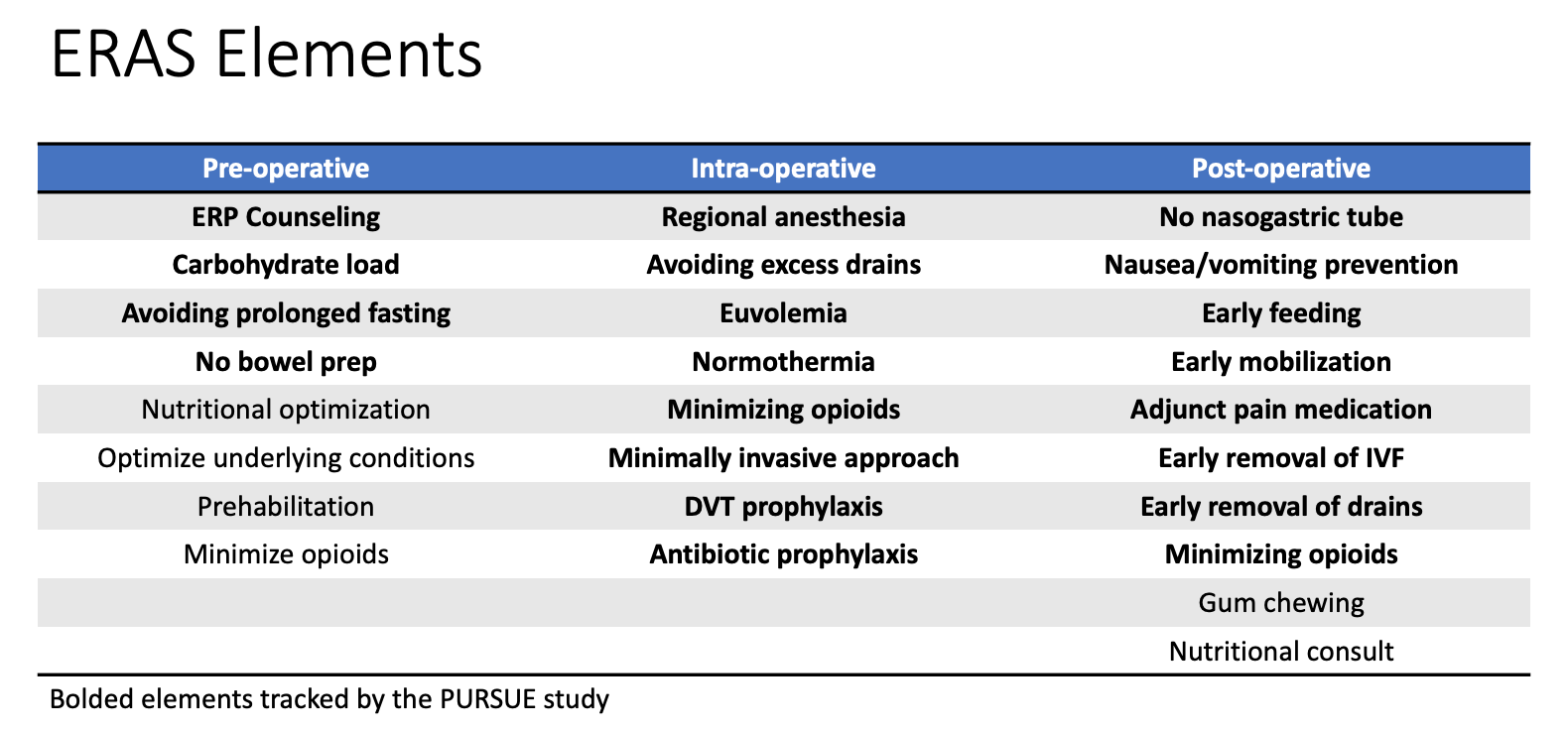
图 2 ERAS 要素。 表格列出了作为本机构加速康复外科(ERAS)通路的一部分所实施的各类加速康复要素。加粗的要素作为多中心研究 PURSUE 的一部分进行追踪。
包括早期进食、早期拔除导尿管以及早期下床活动在内的许多ERAS要素,已经在接受输尿管再植术和肾盂成形术的患者中得到实施,这标志着与以往传统做法的转变。7 尽管这些病例未必存在标准化方案,这些实践变化反映了在改进小儿泌尿外科患者术后护理方面的持续努力。
儿科阿片类药物使用
在过去的几十年里,由阿片类药物过量导致的死亡不断增加,并且在1999–2007年间,占到儿科药物过量死亡的一半。14 为应对阿片类药物危机,许多研究考察了小儿泌尿外科手术后的阿片类药物处方模式,强调不同医疗提供者之间的处方习惯存在较大变异。15,16 Garren 等 进一步指出,62%的小儿泌尿外科患者并不需要或未使用完所开具的全部阿片类药物。17 为应对阿片类药物危机,小儿泌尿外科医生一直在持续努力限制术后阿片类药物处方。
多家儿科机构已利用质量改进(QI)框架来尽量减少门诊泌尿外科手术中的阿片类药物处方。O’Kelly 等人 在 The Hospital for Sick Children 推行了一项 QI 举措,以减少接受尿道下裂修复术儿童的阿片类药物处方。该举措将处方减少了56%,且未见疼痛评分或术后结局有显著差异。18 Mittal 等人 在 Children’s Hospital of Philadelphia 实施了类似举措,以减少接受门诊儿科泌尿外科手术患者的阿片类药物处方。他们成功将处方率从43.9%降至2.3%,且患者满意度高。19 Cardona-Grau 等人 采用计划-执行-研究-行动(PDSA)模型,将儿科泌尿外科手术后的阿片类药物处方减少了50%。实施后未见疼痛评分差异。20 许多其他类似举措仍在进行中,随着各州为应对阿片危机而出台的强制性规定,这些举措的成效可能会进一步增强。21
同时,人们也在努力改进关于阿片类药物正确处置的公众教育。Garren et al 强调,78%的患者未处置剩余的阿片类药物,且仅有少数人在围手术期获得关于正确存放与处置的宣教。17 Butler et al 也指出,尽管知晓正确的处置方法,小儿泌尿外科手术后仍缺乏对阿片类药物的正确处置。他们的研究提示,医疗专业人员的宣教可能提高正确处置率,但仍需进一步的质量改进(QI)举措以更好地评估这一点。
转衔门诊
患有脊柱裂的儿童往往具有复杂的多学科医疗需求,通常由小儿泌尿科医师、骨科外科医师、神经外科医师,以及物理医学与康复科医师或发育与行为小儿科医师共同照护。随着医疗护理的进步,这一人群的预期寿命延长,因而需要将医疗照护过渡至成人专科医生。22,23 研究显示,20%的脊柱裂青少年在进行间歇性导尿时仍需要照护者的协助。24 转衔准备度与患者的健康素养相关,围绕提升这一能力的项目十分重要。25 由于多种原因,这一过渡并不总是顺利。许多患者在与成人专科建立照护关系以及在成年期管理其医疗需求方面面临问题。
尽管尚无既定指南,许多机构已设立转衔门诊,以在这一过程中为患者提供协助与指导。在达拉斯儿童医疗中心,脊柱裂患者年满18岁后,在成人泌尿科转衔门诊由泌尿科医师、护士和社会工作者接诊。该团队指出,患有神经源性膀胱的青少年在用药管理、应对医疗保险公司以及个人财务管理方面需要指导。社会工作与护理的参与对于转衔协助至关重要。26 在加拿大哈利法克斯,患者在转衔的第一年于儿科和成人泌尿科门诊间交替就诊。27 在费城儿童医院,这些患者在同一门诊空间由儿科和成人医疗提供者共同诊治,以便在熟悉且安全的环境中促进医患信任的建立。22 转衔模式多种多样,包括上述机构在内的许多机构已建立项目,以协助这一具有挑战性且复杂的过程。然而,尽管设有转衔门诊,一些中心仍报告成功转衔率出乎意料地低,这提示在这一工作中需要开展更多研究和质量改进(QI)举措。28
出血性膀胱炎
出血性膀胱炎可发生于接受盆腔放射治疗的儿童,或因化疗或骨髓移植而继发血小板减少的儿童。严重的出血性膀胱炎可导致尿潴留,从而陷入膀胱进一步扩张和血块负担增加的恶性循环。这些病例难以管理,并对患者的生活质量产生严重的负面影响。
由于尚无相关指南,对于重症病例,采取多学科管理策略可能有益。在达拉斯儿童医学中心,于2020年组建了一个由泌尿科医师、肿瘤科医师、感染病专科医师、介入放射科医师和药师组成的出血性膀胱炎工作组,以为此类病例制定分步处置方案。该院内指南目前正在制定中。
减少手术室浪费
随着医疗成本的持续上升,减少手术室中的浪费变得越来越重要。许多小儿泌尿科医师推动手术器械的标准化,以降低再处理成本。Koyle et al 对由小儿外科医生和泌尿科医生用于小儿疝的器械盘进行了标准化,将器械再处理时间减少了一半。尽管未对成本降低进行专门评估,但对外科医生和护士的调查显示,安全性、质量和效率均有所改善。29 Nast 和 Swords 将其泌尿生殖(GU)小型器械盘减少了39%,并在 Rady Children’s Hospital 将年度成本降低了$3,489.42。采用相同的方法,他们进一步修改了其他手术器械盘,估算每年的潜在节省为$14,588。30 Lurie Children’s 的泌尿科团队也使用 DMAIC 方法(定义、测量、分析、改进、控制)减少了用于腹股沟和阴茎病例的手术器械盘中的器械数量,并取得了积极结果(E. Johnson,个人通信,2021年9月29日)。
小儿泌尿外科培训中的质量改进
在小儿泌尿外科领域,强调对新晋医师进行质量改进(QI)培训的重要性。作为专科培训的一部分,小儿泌尿外科专科医师被要求完成一项机构层面的QI项目。通过这种体验式过程,他们学习QI方法学,并亲身经历克服机构实施障碍以及争取利益相关者支持的挑战。31
QI 方法学也被用于改进医学教育。Sharma 等人 实施了一项 QI 计划,以提高医务人员在评估隐睾方面的信心和专业能力。32 隐睾影响 1–3% 的足月男婴,并且是发生睾丸癌的已知危险因素。若双侧睾丸均受累,可导致生育力下降。及时诊断至关重要,但初级保健医生在诊断方面的熟练度与信心可能存在差异。作者调查了医学生、家庭医学医师、儿科医生、泌尿外科住院医师和儿科主治医师,了解其基线培训情况以及在检查隐睾方面的自信心。随后进行了一项由小儿泌尿外科医师监考的考试,并在 3 个月后进行随访问卷。该干预提高了医务人员在诊断与体格检查技能方面的信心。32 随着我们持续改进医学教育与反馈,类似研究将有助于识别学习差距并加强泌尿学培训。
基础设施
局部
随着对QI重要性的日益认可,许多机构已建立机构层面的QI和患者安全项目。QI顾问帮助医疗服务提供者设计并执行QI举措,组织主要利益相关方会议,并与信息技术专家合作,利用机构的电子病历(EMR)系统来持续推进这些工作。借助通过EMR进行的自动化数据提取,还可以更容易地开展对QI举措结果的审计。33
全国性
在全国层面,美国外科医师学会设立了国家外科质量改进计划(儿科,ACS NSQIP Peds),以更好地评估并改进儿童外科医疗服务。参与NSQIP Peds的机构提供关于30天手术结局的、经风险调整的机构级数据,可用于制定质量指标。已鼓励提高儿科泌尿外科的参与度。34
QI的方法学与途径
有多种资源可供希望进一步提升其关于质量改进(QI)方法学知识的人士使用。医疗保健改进研究所(IHI)提供线下和线上项目,并提供资质认证选项以成为经认证的患者安全专业人员。美国外科医师学会还提供一门自定进度课程,介绍QI方法的基础。多家机构为希望在该领域攻读高等学位的人士提供QI与患者安全方面的证书或硕士项目。
Squire 2.0
为质量改进工作报告提供框架,质量改进报告卓越标准(SQUIRE)指南于2008年推出。修订版(SQUIRE 2.0)于2015年发布。该指南鼓励作者阐明所要解决问题的性质与重要性,详细描述干预措施的实施过程以便他人可重复,并评估干预的影响与可持续性。35 在小儿泌尿外科领域的质量改进(QI)类出版物中,越来越鼓励遵循 SQUIRE 2.0 指南。36
改进模型与PDSA
QI实施有不同的框架。其中一种方法是由Associates in Process Improvement开发的改进模型(Model for Improvement)。37 在该框架下,团队会提出三个基本问题:确定干预的目标、界定用于评估干预效果的度量指标,以及识别为实现改进所需变更的领域。随后,通过计划-执行-研究-行动(Plan-Do-Study-Act)方法(图3)对变更或干预的效果进行测试。实施所提议的变更,并对其效果进行评估。在小范围实施干预并评估结果后,对干预进行完善,然后在更大范围内实施。37
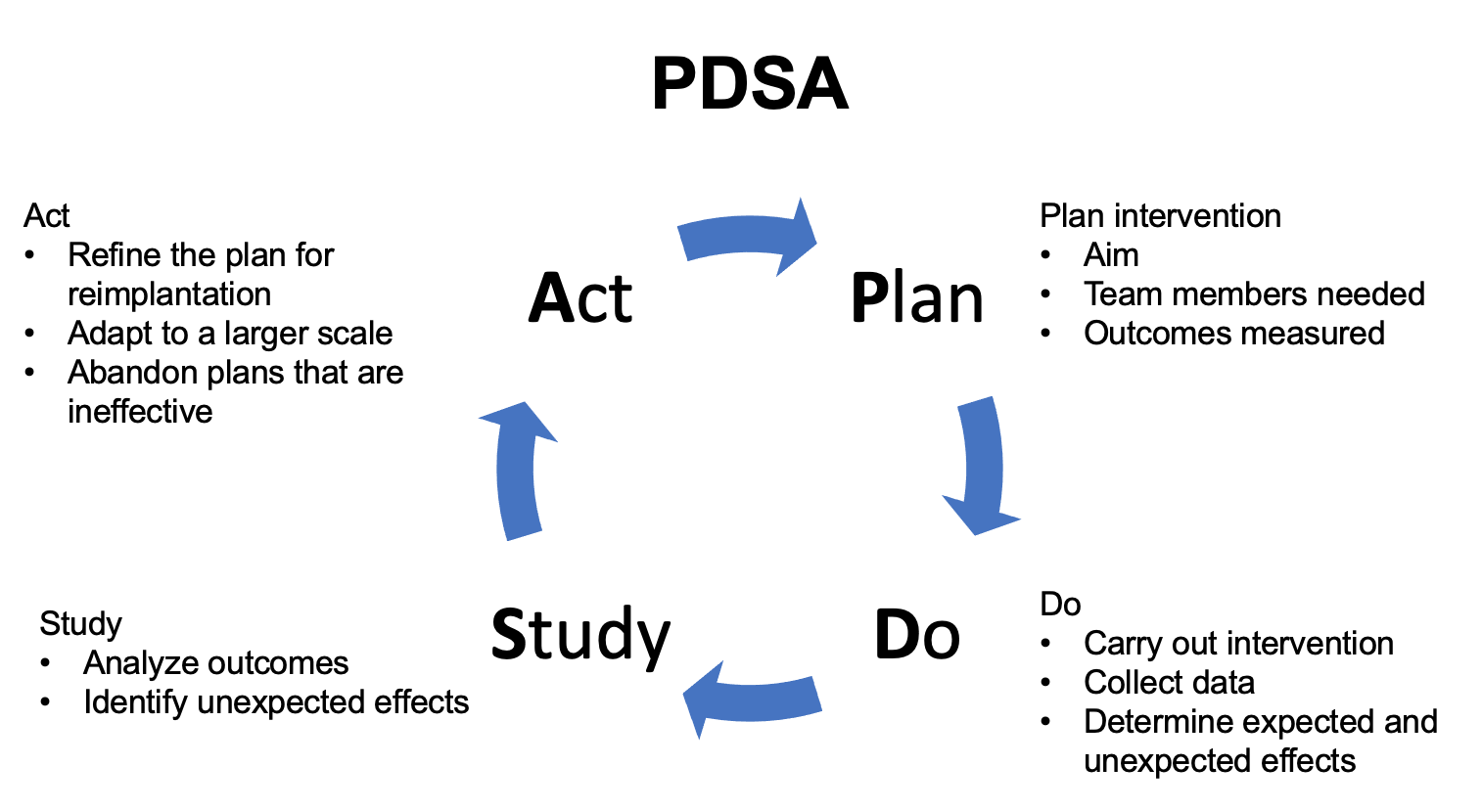
图 3 PDSA。 详述计划-执行-研究-行动(PDSA)方法的示意图。
精益六西格玛与 DMAIC
精益六西格玛结合了精益思想与六西格玛的方法。精益思想起源于日本汽车工业,侧重于减少浪费。采用这种方法,首先研究需要改进的流程,并减少浪费性的流程。38 六西格玛是一种源自制造业的、用于流程与质量改进的结构化方法。将两种方法结合称为精益六西格玛。在该框架下,团队通过五个阶段开展 QI 项目:定义、测量、分析、改进、控制(图4) 在定义阶段,确定需要解决的问题。在测量阶段收集基线数据。在分析阶段,查明问题的根本原因并实施改进措施。在控制阶段,维持已实施的变更。39
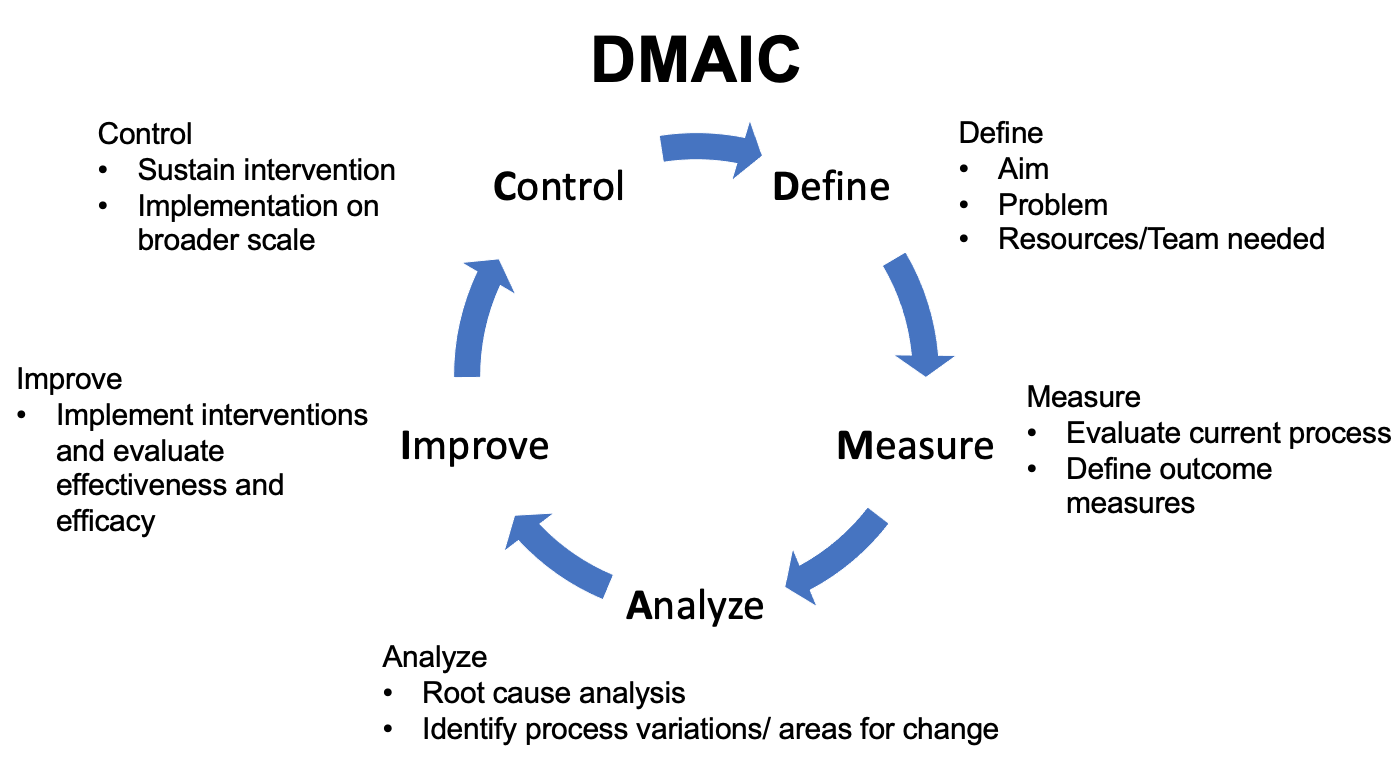
图 4 DMAIC。 详述定义-测量-分析-改进-控制方法的示意图。
未来方向
在小儿泌尿外科领域,质量改进正在获得动力,但前路仍然漫长。与标准的临床研究相比,方法学、实施过程,以及对全球性和机构层面的实施障碍的管理,对QI项目的成功尤为关键。尽管包括《Journal of Pediatric Urology》在内的期刊正在发表更多QI论文,但在泌尿外科文献中此类出版物仍然匮乏。一个面向小儿泌尿外科QI爱好者的讨论平台,可以在我们共同应对实施障碍、相互学习彼此的经验与挑战的过程中,推动项目向前发展。小儿泌尿系统疾病的相对罕见性也使得界定“质量”具有挑战性,因为用于支持最佳实践的高质量证据有限。36 然而,随着我们持续挑战教条,落实数据驱动的实践可能有助于更好地评估其有效性和安全性。作为小儿泌尿外科医师,在我们力求持续改进、推动本领域前进的过程中,我们对QI的参与和领导至关重要。
推荐阅读
- 医疗保健改进研究所
- Hannick JH, O’Kelly F, Wolfstadt JI. Improving care in pediatric urology-A primer on quality improvement methodology and how to apply it to pediatric urology. J Pediatr Urol 2019; 15: 503, DOI: 10.1016/j.jpurol.2019.09.014.
- Cohen R. I.: Lean Methodology in Health Care. Chest 2018; 154: 1448, DOI: 10.1016/j.chest.2018.06.005.
- Koning H, Verver JP, Heuvel J. Lean six sigma in healthcare. J Healthc Qual 2006; 28: 4, DOI: 10.4018/978-1-4666-7320-5.ch009.
参考文献
- Kohn LT, Corrigan JM, Washington MSD, editors. To Err is Human: Building a Safer Health System. 2000. DOI: 10.1016/s1051-0443(01)70072-3.
- Zhao LC, Lautz TB, Meeks JJ. Pediatric testicular torsion epidemiology using a national database: incidence, risk of orchiectomy and possible measures toward improving the quality of care. J Urol 2011; 186: 2009, DOI: 10.1016/j.juro.2011.07.024.
- Arevalo MK, Sheth KR, Menon VS. Straight to the Operating Room: An Emergent Surgery Track for Acute Testicular Torsion Transfers. J Pediatr 2018; 192: 178, DOI: 10.1016/j.jpeds.2017.09.009.
- Zee RS, Bayne CE, Gomella PT. Implementation of the accelerated care of torsion pathway: a quality improvement initiative for testicular torsion. J Pediatr Urol 2019; 15: 473, DOI: 10.1016/j.jpurol.2019.07.011.
- Heathcote S Sr., Duggan K, Rosbrugh J. Enhanced Recovery after Surgery (ERAS) Protocols Expanded over Multiple Service Lines Improves Patient Care and Hospital Cost. Am Surg 2019; 85: 1044, DOI: 10.1177/000313481908500951.
- Ljungqvist O, Scott M, Fearon K. C.: Enhanced Recovery After Surgery: A Review. JAMA Surg 2017; 152: 292, DOI: 10.1007/978-3-030-33443-7.
- Cain MP. Enhanced Recovery after Surgery Protocols in Pediatric Urology-How are we Doing and What Should we be Doing? J Urol 2018; 200: 952, DOI: 10.1016/j.juro.2018.08.037.
- Brindle ME, McDiarmid C, Short K. Consensus Guidelines for Perioperative Care in Neonatal Intestinal Surgery: Enhanced Recovery After Surgery (ERAS((R))) Society Recommendations. World J Surg 2020; 44: 2482, DOI: 10.1007/s00268-020-05530-1.
- Short HL, Heiss KF, Burch K. Implementation of an enhanced recovery protocol in pediatric colorectal surgery. J Pediatr Surg 2018; 53: 688, DOI: 10.1016/j.jpedsurg.2017.05.004.
- Chan YY, Rosoklija I, Meade P. Utilization of and barriers to enhanced recovery pathway implementation in pediatric urology. J Pediatr Urol 2021; 17: 294 1, DOI: 10.1016/j.jpurol.2021.01.044.
- Rove KO, Brockel MA, Saltzman AF. Prospective study of enhanced recovery after surgery protocol in children undergoing reconstructive operations. J Pediatr Urol 2018; 14: 252 1, DOI: 10.1016/j.jpurol.2018.01.001.
- Chan YY, Chu DI, Hirsch J. Implementation and sustainability of an enhanced recovery pathway in pediatric bladder reconstruction: Flexibility, commitment, teamwork. J Pediatr Urol 2021. DOI: 10.1016/j.jpurol.2021.08.023.
- Rove KO, Strine AC, Wilcox DT. Design and development of the Pediatric Urology Recovery After Surgery Endeavor (PURSUE) multicentre pilot and exploratory study. BMJ Open 2020; 10: 039035, DOI: 10.1016/j.juro.2018.02.2313.
- Kelly BC, Vuolo M, Frizzell LC. Pediatric drug overdose mortality: contextual and policy effects for children under 12 years. Pediatr Res 2021. DOI: 10.1038/s41390-021-01567-7.
- Corona LE, Roth EB, Thao A. Opioid prescribing is excessive and variable after pediatric ambulatory urologic surgery. J Pediatr Urol 2021; 17: 259 1, DOI: 10.1016/j.jpurol.2021.01.008.
- Ahn JJ, Ellison JS, Merguerian P. A.: A Societies for Pediatric Urology survey of opioid prescribing practices after ambulatory pediatric urology procedures. J Pediatr Urol 2019; 15: 451, DOI: 10.1016/j.jpurol.2019.04.025.
- Garren BR, Lawrence MB, McNaull PP. Opioid-prescribing patterns, storage, handling, and disposal in postoperative pediatric urology patients. J Pediatr Urol 2019; 15: 260 1, DOI: 10.1016/j.jpurol.2019.02.009.
- O’Kelly F, Pokarowski M, DeCotiis KN. Structured opioid-free protocol following outpatient hypospadias repair - A prospective SQUIRE 2.0-compliant quality improvement initiative. J Pediatr Urol 2020; 16: 647 1, DOI: 10.1016/j.jpurol.2020.06.012.
- Mittal S, Shukla AR, Sahadev R. Reducing post-operative opioids in children undergoing outpatient urologic surgery: A quality improvement initiative. J Pediatr Urol 2020; 16: 846 1, DOI: 10.1016/j.jpurol.2020.09.022.
- Cardona-Grau D, Bush RA, Le HK. Reducing Opioid Prescriptions in Outpatient Pediatric Urological Surgery. J Urol 2019; 201: 1012, DOI: 10.1097/ju.0000000000000020.
- Villanueva J, Pifer B, Colaco M. A government mandated consent safely reduces opioid utilization for major pediatric genitourinary surgeries. J Pediatr Surg 2021. DOI: 10.1016/j.jpedsurg.2021.01.004.
- Skokan AJ, Kovell RC. Advances and Challenges in Transitional Urology: Caring for Adolescents and Young Adults with Lifelong Complex Genitourinary Conditions. Curr Urol Rep 2018; 19: 26, DOI: 10.1007/s11934-018-0774-3.
- Hsieh MH, Wood HM, Dicianno BE. Research Needs for Effective Transition in Lifelong Care of Congenital Genitourinary Conditions: A Workshop Sponsored by the National Institute of Diabetes and Digestive and Kidney Diseases. Urology 2017; 103: 261, DOI: 10.1016/j.urology.2016.12.052.
- Chu DI, Kayle M, Stern A. Longitudinal Trajectories of Clean Intermittent Catheterization Responsibility in Youths with Spina Bifida. J Urol 2021; 101097JU0000000000002204. DOI: 10.1097/ju.0000000000002204.
- Rague JT, Kim S, Hirsch JA. Assessment of Health Literacy and Self-reported Readiness for Transition to Adult Care Among Adolescents and Young Adults With Spina Bifida. JAMA Netw Open 2021; 4: 2127034, DOI: 10.1001/jamanetworkopen.2021.27034.
- Grimsby GM, Burgess R, Culver S. Barriers to transition in young adults with neurogenic bladder. J Pediatr Urol 2016; 12: 258 1, DOI: 10.1016/j.jpurol.2016.04.015.
- Duplisea JJ, Romao RL, MacLellan DL. Urological Follow-up in Adult Spina Bifida Patients: Is There an Ideal Interval? Urology 2016; 97: 269, DOI: 10.1016/j.urology.2016.06.025.
- Szymanski KM, Cain MP, Hardacker TJ. How successful is the transition to adult urology care in spina bifida? A single center 7-year experience. J Pediatr Urol 2017; 13: 40 1, DOI: 10.1016/j.jpurol.2016.09.020.
- Koyle MA, AlQarni N, Odeh R. Reduction and standardization of surgical instruments in pediatric inguinal hernia repair. J Pediatr Urol 2018; 14: 20, DOI: 10.1016/j.jpurol.2017.08.002.
- Nast K, Swords K. A.: Decreasing operating room costs via reduction of surgical instruments. J Pediatr Urol 2019; 15: 153 1, DOI: 10.1016/j.jpurol.2019.01.013.
- Hannick JH, O’Kelly F, Wolfstadt JI. Improving care in pediatric urology-A primer on quality improvement methodology and how to apply it to pediatric urology. J Pediatr Urol 2019; 15: 503, DOI: 10.1016/j.jpurol.2019.09.014.
- Buchhalter JR, Scantlebury MH, D’Alfonso S. Creation and implementation of an electronic health record note for quality improvement in pediatric epilepsy: Practical considerations and lessons learned. Epilepsia Open 2021; 6: 345, DOI: 10.1002/epi4.12480.
- Ellison JS. Society for Pediatric Urology (SPU): NSQIP update. Societies for Pediatric Urology, Virtual. 2011.
- Ogrinc G, Davies L, Goodman D. Squire 2.0 (Standards for Quality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. Am J Crit Care 2015; 24: 466, DOI: 10.1016/s1553-7250(15)41062-1.
- O’Kelly F, Hannick JH, Wolfstadt JI. Quality improvement in pediatric urology-a historical perspective on street pumps, puerperal fever, surgical infection, and contemporary methodology. J Pediatr Urol 2019; 15: 495, DOI: 10.1016/j.jpurol.2019.08.016.
- Langley GL, R. M, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2nd ed., San Francisco, California, USA: Jossey-Bass Publishers; 2009, DOI: 10.1080/10686967.1998.11919154.
- Cohen R. I.: Lean Methodology in Health Care. Chest 2018; 154: 1448, DOI: 10.1016/j.chest.2018.06.005.
- Koning H, Verver JP, Heuvel J. Lean six sigma in healthcare. J Healthc Qual 2006; 28: 4, DOI: 10.4018/978-1-4666-7320-5.ch009.
最近更新时间: 2025-09-22 08:00